[1]
Singh D, Agusti A, Anzueto A, Barnes PJ, Bourbeau J, Celli BR, Criner GJ, Frith P, Halpin DMG, Han M, López Varela MV, Martinez F, Montes de Oca M, Papi A, Pavord ID, Roche N, Sin DD, Stockley R, Vestbo J, Wedzicha JA, Vogelmeier C. Global Strategy for the Diagnosis, Management, and Prevention of Chronic Obstructive Lung Disease: the GOLD science committee report 2019. The European respiratory journal. 2019 May:53(5):. pii: 1900164. doi: 10.1183/13993003.00164-2019. Epub 2019 May 18
[PubMed PMID: 30846476]
[2]
GBD 2015 Chronic Respiratory Disease Collaborators. Global, regional, and national deaths, prevalence, disability-adjusted life years, and years lived with disability for chronic obstructive pulmonary disease and asthma, 1990-2015: a systematic analysis for the Global Burden of Disease Study 2015. The Lancet. Respiratory medicine. 2017 Sep:5(9):691-706. doi: 10.1016/S2213-2600(17)30293-X. Epub 2017 Aug 16
[PubMed PMID: 28822787]
Level 1 (high-level) evidence
[3]
Stockley RA. Neutrophils and protease/antiprotease imbalance. American journal of respiratory and critical care medicine. 1999 Nov:160(5 Pt 2):S49-52
[PubMed PMID: 10556170]
[4]
Parker CM, Voduc N, Aaron SD, Webb KA, O'Donnell DE. Physiological changes during symptom recovery from moderate exacerbations of COPD. The European respiratory journal. 2005 Sep:26(3):420-8
[PubMed PMID: 16135722]
[5]
Mattos WL, Signori LG, Borges FK, Bergamin JA, Machado V. Accuracy of clinical examination findings in the diagnosis of COPD. Jornal brasileiro de pneumologia : publicacao oficial da Sociedade Brasileira de Pneumologia e Tisilogia. 2009 May:35(5):404-8
[PubMed PMID: 19547847]
[6]
Changizi M, Rio K. Harnessing color vision for visual oximetry in central cyanosis. Medical hypotheses. 2010 Jan:74(1):87-91. doi: 10.1016/j.mehy.2009.07.045. Epub 2009 Aug 21
[PubMed PMID: 19699589]
[7]
Qaseem A, Wilt TJ, Weinberger SE, Hanania NA, Criner G, van der Molen T, Marciniuk DD, Denberg T, Schünemann H, Wedzicha W, MacDonald R, Shekelle P, American College of Physicians, American College of Chest Physicians, American Thoracic Society, European Respiratory Society. Diagnosis and management of stable chronic obstructive pulmonary disease: a clinical practice guideline update from the American College of Physicians, American College of Chest Physicians, American Thoracic Society, and European Respiratory Society. Annals of internal medicine. 2011 Aug 2:155(3):179-91. doi: 10.7326/0003-4819-155-3-201108020-00008. Epub
[PubMed PMID: 21810710]
Level 1 (high-level) evidence
[8]
Decramer M, Janssens W, Miravitlles M. Chronic obstructive pulmonary disease. Lancet (London, England). 2012 Apr 7:379(9823):1341-51. doi: 10.1016/S0140-6736(11)60968-9. Epub 2012 Feb 6
[PubMed PMID: 22314182]
[9]
FLETCHER CM, ELMES PC, FAIRBAIRN AS, WOOD CH. The significance of respiratory symptoms and the diagnosis of chronic bronchitis in a working population. British medical journal. 1959 Aug 29:2(5147):257-66
[PubMed PMID: 13823475]
[10]
ATS Committee on Proficiency Standards for Clinical Pulmonary Function Laboratories. ATS statement: guidelines for the six-minute walk test. American journal of respiratory and critical care medicine. 2002 Jul 1:166(1):111-7
[PubMed PMID: 12091180]
[11]
Shaker SB, Dirksen A, Bach KS, Mortensen J. Imaging in chronic obstructive pulmonary disease. COPD. 2007 Jun:4(2):143-61
[PubMed PMID: 17530508]
[12]
Anthonisen NR, Manfreda J, Warren CP, Hershfield ES, Harding GK, Nelson NA. Antibiotic therapy in exacerbations of chronic obstructive pulmonary disease. Annals of internal medicine. 1987 Feb:106(2):196-204
[PubMed PMID: 3492164]
[13]
Melani AS. Long-acting muscarinic antagonists. Expert review of clinical pharmacology. 2015:8(4):479-501. doi: 10.1586/17512433.2015.1058154. Epub
[PubMed PMID: 26109098]
[14]
Ram FS, Jones PW, Castro AA, De Brito JA, Atallah AN, Lacasse Y, Mazzini R, Goldstein R, Cendon S. Oral theophylline for chronic obstructive pulmonary disease. The Cochrane database of systematic reviews. 2002:2002(4):CD003902
[PubMed PMID: 12519617]
Level 1 (high-level) evidence
[15]
ZuWallack RL, Mahler DA, Reilly D, Church N, Emmett A, Rickard K, Knobil K. Salmeterol plus theophylline combination therapy in the treatment of COPD. Chest. 2001 Jun:119(6):1661-70
[PubMed PMID: 11399688]
[16]
Nannini LJ, Lasserson TJ, Poole P. Combined corticosteroid and long-acting beta(2)-agonist in one inhaler versus long-acting beta(2)-agonists for chronic obstructive pulmonary disease. The Cochrane database of systematic reviews. 2012 Sep 12:2012(9):CD006829. doi: 10.1002/14651858.CD006829.pub2. Epub 2012 Sep 12
[PubMed PMID: 22972099]
Level 1 (high-level) evidence
[17]
Nannini LJ, Poole P, Milan SJ, Kesterton A. Combined corticosteroid and long-acting beta(2)-agonist in one inhaler versus inhaled corticosteroids alone for chronic obstructive pulmonary disease. The Cochrane database of systematic reviews. 2013 Aug 30:2013(8):CD006826. doi: 10.1002/14651858.CD006826.pub2. Epub 2013 Aug 30
[PubMed PMID: 23990350]
Level 1 (high-level) evidence
[18]
Rabe KF. Update on roflumilast, a phosphodiesterase 4 inhibitor for the treatment of chronic obstructive pulmonary disease. British journal of pharmacology. 2011 May:163(1):53-67. doi: 10.1111/j.1476-5381.2011.01218.x. Epub
[PubMed PMID: 21232047]
[19]
Calverley PM, Rabe KF, Goehring UM, Kristiansen S, Fabbri LM, Martinez FJ, M2-124 and M2-125 study groups. Roflumilast in symptomatic chronic obstructive pulmonary disease: two randomised clinical trials. Lancet (London, England). 2009 Aug 29:374(9691):685-94. doi: 10.1016/S0140-6736(09)61255-1. Epub
[PubMed PMID: 19716960]
Level 1 (high-level) evidence
[20]
Uzun S, Djamin RS, Kluytmans JA, Mulder PG, van't Veer NE, Ermens AA, Pelle AJ, Hoogsteden HC, Aerts JG, van der Eerden MM. Azithromycin maintenance treatment in patients with frequent exacerbations of chronic obstructive pulmonary disease (COLUMBUS): a randomised, double-blind, placebo-controlled trial. The Lancet. Respiratory medicine. 2014 May:2(5):361-8. doi: 10.1016/S2213-2600(14)70019-0. Epub 2014 Apr 15
[PubMed PMID: 24746000]
Level 1 (high-level) evidence
[21]
Albert RK, Connett J, Bailey WC, Casaburi R, Cooper JA Jr, Criner GJ, Curtis JL, Dransfield MT, Han MK, Lazarus SC, Make B, Marchetti N, Martinez FJ, Madinger NE, McEvoy C, Niewoehner DE, Porsasz J, Price CS, Reilly J, Scanlon PD, Sciurba FC, Scharf SM, Washko GR, Woodruff PG, Anthonisen NR, COPD Clinical Research Network. Azithromycin for prevention of exacerbations of COPD. The New England journal of medicine. 2011 Aug 25:365(8):689-98. doi: 10.1056/NEJMoa1104623. Epub
[PubMed PMID: 21864166]
[22]
de Jong YP, Uil SM, Grotjohan HP, Postma DS, Kerstjens HA, van den Berg JW. Oral or IV prednisolone in the treatment of COPD exacerbations: a randomized, controlled, double-blind study. Chest. 2007 Dec:132(6):1741-7
[PubMed PMID: 17646228]
Level 1 (high-level) evidence
[23]
McCarthy B, Casey D, Devane D, Murphy K, Murphy E, Lacasse Y. Pulmonary rehabilitation for chronic obstructive pulmonary disease. The Cochrane database of systematic reviews. 2015 Feb 23:2015(2):CD003793. doi: 10.1002/14651858.CD003793.pub3. Epub 2015 Feb 23
[PubMed PMID: 25705944]
Level 3 (low-level) evidence
[24]
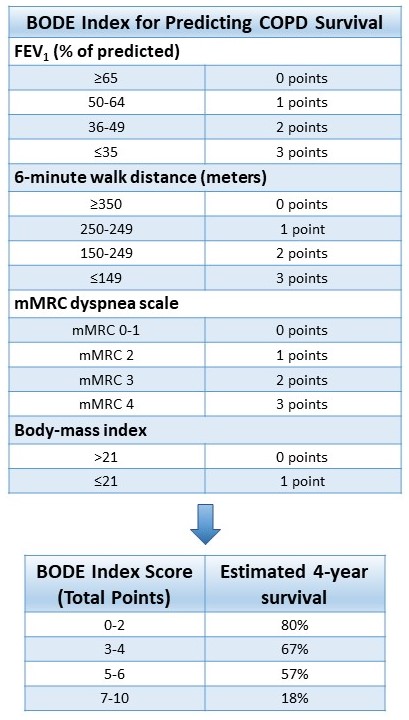
Celli BR, Cote CG, Marin JM, Casanova C, Montes de Oca M, Mendez RA, Pinto Plata V, Cabral HJ. The body-mass index, airflow obstruction, dyspnea, and exercise capacity index in chronic obstructive pulmonary disease. The New England journal of medicine. 2004 Mar 4:350(10):1005-12
[PubMed PMID: 14999112]
[25]
Tanoue LT, Tanner NT, Gould MK, Silvestri GA. Lung cancer screening. American journal of respiratory and critical care medicine. 2015 Jan 1:191(1):19-33. doi: 10.1164/rccm.201410-1777CI. Epub
[PubMed PMID: 25369325]