Introduction
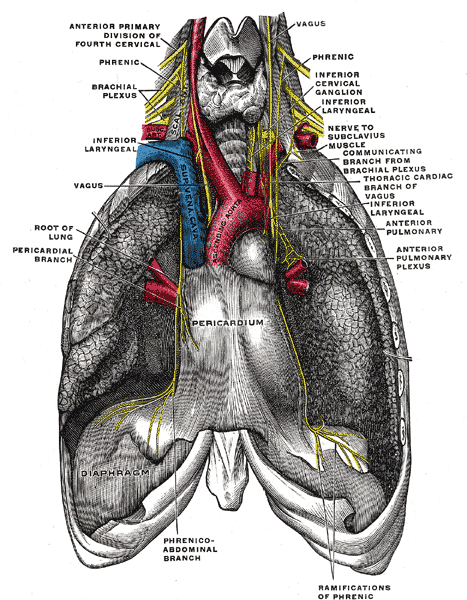
The phrenic nerve originates from the anterior rami of C3 through C5 and traverses the neck, heart, and lungs to reach the diaphragm. From its origin, the phrenic nerve descends vertically caudad and adjacent to the internal jugular vein. In the neck and upper thorax, the left phrenic nerve tracts proximal to the subclavian artery. The right phrenic nerve runs superficial to the anterior scalene muscle and the second part of the right subclavian artery. In the thorax, the right and left phrenic nerve will continue to descend anteriorly to the root of the lung and between the mediastinal surface of the parietal pleura and fibrous pericardium. The right phrenic nerve passes lateral to the right atrium and right ventricle and will continue to descend through the vena cava hiatus in the diaphragmatic opening at the level of T8. The left phrenic nerve descends anterior to the pericardial sac of the left ventricle and terminates at the central tendon of the diaphragm.[1][2][3]