Introduction
There are many muscles in the neck. One of the classifications of the muscles of the neck is relative to the hyoid bone. Those muscles which are above the hyoid bone are termed as supra-hyoid muscles, and those below it are called infra-hyoid muscles. This group of muscles participates in the processes of chewing, swallowing, and phonetics. Moreover, together with the infrahyoid muscles, they contribute to the fixation of the hyoid bone, which does not articulate with any other bone. The suprahyoid muscles participate in improving the flexion movement of the neck.
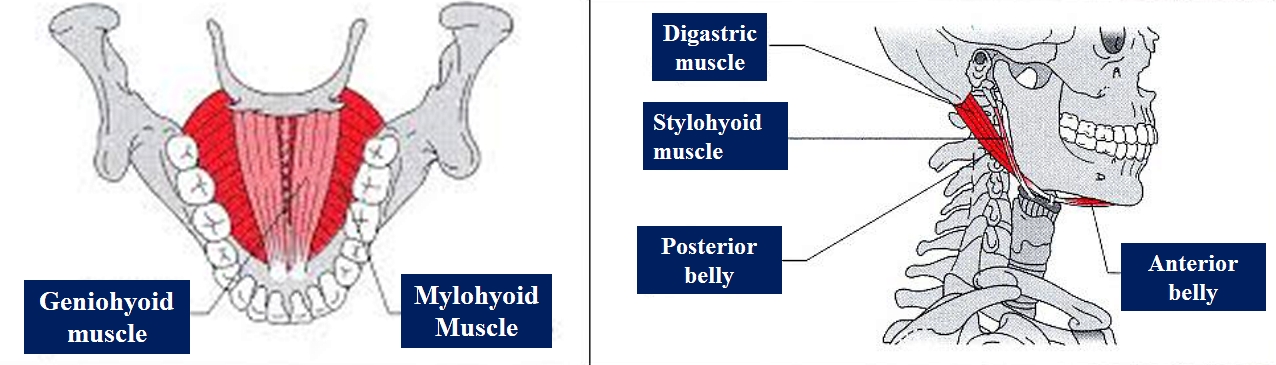
The supra-hyoid muscles are between the two bony landmarks, the base of the mandible above and the hyoid bone below. They are in pairs of four present on each side of the midline of the neck, named as follows
- Digastric
- Stylohyoid
- Mylohyoid
- Geniohyoid
Structure and Function
All the suprahyoid muscles are thin and slender muscles (except the mylohyoid) which connect the hyoid bone to the base of the mandible and the skull and help in the hanging of the hyoid bone from above. Whenever the base of the mandible is stabilized, then these muscles help in elevating the hyoid bone upwards and in turn in elevating the floor of the mouth for deglutition. Whenever the infrahyoid muscles stabilize the hyoid bone, then the suprahyoid muscles help in the depression of the mandible and thus help in wide opening of the mouth. The suprahyoid muscles participate in improving the flexion movement of the neck. They are located on three levels: a deep plane formed by the geniohyoid muscle, a medium plane consisting of the mylohyoid muscle and a surface plane formed by the digastric and styloid muscles. Some literature includes the hyoglossus muscle as part of the suprahyoid muscles; however, in most bibliographies, it is treated as an extrinsic tongue muscle, since it does not insert into any upper bone structure as do the rest of the suprahyoid muscles.
If we study the function of each muscle, it differs slightly in nature. Digastric muscle helps in depressing and retracting the chin, thus helping in the opening of the mouth. Digastric pulls the hyoid bone and the floor of the oral cavity upwards, thus helping in deglutition. The mylohyoid muscle also helps in elevating the floor of mouth and tongue, thus helping in deglutition and speaking. It also helps in the depression of the mandible when the hyoid bone is in a fixed position. The stylohyoid helps in drawing the hyoid bone upward and backward, elevating the tongue and elongates floor of the mouth. The geniohyoid muscle helps in bringing the hyoid bone upwards and forwards and also in the widening of the airway passage.
The geniohyoid muscle is under the genioglossus muscle; it is a small and short muscle that has a cylindrical shape located above the digastric muscle and the mylohyoid muscle.
The mylohyoid muscle has a square morphology that forms the muscular floor of the mouth; it connects superficially to the digastric muscles. The mylohyoid muscle participates in the formation of the Pirogoff triangle, created by the posterior edge of the mylohyoid muscle, the middle tendon of the digastric, and the hypoglossal nerve. This triangle contains the lingual artery.
The digastric muscle has this name because it has the characteristic of being one of the few muscles in the human body that has two muscular bellies, one anterior and one posterior, joined by an intermediate tendon. It connects from its posterior belly to the sternocleidomastoid muscle and to the splenius muscle of the head, which also inserts on the mastoid process. It also has similar linkages to the internal jugular vein, internal carotid artery, and the parotid gland.
The digastric muscle's posterior belly participates in the formation of the Beclard triangle, shaped by the posterior edge of the hyoglossus muscle, by the greater horn of the hyoid bone and by the posterior edge of the posterior belly of the digastric muscle. This triangle contains the hypoglossal nerve and the lingual artery. The anterior belly is related to its contralateral counterpart, with the submandibular gland and the superficial face of the mylohyoid muscle.
The stylohyoid is a thin and elongated muscle; it connects to the posterior belly of the digastric muscle in its path. Medially it is related to the external carotid artery.
In the complexity of these muscles, studies reveal that the geniohyoid muscle is stronger in moving the hyoid bone forward, while the mylohyoid muscle expresses greater force in moving the hyoid bone in a cranial direction.
Embryology
Out of the four suprahyoid muscles, mylohyoid and anterior belly of digastric are derived from the mesoderm of the first pharyngeal (branchial) arch and hence supplied by the nerve of the first arch, i.e., the mandibular nerve (the third division of cranial nerve V - the trigeminal nerve). The posterior belly of the digastric muscle and the stylohyoid are developed from the mesoderm of the second pharyngeal arch and hence supplied by the nerve of the second arch, i.e., the facial nerve (cranial nerve VII).[1]
The geniohyoid muscle derives from occipital somitic sources compared to other muscles.
The suprahyoid muscles appear towards the eighth week of gestation.
Blood Supply and Lymphatics
All the suprahyoid muscles of the neck receive vascular supply from the branches of the external carotid artery. The anterior belly of the digastric muscle gets its blood supplied from the facial artery (submental branch) and the posterior belly by occipital artery and posterior auricular artery. Geniohyoid receives supply via the lingual artery branches. The mylohyoid's blood supply is from the facial artery (submental branch) and inferior alveolar artery (mylohyoid branch).[2]
Lymphatics from the suprahyoid part of the neck drain into the submental and submandibular group of lymph nodes of the neck. Finally, these all drain into the deep cervical group of lymph nodes.
Nerves
.The mylohyoid and the anterior belly of digastric muscles receive innervation by mylohyoid nerve branch from the inferior alveolar branch of the mandibular nerve (the V3 branch of cranial nerve V). The stylohyoid and posterior belly of digastric muscles' nerve supply is by the facial nerve (VII cranial nerve). The first cervical nerve via the hypoglossal nerve innervates the geniohyoid muscle.
Muscles
All these muscles are named based on their origin and insertion (except the digastric muscle). The first part of the name indicates its origin, and the second part suggests its insertion. But here the origin, and insertion can be interchangeable depending on whether the hyoid bone is mobile or fixed by the infrahyoid muscles.
Digastric Muscle: It is a spindle-shaped muscle consisting of two bellies (di = two, gastric = belly), the anterior and the posterior bellies which are held together with an intermediate tendon. The posterior belly is quite long compared to the anterior belly of the digastric muscle and takes origin from the temporal bone (mastoid notch) and the anterior belly from the mandible (digastric fossa near the symphysis menti).[3] Both the bellies slope downwards from their origins to the middle and connect via an intermediate tendon anchored by a fascial sling (deep cervical fascia) to the hyoid bone (at the junction of body of the hyoid bone with its greater cornu). Even though both the bellies form a single muscle, because of the developmental difference, they are supplied by two different nerves of those particular pharyngeal arches from where each has developed. The posterior belly receives its supply from the facial nerve & anterior belly by the mylohyoid branch of the inferior alveolar nerve (mandibular). The two bellies of the digastric will form two boundaries of the submandibular triangle. Hence it is also called a digastric triangle. The two anterior bellies of either side of the midline together will establish two borders of the submental triangle.
Stylohyoid Muscle: This muscle accompanies the posterior belly of digastric, and both receive innervation from the same nerve (facial nerve). This slender muscle takes origin from the middle of the styloid process (temporal bone) and gets inserted to the hyoid bone (junction of the body and greater cornu) superior to omohyoid. Stylohyoid pulls the hyoid bone backward and upward, thus, in turn, elevates the tongue and elongates the floor of the mouth, helping in deglutition. The intermediate tendon of digastric muscle passes through stylohyoid muscle near its insertion.
Mylohyoid Muscle: This is a flat muscle taking origin from the inner surface of the body of the mandible (mylohyoid line). The origin is quite broad and extends from the symphysis menti (anteriorly) to the last molar tooth (posteriorly). Hence the name mylo (mylo = molar in Greek). The insertion is by joining with the opposite mylohyoid muscle in the midline of the neck (median fibrous raphe) anteriorly and body of hyoid bone posteriorly sloping downward and medially, on each side. Thus together it forms the gutter of the floor of the mouth and acts as a support for the tongue. Therefore it is also called as the diaphragma oris (oral diaphragm).
Geniohyoid Muscle: It is short, slender, ribbon-shaped muscle, situated deep to mylohyoid, representing the most proximal component of rectus cervices muscle. It takes origin from the inferior genial tubercle (symphysis menti) and gets inserted to the body of the hyoid bone. The two geniohyoid muscles on either side of the midline are parallel and close to each other.[4]
Physiologic Variants
The stylohyoid can be duplicated or absent. Sometimes stylohyoid might insert into the mylohyoid or omohyoid muscles themselves.
Sublingual glands and vessels might sometimes herniate through the mylohyoid muscle.[5]
Accessory heads of the anterior belly of digastric are quite common (65.8%) and can mislead a radiologist to be a mass in a CT or MRI radiography.[6][7][3] The anterior belly of digastric may be absent in rare cases (agenesis).
Variation of nerve to mylohyoid is even though rare but has important clinical implications in surgically manipulative surgeries like implants in the edentulous mandible, harvesting a graft, post-traumatic screw placement, etc.[8]
Surgical Considerations
The suprahyoid muscles form boundaries for the triangles of the neck present in the suprahyoid area. Between the digastric muscles' two anterior bellies is the submental triangle. Between the anterior and posterior bellies of the digastric muscle is the submandibular (digastric triangle). These triangles are essential for locating of particular structures within these triangles and hence knowledge of the boundaries of triangles, and their contents are vital for surgeons.
The posterior belly of digastric is a significant landmark for surgeons as three cranial nerves, i.e., hypoglossal, accessory, and vagus pass deep to the posterior belly of digastric along with three great vessels, i.e., external and internal carotid arteries, and internal jugular vein.[9]
The anterior belly of the digastric muscle is of great importance in some aesthetic surgical procedures, such as rhytidectomy, submental lipectomy, displacement of suprahyoid muscles, submental artery flap, change of cervicomental angle and in the revitalization procedures of the facial muscles after neurological injury.
Stylohyoid muscle transfer may be a surgical option when the digastric muscle is unusable for any of various reasons. The transfer is performed to improve the aesthetic and functional effect after a lesion of the marginal mandibular nerve, which lesion makes the lips asymmetrical.
In some surgical procedures, the addition of mylohyoid muscle transfer after a total parotidectomy facilitates better healing and adds volume.
Clinical Significance
The ligament of stylohyoid muscle which is fibrous sometimes ossifies partially leading to Eagle syndrome (stylohyoid syndrome).[10]. Eagle syndrome present in 4% population presents with mostly unilateral sharp shooting pain in jaw radiating into throat, tongue or ear leading to difficulty in deglutition, sore throat, and tinnitus especially on turning of the neck. Another cause of this syndrome is an excessive long styloid process (greater than or equal to 3 cm).[10] Eagle syndrome has been observed to be more common in patients with Turner syndrome than in the normal population.[11] Vascular type might lead to compression of internal carotid artery or vein.[12] Treatment is surgical by resection of whichever structure (ligament or process) is compressing the underlying structures.[13] In some animals, this ligament of stylohyoid muscle completely ossifies and appears as a distinct bone called the epihyal.
Other Issues
Researchers have recently observed that tongue pressure technique not only improves the strength of the muscles of the tongue but also to a greater extent, the enhancement of the functions of the suprahyoid muscles.[14]
Chin-tuck Against Resistance exercise, Shakers exercise, Expiratory Muscle Strength Training, and Neuromuscular Electrical Stimulation have shown to improve the strength of suprahyoid muscles in the laryngeal elevation, and in turn help in better airway protection during swallowing.
Suprahyoid muscles are manually treated by osteopathic approaches to improve the functioning of the tongue and the movement of the hyoid bone. The therapeutic approach to this muscle area is through fascial techniques.