Introduction
If you are smiling right now, you are likely engaging the risorius muscle – that is, if you even have a risorius muscle. Commonly known as the smiling muscle, it serves as a muscle of facial expression. As alluded to here, it is not present in all people, and it is believed to be unique only to the Hominines, or the African great apes and humans, evolving in our common ancestor.[1]
Structure and Function
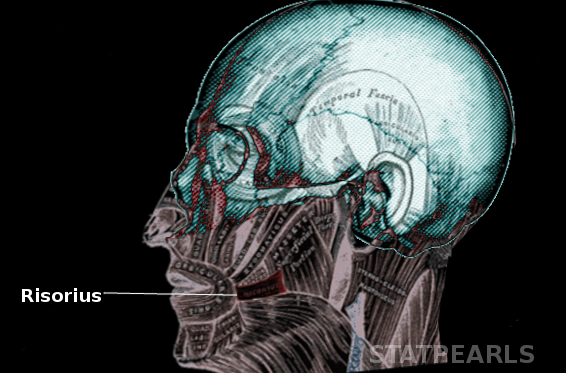
The risorius muscle is a narrow bundle of muscle fibers that becomes narrower from its origin at the fascia of the lateral cheek over the parotid gland and superficial masseter and platysma muscles, to its insertion onto the skin of the angle of the mouth. There is a risorius muscle located on either side of the lips in most individuals. Like other facial muscles, the risorius has a greater percentage of slow muscle fibers and contains a more intricate configuration of innervation of extrafusal fibers than other skeletal muscles throughout the body. Its location is within the deep portion of the superficial musculoaponeurotic system (SMAS),[2] a fibrous network containing the facial muscles, that is continuous with the temporoparietal fascia and galea and extends from the galea aponeurotica and the platysma. Vertical septa connect the SMAS to the dermis. The risorius muscle’s function is to aid in facial expression by pulling the corner of the mouth laterally via its contraction in an outward and upward motion. In conjunction with other facial muscles, this helps to create a smile or a frown, and myriad other expressions in-between.
Embryology
The risorius muscle, along with its arterial supply, arises from the second pharyngeal arch mesoderm, which forms approximately during the fourth week of gestation. The motor and sensory innervation to the risorius come from the facial and trigeminal nerves, respectively, which arise from the neural crest cells, as do the mandible bone and the connective tissue upon which the risorius lies.
Blood Supply and Lymphatics
The risorius muscle receives its arterial blood supply via the facial artery and the transverse facial artery at its origin. The facial artery is a branch of the external carotid artery and gives rise to the submental and inferior and superior labial arteries, supplying the chin and lip regions, and proceeds superomedially to the lateral aspect of the nose as the angular artery. Proximally, it passes anterosuperiorly over the mandible and is deep to the risorius. The transverse facial artery arises from the superficial temporal artery just inferior to the zygomatic arch of the temporal bone, where it courses anteriorly down the mandible between the superficial and deep masseter muscles.
The facial and transverse facial veins drain deoxygenated blood from the risorius. The facial vein drains into the common facial vein, then into the internal jugular vein. The transverse facial vein drains into the retromandibular vein, which then drains into the external jugular vein via the posterior branch of the retromandibular vein, or to the internal jugular vein via the anterior branch of the retromandibular vein and the common facial vein. The submandibular and mandibular lymph nodes receive lymph drainage from the risorius.
Nerves
The risorius muscle is innervated, like all muscles of facial expression, by the facial nerve, to which it is directly connected. There is debate over which branch of the facial nerve actually innervates the risorius, but most agree that it is either one of the buccal branches or the marginal mandibular branch, and it may receive motor innervation from both. The buccal branches of the facial nerve arise from the facial nerve deep to the parotid gland and just posterior to the superficial and deep masseter muscles upon which it sits and has branches that flank the risorius muscle on its superior and inferior aspects. The marginal mandibular branch of the facial nerve is a tributary from the facial nerve just distal to the most distal buccal branch, and courses down the angle of the jaw and along the posterior aspect of the mandible. Sensory innervation of the cheek come from the buccal nerve, a branch of the anterior division of the mandibular branch of the trigeminal nerve via general somatic afferent fibers.
Muscles
The risorius muscle sits atop the orbicularis oris and the depressor anguli oris at its most anterior aspect and is superficial to the superficial masseter muscle at its posterior portion. There are spaces on the superior and inferior aspects of the muscle. The inferior space is rectangular with its borders comprised of the superficial masseter posteriorly, the platysma inferiorly, the depressor anguli oris anteriorly, and the risorius superiorly. This inferior rectangular space contains a buccal branch of the facial nerve, as well as the facial artery and vein anteriorly. The mandible is deep to this space. The superior triangular space is comprised of the superficial masseter posteriorly, the risorius inferiorly, and the zygomaticus major muscle makes up the hypotenuse. Deep to this space is the buccinator artery, vein, and nerves, all of which sit atop the buccinator muscle.
Physiologic Variants
There is significant variation among individuals regarding bilateral symmetry, asymmetry, or the presence of the risorius.[3]
Surgical Considerations
In plastic surgery, the superficial muscular aponeurotic system (SMAS), which contains the risorius muscle, is manipulated during cosmetic surgeries of the face, such as rhytidectomies (facelifts). Removal of excess facial skin along with tightening of the underlying tissues (SMAS) helps to create a more youthful appearance. Facelift surgery was the sixth most popular cosmetic surgery in 2011 according to the American Society for Aesthetic Plastic Surgery.
Clinical Significance
In Bell palsy, a condition caused by a facial nerve deficit characterized by paresis or paralysis of the muscles it innervates, the risorius may be affected with other muscles of facial expression. This condition generally receives treatment with oral steroids, with no clinically meaningful difference in outcomes between high-dose vs. moderate or low dose steroids.[4] Sometimes, clinicians may add an antiviral such as valacyclovir, and although steroid and antiviral treatment is controversial, an antiviral alone has shown no benefit when compared to placebo. Some cases may warrant physical therapy. Bell palsy may present similarly to stroke, Lyme disease, and tumors, so workup may include ruling out these other causes of facial paralysis.