Definition/Introduction
The oculocephalic reflex (doll's eyes reflex) is an application of the vestibular-ocular reflex (VOR) used for neurologic examination of cranial nerves 3, 6, and 8, the reflex arc including brainstem nuclei, and overall gross brainstem function. It is often used to examine patients in the neurologic critical care setting and may have utility to assess neonates, anesthetized patients, or dizzy patients.[1][2][3][4][5] The reflex derives its name from the characteristic doll's eyes appearance that a patient has if the reflex is positive.[6]
The oculocephalic reflex is performed by holding a patient’s eyelids open and moving their head from side to side. The examination should only be performed on patients with a stable cervical spine without c-spine precautions. With the patient's eyelids open, the examiner briskly rotates the patient's head from side to side while the examiner observes the patient’s eyes. The examiner observes a positive oculocephalic reflex when the patient moves their eyes opposite of the rotation of their head, such that their eyes stay looking forward (like a doll’s eyes). The examiner observes a negative oculocephalic reflex when the patient’s eyes stay midline and do not move while the examiner rotates the head. A similar examination is performable for vertical eye movements.[6] Note that the designation of "positive" (eyes moving in the opposite direction of head movement indicating an intact brainstem function) or "negative" (eyes moving towards the same direction of head movement indicating severe brainstem dysfunction) doll's eyes reflex is an oversimplification and that some eye movement with nystagmus can occur in pathologic states.[7] The reflex is suppressed in a conscious adult with normal neurologic function but is active in a comatose patient with gross brainstem function, absent if there is damage to the reflex arc.[6]
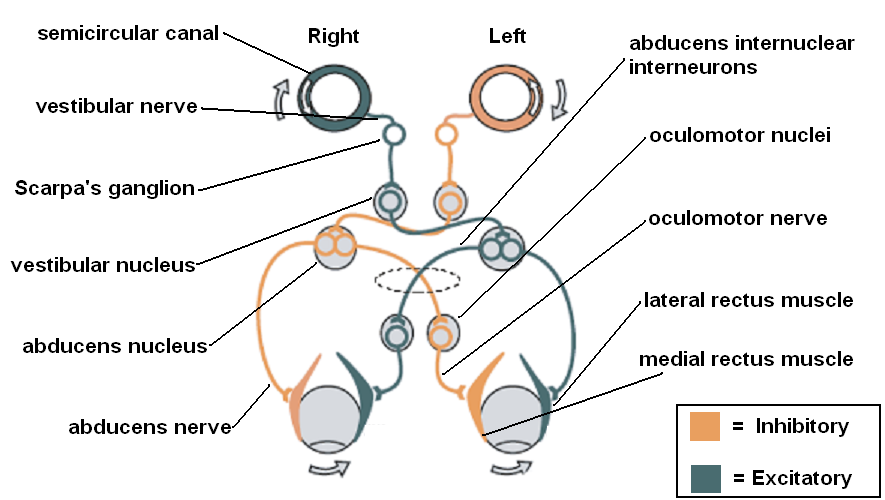
The reflex arc in the doll's eyes reflex has had extensive research. The vestibulo-ocular reflex (VOR) arc consists of a series of brainstem nuclei and the nerves connecting them as well as the vestibular system and the extra-ocular muscles of the eye. In the most simplified version of the reflex arc, angular rotation of the head causes endolymph in the horizontal semi-circular canals to rotate opposite to the direction of the head; this causes the ipsilateral vestibular nerve to activate the ipsilateral vestibular nucleus and the contralateral vestibular nerve to inhibit the contralateral vestibular nucleus. Both vestibular nuclei then activate or inhibit both abducens nuclei, which sends signals to the corresponding ipsilateral lateral rectus and contralateral oculomotor nucleus through the medial longitudinal fasciculus. The oculomotor nuclei then activate or inhibit the corresponding ipsilateral medial recti. Ultimately, the reflex gets elicited if all components of the arc are intact, and a conscious state does not suppress the reflex.[8]