Continuing Education Activity
This activity reviews the etiology, evaluation, and management of afferent loop syndrome (ALS), with particular attention to the difference in management between benign and malignant etiologies. This activity highlights the role of the interprofessional team in the diagnosis and expedient treatment of patients with this condition.
Objectives:
- Review the etiology of afferent loop syndrome.
- Outline key findings on diagnostic imaging and classic laboratory abnormalities for patients with afferent loop syndrome.
- Summarize the importance of early operative intervention for patients with afferent loop syndrome.
- Explain the importance for all members of the interprofessional team to be aware of the risk factors and presentation of afferent loop syndrome, with a focus on early recognition and surgical consultation.
Introduction
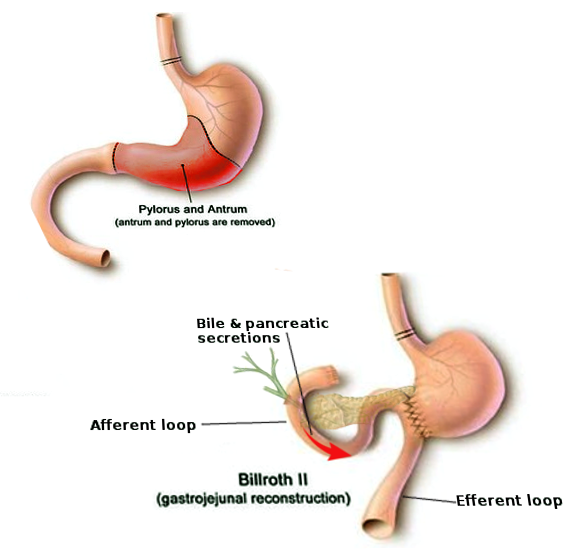
Afferent loop syndrome (ALS) is an uncommon mechanical complication that can occur after various upper gastrointestinal procedures involving anastomosis of the stomach or esophagus to the jejunum. Classically described with Billroth II gastrojejunostomy, other common procedures such as Roux-en-Y gastrojejunostomy, Roux-en-Y esophagojejunostomy, and the Whipple procedure are also associated with afferent loop syndrome.[1]
Following a Billroth II reconstruction, the afferent loop is comprised of the gastric/duodenal stump, duodenum, and the short segment of jejunum proximal to the gastrojejunostomy. Following Roux-en-Y gastric bypass, the biliopancreatic limb remains connected to the remnant stomach and is anastomosed distally via jejunojejunostomy.
The afferent limb transfers bile, pancreatic, and proximal intestinal secretions distally towards the anastomosis (gastrojejunostomy in Billroth II/Whipple procedures and jejunojejunostomy in Roux-en-Y). The efferent loop receives and transfers the ingested food and liquids. Afferent loop syndrome is defined by a distal obstruction causing distension of the afferent limb secondary to the accumulation of bile, pancreatic fluid, and proximal small bowel secretions.[2]
Etiology
Any intrinsic or extrinsic obstructive process along the afferent limb or at the distal anastomosis may result in afferent loop syndrome. Common causes include adhesions, which may result in compression or kinking of the afferent limb, internal hernia, scarring caused by previous ulceration of the gastrojejunostomy, and recurrent disease in patients who underwent surgery for cancer. Other causes may be related to intraluminal obstruction from foreign bodies, bezoars, or enteroliths.[3] Afferent loop intussusception and radiation enteritis have also been implicated.
Overall, longer afferent loops (greater than 30 to 40 cm) are more likely to volvulize or have compressive adhesions, resulting in entrapment or kinking. Retrocolic afferent loops are susceptible to internal herniation through mesocolic defects.[4]
The various etiologies of afferent loop syndrome correlate with varying degrees of acuity or chronicity and may require different management. For example, obstruction from the recurrent disease would be expected to present with chronic onset of symptoms and may have treatment with endoscopic or percutaneous decompression followed by salvage chemoradiation.[5] Alternatively, a bezoar impacted at the anastomosis will likely present with subacute to acute onset of symptoms and necessitate surgical intervention.[4]
Epidemiology
The surgical procedures associated with afferent loop syndrome have historically taken place in the treatment of gastric/duodenal ulcer disease and distal gastric cancer. With the advent and widespread availability of acid suppression medications and antibiotics for the treatment of Helicobacter pylori, fewer patients require surgical management of benign gastric disease. Thus, the overall incidence of afferent loop syndrome has declined in recent years. However, the incidence of gastric carcinoma remains high in some geographic regions, including China and Japan.[6]
With the increased prevalence of morbid obesity, recent decades have seen increased numbers of patients undergoing bariatric surgeries. Roux-en-Y gastric bypass was once the most common bariatric procedure in North America, though sleeve gastrectomy has become more common in recent years.[7][8]
Up to 1% of patients who undergo partial gastrectomy with Billroth II or Roux-en-Y reconstruction will experience afferent loop syndrome.[9] Retrospective studies have demonstrated incidence as high as 1% following laparoscopic distal gastrectomy with Billroth II reconstruction, with a lower incidence of 0.2% following open distal gastrectomy with Roux-en-Y reconstruction.[4][10][11] Overall, there is no significant difference in the risk of developing afferent loop syndrome between patients who underwent open or laparoscopic surgery.[4]
While the majority of patients present in the early postoperative period, the diagnosis should not be excluded in those with remote surgical histories. There are multiple case reports of afferent loop syndrome presenting a decade or more following gastrectomy.[3][12] There is a higher reported incidence following pancreaticoduodenectomy (Whipple), up to 13%, especially in those patients who survive three years or longer following surgery.[13]
Pathophysiology
Afferent loop syndrome occurs as a result of partial or complete obstruction of the afferent limb along its course or at the anastomosis. Symptoms are related to both the distention of the bowel as secretions accumulate and the obstruction of the pancreaticobiliary tree.[14] A complete obstruction is a closed-loop obstruction and will often present acutely with steeply increased intraluminal pressures that result in ischemia of the afferent limb. Stagnant pancreatic secretions and bile contribute to the development of pancreatitis and ascending cholangitis.[14] If severe, bowel distention and ischemia may lead to a leak at the anastomosis, perforation, and peritonitis.
Chronic afferent loop syndrome is usually related to partial obstruction. The bowel can partially decompress; however, ascending cholangitis and pancreatitis may still be seen. Additionally, stagnant secretions allow for bacterial overgrowth within the afferent limb (blind loop syndrome), presenting with symptoms of malnutrition, vitamin B12 deficiency, and steatorrhea.[4]
History and Physical
Patients with afferent loop syndrome may present with acute or chronic complaints. Most cases of acute afferent loop syndrome occur within the early postoperative period. These patients will report a sudden onset of abdominal pain, often with nausea and vomiting. There may be localized tenderness in the right upper quadrant or epigastrium and involuntary guarding. Palpation may reveal an upper abdominal mass. Jaundice may reflect biliary obstruction. Severe cases will demonstrate signs of peritonitis and septic shock.
Chronic afferent loop syndrome presents months to years after the surgery. Often, the patient will report postprandial midabdominal discomfort. Weight loss is common and multifactorial. Patients may develop an aversion to eating secondary to pain, while bacterial overgrowth may result in malabsorption.[4] Recurrent disease is also associated with weight loss. Occasionally, patients will report projectile bilious emesis followed by a relief in symptoms, which is thought to represent forceful decompression of the afferent limb with retrograde flow of the contents into the stomach and up the esophagus.[1] Physical exam findings may be similar to those seen in acute ALS, though less pronounced.
Evaluation
Acute afferent loop syndrome in the setting of complete obstruction represents a surgical emergency. Meanwhile, patients with chronic afferent loop syndrome may convert to complete obstruction, presenting with acute exacerbation of symptoms. For early diagnosis and management, clinicians must maintain a high index of suspicion when evaluating a patient with the appropriate surgical history presenting with acute abdominal pain.
While laboratory studies such as complete blood count (CBC), lactate, liver function tests (LFTs), pancreatic enzymes, and serum electrolytes are important adjuncts in evaluating the patient, abdominal imaging with computed tomography (CT) is the mainstay of diagnosis for afferent loop syndrome. An abdominal CT scan secures the diagnosis by demonstrating the obstructed loop while also providing information about the severity of bowel ischemia and the presence of complications such as perforation, pancreatitis, and inflammatory changes to the biliary tree. CT is also helpful in evaluating the underlying etiology for the obstruction, which may impact management.
Radiologists should be aware of the pathophysiology of the disease to interpret imaging findings better. Multiple signs have been described for the CT appearance of afferent loop syndrome, including the C-loop sign in the right upper quadrant, which represents the dilated afferent limb, and the keyboard sign, which describes the projection of valvulae conniventes projecting into the lumen to help differentiate the dilated bowel from pancreatic pseudocysts.[15] This loop may cross the midline, passing between the aorta and superior mesenteric artery. Magnetic resonance cholangiopancreatography (MRCP) provides similar information and may be considered in patients for whom the risk of iodinated contrast or ionizing radiation outweighs the need for the expedience of CT imaging. MRCP may also be a helpful adjunct to CT in elucidating the underlying etiology for patients with subacute to a chronic presentation.[16]
When interpreting abdominal imaging on these patients, presence of pancreaticobiliary tract dilation, focal non-enhancement of the pancreas or peripancreatic edema, mass or wall thickening involving the anastomosis, and evidence of metastatic disease (lymphadenopathy, peritoneal nodules, ascites, distant metastatic lesions) should be noted. Adhesions are implicated when a discrete transition point is seen without another underlying cause. The presence of intraperitoneal air in the immediate post-operative patient is expected; however, if persistent or increasing air is noted or if it is seen more than 10 days following surgery in the setting of afferent loop syndrome, perforation of the afferent limb should be suspected.[6] Clinically a patient will usually present with other signs of a perforation or a leak before 10 days, such as persistent tachycardia of greater than 120 bpm, fever, and abdominal pain.
Abdominal radiographs are often normal, except in the setting of gross pneumoperitoneum or with a long segment, dilated afferent loop. Ultrasound and fluoroscopic upper GI barium studies have largely been replaced with CT imaging in acutely ill patients with concern for afferent loop syndrome. In the early postoperative period, the leading differential consideration is an anastomotic leak, and these patients often undergo fluoroscopic upper GI before cross-sectional imaging. Findings associated with afferent loop syndrome on fluoroscopic upper GI include failure of contrast to enter the afferent limb, though this is a nonspecific finding. Alternately, preferential filling of the afferent limb of a gastrojejunostomy (Billroth II reconstruction and Whipple) with retention of contrast may also suggest the diagnosis.[15]
Treatment / Management
Management for patients with afferent loop syndrome can largely subdivide according to underlying etiology. For most benign causes, surgery usually provides definitive treatment. In the setting of malignancy, initial neoadjuvant management may be followed by surgical treatment with curative/palliative intent.[4][9] Nasogastric tube drainage may provide temporary relief of symptoms while the patient is resuscitated for surgery. At least one retrospective study evaluated the efficacy of endoscopic placement of a nasogastric tube into the afferent limb as both a temporizing measure before surgery and as a conservative treatment for patients with benign ALS due to non-obstructive causes such as mucosal edema.[9] Patients with chronic afferent loop syndrome may benefit from preoperative nutritional support and blood transfusions to decrease surgical complications. Antibiotics are an option to treat bacterial overgrowth contributing to malnutrition.
The nature of intervention for afferent loop syndrome secondary to benign causes depends on the original surgery performed and the underlying cause of obstruction. Various corrective surgical procedures have been described, including:
- Converting a Billroth II to a Roux-en-Y
- Creating a Braun anastomosis in a Billroth II, which is an anastomosis from the afferent limb directly to the efferent limb allowing secretions to bypass the gastrojejunal anastomosis[1]
- Redundant loops may be excised and reconstructed.
Obstructions that involve the supramesocolic portion of the afferent loop are often more technically complex to fix due to the dense adhesions that form in the region. Of the benign causes for afferent loop syndrome, anastomotic scarring from a healed marginal ulcer may receive management by endoscopic balloon dilation.[4] Patients who are not strong surgical candidates may benefit from the endoscopic ultrasound-guided creation of a gastrojejunostomy using a biflanged lumen apposing metal stent. Early multicenter reports on these procedures show them to have high technical and clinical success rates.[17]
Patients with acute afferent loop syndrome due to malignant causes that are deemed non-operative should undergo palliative treatment targeted at relieving the acute obstruction. Excision and reconstruction are not typically performed in the acute setting for these patients.[4] Examples include endoscopic balloon dilation and endoscopic or percutaneous placement of stents and/or drains. For patients who have undergone pancreaticoduodenectomy (Whipple), additional considerations in acute management include patency of the hepaticojejunostomy and pancreaticojejunostomy. Failure to address concurrent obstruction at the time of intervention for afferent loop syndrome is expected to result in worse patient outcomes.
Differential Diagnosis
Abdominal surgeries associated with afferent loop syndrome are relatively more complex procedures and can cause multiple early and late complications. During the early postoperative period, abdominal pain and nausea are both nonspecific and relatively common. In addition to ALS, clinicians should consider postoperative ileus, anastomotic leak, transient partial obstruction at the anastomosis secondary to edema/inflammation, bile reflux, acute iatrogenic pancreatitis, and postoperative fluid collections. Nausea and vomiting may be related to analgesia or metabolic disturbances. Patients reporting severe abdominal pain or progressive symptoms should undergo imaging evaluation. Chronic ALS presents with likewise non-specific symptoms that may present with internal hernias and adhesions without obstruction, mesenteric ischemia, small bowel bacterial overgrowth, chronic pancreatitis, biliary colic, and gallstone-related disease.
Prognosis
Except in advanced or recurrent malignancy cases, the prognosis is good for patients who receive a prompt diagnosis and undergo surgery. The mortality rate for delayed diagnosis is variably reported between 30% to 60%, with poor outcomes for those patients who suffer perforation of the afferent limb, with subsequent peritonitis and shock.[12]
Complications
When afferent loop syndrome presents acutely, the major cause of mortality is sepsis, which leads to multiorgan failure. Even when intervention occurs before the development of peritonitis and systemic infection, these patients are at increased risk for other periprocedural complications, especially if the initial surgery was for the treatment of malignancy. Patients who have an acute-on-chronic presentation may also experience an increased rate of complications due to malnutrition and anemia. Examples of complications for which these patients experience increased risk include anastomotic leak, recurrent adhesions or strictures, fistula formation, wound infection and dehiscence, deep venous thrombosis, pulmonary embolism, and aspiration on the induction of anesthesia.
Postoperative and Rehabilitation Care
Management in the immediate postoperative period is similar to any other upper gastrointestinal surgery. The patient should remain NPO (nothing by mouth), have maintenance IV fluids, and have adequate analgesia. A nasogastric or nasoenteric tube is often necessary for decompression. The patient should be out of bed early and often, with chemical and mechanical deep venous thrombosis prophylaxis, as appropriate. A diet is slowly progressed from a clear liquid diet to soft food and then to solid food. Any subsequent dietary modifications should take into account the specific clinical scenario, including the operation performed, with the involvement of a trained and experienced nutritionist, if available.
Consultations
In the acute setting, early surgical consultation is mandatory as a delay in diagnosis and intervention is life-threatening. Gastroenterology can assist with palliative/endoscopic management for select patients, and Interventional Radiology may be necessary for percutaneous intervention. In the chronic or subacute setting, when intervention can sustain delay for nutritional and medical optimization, hematology and nutritional medicine are meaningful consultations to consider.
Deterrence and Patient Education
Although rare, patients undergoing Billroth II, Roux-en-Y, pancreaticoduodenectomy, and related procedures should receive counsel on the risk of afferent loop syndrome before surgery. These patients should be directed to seek emergent care should they develop symptoms of acute afferent loop syndrome.
Enhancing Healthcare Team Outcomes
Effective teamwork at all levels can improve the patient outcome in afferent loop syndrome. Primary care and frontline providers evaluating patients at risk for afferent loop syndrome should consider early surgical consultation and work closely with diagnostic radiologists to perform the appropriate diagnostic imaging and improve interpretation. An interprofessional approach is encouraged with the patient care team, including an interventional radiologist, endoscopist, hematologist, and nutritionist, along with the surgical specialist as well as specialty trained nurses. Perianesthesia and operating room nurses will provide surgical prep and intra- and post-surgical care. In cases requiring nutritional stabilization, nursing can work closely with nutritional support (nutrition doctor, nutritionist) to assist with patient monitoring and compliance. The pharmacy can assist with postoperative pain management. This interprofessional approach can prevent unnecessary delays in the diagnosis of afferent loop syndrome, ensure adequate surgical disposition based on underlying etiology, and also helps to optimize the patient before surgery, helping to increase the likelihood of a good surgical outcome. [Level 5]