[1]
Sapundzhiev N,Werner JA, Nasal snuff: historical review and health related aspects. The Journal of laryngology and otology. 2003 Sep
[PubMed PMID: 14561353]
[2]
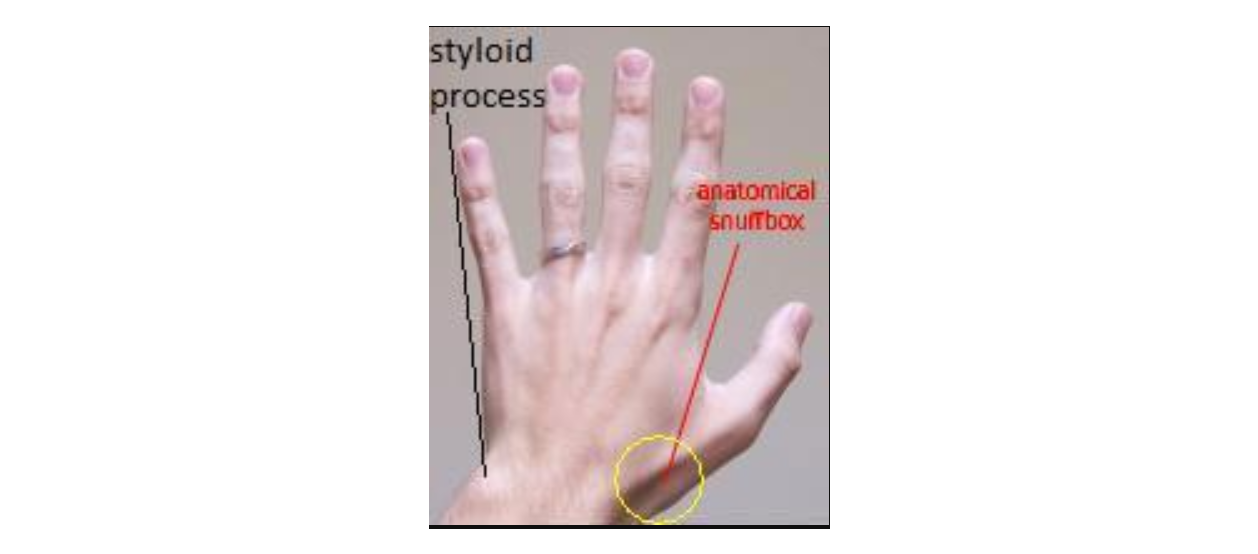
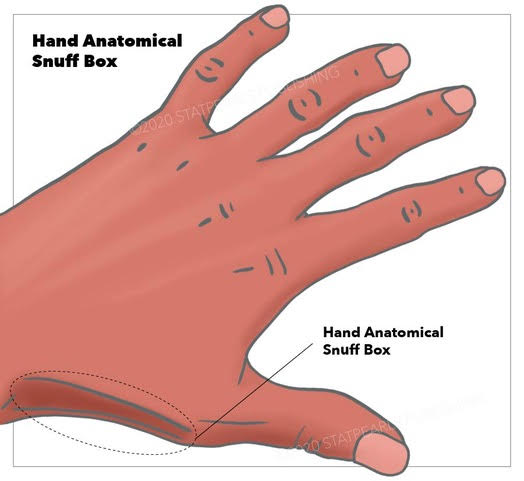
It's time to snuff out the "anatomical snuff box"., Seidenberg AB,Halperin EC,Goldstein AO,, Academic medicine : journal of the Association of American Medical Colleges, 2015 Aug
[PubMed PMID: 26218360]
[4]
Strauch RJ,Strauch CB, Extensor pollicis brevis tendon can hyperextend thumb interphalangeal joint in absence of extensor pollicis longus: Case report and review of the literature. World journal of orthopedics. 2016 Jul 18
[PubMed PMID: 27458556]
Level 3 (low-level) evidence
[5]
Shigematsu S,Shimizu H,Beppu M,Hirata K, Anatomy of the extensor pollicis brevis associated with an extension mechanism of the thumb metacarpophalangeal joint. Hand surgery : an international journal devoted to hand and upper limb surgery and related research : journal of the Asia-Pacific Federation of Societies for Surgery of the Hand. 2014;
[PubMed PMID: 24875499]
[6]
Roh JH,Lee JH, Distal Radial Approach through the Anatomical Snuff Box for Coronary Angiography and Percutaneous Coronary Intervention. Korean circulation journal. 2018 Dec
[PubMed PMID: 30403016]
[8]
The vascularity of the scaphoid bone., Gelberman RH,Menon J,, The Journal of hand surgery, 1980 Sep
[PubMed PMID: 7430591]
[9]
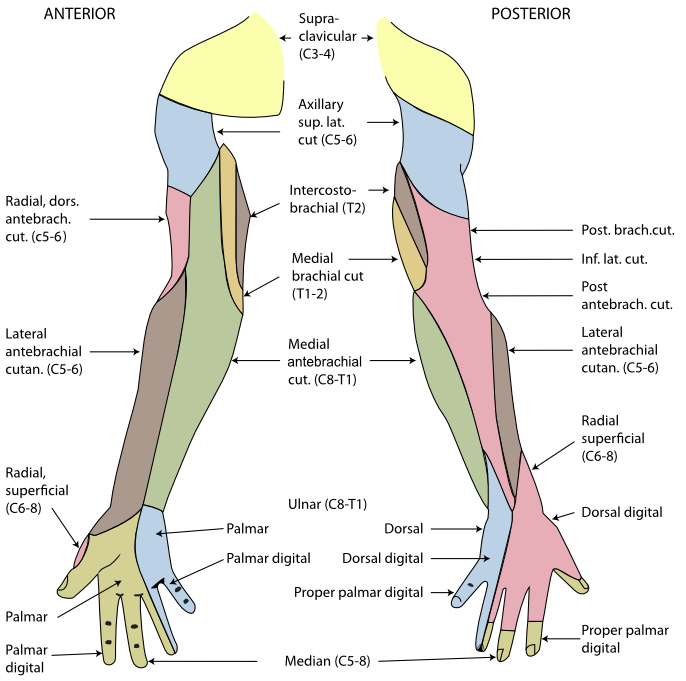
Applied anatomy of the superficial branch of the radial nerve., Robson AJ,See MS,Ellis H,, Clinical anatomy (New York, N.Y.), 2008 Jan
[PubMed PMID: 18092362]
[10]
Gurses IA,Coskun O,Gayretli O,Kale A,Ozturk A, The relationship of the superficial radial nerve and its branch to the thumb to the first extensor compartment. The Journal of hand surgery. 2014 Mar
[PubMed PMID: 24495622]
[11]
Öztürk K,Dursun A,Kastamoni Y,Albay S, Anatomical variations of the extensor tendons of the fetal thumb. Surgical and radiologic anatomy : SRA. 2021 May
[PubMed PMID: 33170332]
[12]
Sugiura S,Matsuura Y,Suzuki T,Nishikawa S,Mori C,Kuniyoshi K, Variant course of extensor pollicis brevis tendon in the third extensor compartment. Surgical and radiologic anatomy : SRA. 2018 Mar;
[PubMed PMID: 29138875]
[13]
Tendinopathies of the Hand and Wrist., Adams JE,Habbu R,, The Journal of the American Academy of Orthopaedic Surgeons, 2015 Dec
[PubMed PMID: 26510626]
[14]
Multiple variations of the tendons of the anatomical snuffbox., Thwin SS,Fazlin F,Than M,, Singapore medical journal, 2014 Jan
[PubMed PMID: 24452976]
[15]
Unintentional arterial puncture during cephalic vein cannulation: case report and anatomical study., Lirk P,Keller C,Colvin J,Colvin H,Rieder J,Maurer H,Moriggl B,, British journal of anaesthesia, 2004 May
[PubMed PMID: 15003983]
Level 3 (low-level) evidence
[16]
Pua U,Quek LHH, "Snuffbox" Distal Radial Access. Journal of vascular and interventional radiology : JVIR. 2018 Jan
[PubMed PMID: 29258662]
[17]
Kiemeneij F, Left distal transradial access in the anatomical snuffbox for coronary angiography (ldTRA) and interventions (ldTRI). EuroIntervention : journal of EuroPCR in collaboration with the Working Group on Interventional Cardiology of the European Society of Cardiology. 2017 Sep 20
[PubMed PMID: 28506941]
[18]
Kim Y,Ahn Y,Kim I,Lee DH,Kim MC,Sim DS,Hong YJ,Kim JH,Jeong MH, Feasibility of Coronary Angiography and Percutaneous Coronary Intervention via Left Snuffbox Approach. Korean circulation journal. 2018 Dec
[PubMed PMID: 30088362]
Level 2 (mid-level) evidence
[19]
Ko JH,Pet MA,Khouri JS,Hammert WC, Management of Scaphoid Fractures. Plastic and reconstructive surgery. 2017 Aug;
[PubMed PMID: 28746289]
[20]
Cohen A,Reijman M,Kraan GA,Mathijssen NMC,Koopmanschap MA,Verhaar JAN,Mol S,Colaris JW,SUSPECT study group, Clinically SUspected ScaPhoid fracturE: treatment with supportive bandage or CasT? 'Study protocol of a multicenter randomized controlled trial' (SUSPECT study). BMJ open. 2020 Sep 29
[PubMed PMID: 32994236]
Level 1 (high-level) evidence
[21]
Li H,Guo W,Guo S,Zhao S,Li R, Surgical versus nonsurgical treatment for scaphoid waist fracture with slight or no displacement: A meta-analysis and systematic review. Medicine. 2018 Nov
[PubMed PMID: 30508914]
Level 1 (high-level) evidence
[22]
Tenosynovitis caused by texting: an emerging disease., Ashurst JV,Turco DA,Lieb BE,, The Journal of the American Osteopathic Association, 2010 May
[PubMed PMID: 20538752]