An ectopic pregnancy occurs when fetal tissue implants outside of the uterus or attaches to an abnormal or scarred portion of the uterus. Ectopic pregnancies carry high rates of morbidity and mortality if not recognized and treated promptly. Ectopic pregnancies may present with pain, vaginal bleeding, or more vague complaints such as nausea and vomiting. This activity will review the etiology of ectopic pregnancy and examine treatment approaches. This activity will outline the role of the interprofessional team in recognizing and treating patients with ectopic pregnancies.
Objectives:
Provide a definition for ectopic pregnancy.
Identify symptoms of ectopic pregnancy.
Describe the proper evaluation for ectopic pregnancy.
Plan a discussion amongst interprofessional, interprofessional team members regarding the detection, evaluation, and management of ectopic pregnancies so that they can be detected quickly and appropriate management can be implemented immediately, enhancing patient outcomes.
Introduction
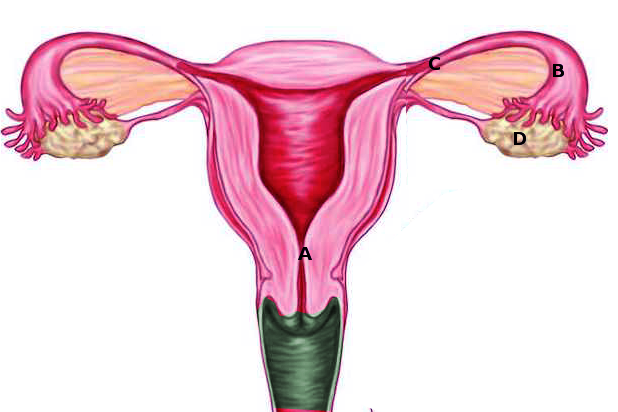
Ectopic pregnancy is a known complication of pregnancy that can carry a high rate of morbidity and mortality when not recognized and treated promptly. It is essential that providers maintain a high index of suspicion for an ectopic in their pregnant patients as they may present with pain, vaginal bleeding, or more vague complaints such as nausea and vomiting. Fertilization and embryo implantation involve an interplay of chemical, hormonal, and anatomical interactions and conditions to allow for a viable intrauterine pregnancy. Much of this system is outside the scope of this article but the most relevant anatomical components to our discussion on the ovaries, fallopian tubes, uterus, egg, and sperm. Ovaries are the female reproductive organs located to both lateral aspects of the uterus in the lower pelvic region. Ovaries serve multiple functions, one of which is to release an egg each month for potential fertilization. The fallopian tubes are tubular structures that serve as a conduit to allow transport of the female egg from the ovaries to the uterus. When sperm is introduced, it will fertilize the egg forming an embryo. The embryo will then implant into endometrial tissue within the uterus. An ectopic pregnancy occurs when this fetal tissue implants somewhere outside of the uterus or attaching to an abnormal or scarred portion of the uterus.
Etiology
Ectopic pregnancy, in essence, is the implantation of an embryo outside of the uterine cavity most commonly in the fallopian tube. Smooth muscle contraction and ciliary beat within the fallopian tubes to assist the transport of an oocyte and embryo. Damage to the fallopian tubes, usually secondary to inflammation, induces tubal dysfunction which can result in retention of an oocyte or embryo. There are several local factors, such as toxic, infectious, immunologic, and hormonal, that can induce inflammation.[1] There is upregulation of pro-inflammatory cytokines following tubal damage; this subsequently promotes embryo implantation, invasion, and angiogenesis within the fallopian tube.[1] Chlamydia trachomatis infection results in the production of interleukin 1 by tubal epithelial cells; this happens to be a vital indicator for embryo implantation within the endometrium[1] Interleukin 1 also has a role in downstream neutrophil recruitment which would further contribute to fallopian tubal damage.[1] Cilia beat frequency is negatively affected by smoking and infection. Hormonal variations throughout the menstrual cycle additionally have demonstrated effects on cilia beat frequency.[1].
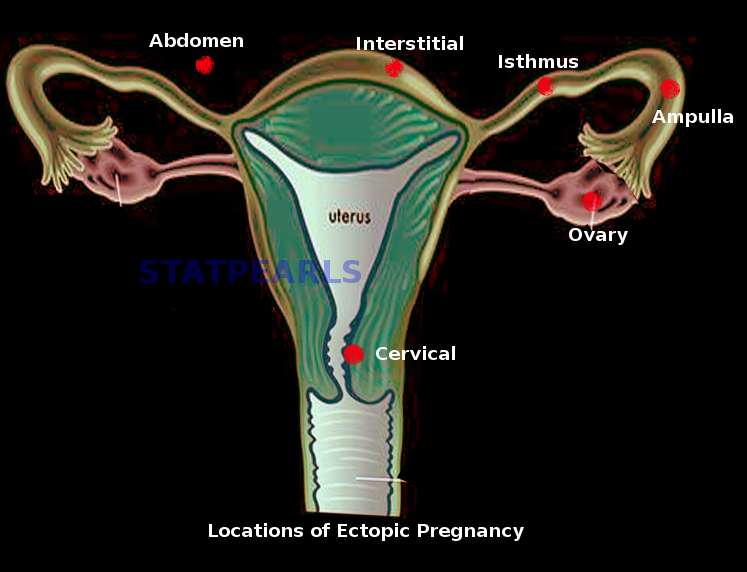
Ectopic implantation can occur in the cervix, uterine cornea, myometrium, ovaries, abdominal cavity, etc.[2] Women with tubal ligation or other post-surgical alterations to their fallopian tubes are at risk for ectopic pregnancies as the native function of the fallopian tube would be altered. The patient additionally can have an ectopic pregnancy with a concurrent intrauterine pregnancy, as known as a heterotopic pregnancy.[1]
Epidemiology
The estimated rate of ectopic pregnancy in the general population is 1 to 2% and 2 to 5% among patients who utilized assisted reproductive technology [1]. Ectopic pregnancies with implantation occurring outside of the fallopian tube account for less than 10% of all ectopic pregnancies.[1] Cesarean scar ectopic pregnancies occur in 4% of all ectopic pregnancies, as well as 1 in 500 pregnancies in women who underwent at least one prior c-section.[3] Interstitial ectopic pregnancies are reported in up to 4% of all ectopic implantation sites and have morbidity with mortality rates up to 7 times higher than other ectopic implantation sites. This increased morbidity and mortality are due to a high rate of hemorrhage in interstitial ectopic pregnancies.[1] Intramural ectopic pregnancies, those implanted in the myometrium, were reported in 1% of ectopic pregnancies.[1] Ectopic pregnancies implanting in the abdominal cavity account for 1.3% of ectopic implantation sites, of which adhere most commonly in the pouches anterior and posterior to the uterus as well as on the serosa of the adnexa and uterus.[1] Reports also exist of implantation sites in omental, retroperitoneal, splenic, and hepatic locations.[1]
Risk factors associated with ectopic pregnancies include advanced maternal age, smoking, history of ectopic pregnancy, tubal damage or tubal surgery, prior pelvic infections, DES exposure, IUD use, and assisted reproductive technologies.[1] Older age does bear risk with ectopic pregnancy; aged fallopian tubes likely have relatively decreased function predisposing to delay of oocyte transport. Women with prior ectopic pregnancies have up to ten times risk compared to the general population. Women pursuing in vitro fertilization have increased risk with developing an ectopic pregnancy with a concurrent intrauterine pregnancy, as known as heterotypic pregnancy. The risk is estimated as high as 1:100 women pursuing in vitro fertilization. The risk of developing a heterotopic pregnancy has been estimated as high as 1:100 in women seeking in vitro fertilization.[1]
Histopathology
The most common site for ectopic pregnancy adherence is in the ampullary region of the fallopian tube.[1] Reportedly 95% of ectopic pregnancies develop in the ampulla, infundibular, and isthmic portions of the fallopian tubes.[4] With cesarean scar pregnancies, there is a migration of blastocyst into the myometrium due to residual scarring defect from prior c-section.[3] The depth of implantation determines the type of cesarean scar pregnancy with type 1 having proximity to the uterine wall and type 2 implanting closer to the urinary bladder.[3]
History and Physical
Women presenting with an ectopic pregnancy will often complain of pelvic pain; however, not all ectopic pregnancies manifest with pain. Women of childbearing age who complain of pelvic pain/discomfort, abdominal pain/discomfort, nausea/vomiting, syncope, lightheadedness, vaginal bleeding, etc. should merit consideration for the possibility of pregnancy. Providers need to identify when the patient's last menstrual period occurred and whether they have monthly routine menstrual periods. If patients have missed their last period or have abnormal uterine bleeding, and are sexually active, then they may be pregnant and thus need further testing with a pregnancy test. Providers should identify any known risk factors for ectopic pregnancy in their patient's history, such as if a patient has had a prior confirmed ectopic pregnancy, known fallopian tube damage (history of pelvic inflammatory disease, tubal surgery, known obstruction), or achieved pregnancy through infertility treatment.[2]
After obtaining a thorough history, an attentive physical exam is the next step. Evaluation of vital signs to assess for tachycardia and hypotension is pivotal in determining the patient’s hemodynamic stability. When examining the abdomen and suprapubic regions, attention should focus on the location of tenderness as well as any exacerbating factors. If voluntary/involuntary guarding of the abdominal musculature is elicited on palpation, this should raise concern for possible free fluid or other cause of peritoneal signs. Palpating a gravid uterus may suggest pregnancy, however, does not exclude other pathologies such as progressed ectopic pregnancy or heterotopic pregnancy. Patient’s presenting with vaginal bleeding would likely benefit from a pelvic exam to assess for infections as well as assess the cervical os. Bimanual pelvic exams additionally allow for palpation of bilateral adnexa to assess for any abnormal masses/structures or to elicit adnexal tenderness. A thorough history and physical exam will lend better certainty with testing obtained when evaluating for possible ectopic pregnancy.
Evaluation
Transvaginal ultrasound imaging is pivotal in diagnosing suspected ectopic pregnancy. Serial exams with transvaginal imaging, serum hCG level measurements, or both are necessary to confirm the diagnosis. The first marker of an intrauterine pregnancy on ultrasound is a small sac eccentrically located within the decidua.[2] Two rings of tissue will form around the sac thus terming it the “double decidual” sign.[2] The double decidual sign usually becomes visible during the 5th week of pregnancy seen on abdominal ultrasound imaging.[2] The yolk sac will become apparent at this time but will require transvaginal ultrasound imaging for identification.[2] An embryonic pole will become visible on transvaginal imaging at around six weeks of pregnancy.[2] Uterine fibroids or highly elevated body mass index can limit the accuracy of ultrasound imaging to identify an early intrauterine pregnancy. MRI imaging can be helpful in extreme circumstances, such as those with large obstructing uterine fibroids; however, its sensitivity and specificity require further research and the potential risks with gadolinium contrast exposure merit consideration.[2]
The best diagnostic confirmation of an ectopic pregnancy comes through identifying a fetal heartbeat outside of the uterine cavity on ultrasound imaging. The absence of a discernable fetal heartbeat can be misleading; however, as a fetal heartbeat does not develop throughout all ectopic pregnancies.[2] Additional signs of ectopic pregnancy include identification of a gestational sac with or without a yolk sac within an ectopic location or having identified a complex adnexal mass that strays from the typical presentations of hemorrhagic corpus luteum.[2] When radiologic imaging fails to confirm the presence of an ectopic pregnancy adequately, direct visualization of the suspicious mass can occur via diagnostic laparoscopy.[2] Direct laparoscopy may not identify very small ectopic gestations, cervical pregnancies, or those located in cesarean scars.[2]
Treatment / Management
Administration of intramuscular methotrexate or performance of laparoscopic surgery is safe and effective treatment modalities in hemodynamically stable women with a non-ruptured ectopic pregnancy. The decision of which modality to pursue is guided by the patient’s clinical picture, their laboratory findings, and radiologic imaging as well as the patient’s well-informed choice after having reviewed the risks and benefits with each procedure. Patients with relatively low hCG levels would benefit from the single-dose methotrexate protocol. Patients with higher hCG levels may necessitate two-dose regimens. There is literature suggestive that methotrexate treatment does not have adverse effects on ovarian reserve or fertility.[5] hCG levels should be trended until a non-pregnancy level exists post-methotrexate administration.[6] Surgical management is necessary when the patients demonstrate any of the following: an indication of intraperitoneal bleeding, symptoms suggestive of ongoing ruptured ectopic mass, or hemodynamically instability.[6]
Surgical management including salpingostomy or salpingectomy should be guided by clinical status, the extent of fallopian tube compromise, and desire for future fertility. In simplest form salpingectomy involves removing the fallopian tube partially or in full.[1] Salpingostomy, or salpingotomy, involves removal of the ectopic pregnancy via tubal incision while leaving the fallopian tube in situ.[1]
Differential Diagnosis
One should begin to formulate a differential diagnosis when taking into account the patient’s history and physical exam findings. Important differential diagnoses to consider with ectopic pregnancies are ovarian torsion, tuba-ovarian abscess, appendicitis, hemorrhagic corpus luteum, ovarian cyst rupture, threatened miscarriage, incomplete miscarriage, pelvic inflammatory disease, and ureteral calculi. The patient's history and hemodynamic status on clinical presentation will influence the order of these differentials, as well as the testing necessary to rule out said differentials.
Prognosis
Patients with a relatively low beta hCG level will likely have a better prognosis regarding treatment success with single-dose methotrexate.[6] The further the ectopic pregnancy has advanced, the less likely single-dose methotrexate therapy will suffice. The patients that present in extremis or with hemodynamically instability have more risk of deterioration such as from hemorrhagic shock or other perioperative complications. Prognosis will thus hinge on early recognition and timely intervention. Fertility outcomes with tubal conservation surgeries remain debatable as some data suggests no significant difference in intrauterine pregnancy rates when comparing salpingectomy versus conservative tubal management.[7]
Complications
Women who present early in pregnancy and have testing suggestive of an ectopic pregnancy would jeopardize the viability of an intrauterine pregnancy if given Methotrexate.[4] Women who receive the single-dose Methotrexate regimen are at high risk of treatment failure if the hCG level does not decrease by 15% from day 4 to day 7 thus prompting second-dose regimen.[6] Women presenting with vaginal bleeding and pelvic pain may be misdiagnosed as an abortion in progress if the ectopic pregnancy is at the cervical os. The patient may have a cervical ectopic pregnancy and would thus run the risk of hemorrhage and potential hemodynamic instability if a dilation and curettage are performed.[4] Complications from management extend to treatment failure, in that women may present with/or develop hemodynamic instability which can result in death despite early operative interventions.
Deterrence and Patient Education
Patients who seek medical treatment for ectopic pregnancy may need to discuss with their obstetrician which foods, supplements, and drugs to avoid when taking methotrexate as there may be decreased efficacy due to adverse interactions with the drug. Methotrexate may increase immunosuppression when paired with other medications, among other potential adverse side effects. Patient’s that undergo surgical interventions will need to adhere to the recommendations by their surgeon as to limit the risk of infection as well as other post-operative complications.
Enhancing Healthcare Team Outcomes
When faced with the possibility of an ectopic pregnancy, the health care team needs to work collectively and efficiently to diagnose accurately and treat the susceptible patient. Women typically will present to the ER with this ailment, accurate and timely identification starts from the initial encounter when triaged by the nursing or provider in triage staff. It is the provider's responsibility to include/consider ectopic pregnancy as a potential differential diagnosis in all sexually active women of childbearing age. A systematic review and meta-analysis were performed to compare and test the performance of current protocols used when managing women with a pregnancy of unknown location [8]. This study found that a logistic regression model, termed the M4 model, outperformed the comparison management protocols thus providing guidance for clinicians when treating patients with the pregnancy of unknown location [8]. This model may increase efficiency when considering unnecessary testing or treatment. Communication remains vital when the discussion takes place with consultants such as between obstetricians, emergency department physician, nurses, and pharmacists. Patient safety and patient-centered care must be implemented when discussing the patient's treatment plan with the obstetrician and when utilizing treatment/management protocols.
(Click Image to Enlarge)
Ectopic pregnancy
Image courtesy S Bhimji MD
(Click Image to Enlarge)
Locations of ectopic pregnancies
Image courtesy S Bhimji MD
Contributed by Ami Kurzweil, MD
(Click Image to Enlarge)
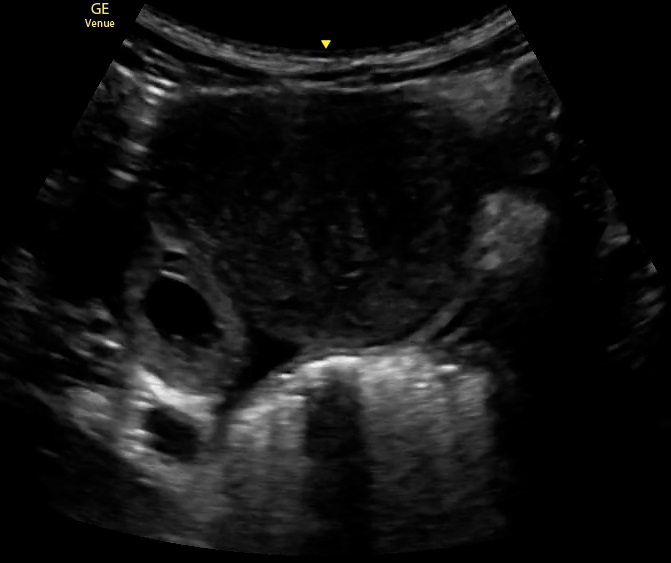
This image demonstrates an ectopic pregnancy via ultrasound.
Contributed by Kenn Ghaffarian, DO
Panelli DM, Phillips CH, Brady PC. Incidence, diagnosis and management of tubal and nontubal ectopic pregnancies: a review. Fertility research and practice. 2015:1():15. doi: 10.1186/s40738-015-0008-z. Epub 2015 Oct 15
[PubMed PMID: 28620520]
Carusi D. Pregnancy of unknown location: Evaluation and management. Seminars in perinatology. 2019 Mar:43(2):95-100. doi: 10.1053/j.semperi.2018.12.006. Epub 2018 Dec 20
[PubMed PMID: 30606496]
Chukus A, Tirada N, Restrepo R, Reddy NI. Uncommon Implantation Sites of Ectopic Pregnancy: Thinking beyond the Complex Adnexal Mass. Radiographics : a review publication of the Radiological Society of North America, Inc. 2015 May-Jun:35(3):946-59. doi: 10.1148/rg.2015140202. Epub 2015 Apr 10
[PubMed PMID: 25860721]
American College of Obstetricians and Gynecologists' Committee on Practice Bulletins—Gynecology. ACOG Practice Bulletin No. 193: Tubal Ectopic Pregnancy. Obstetrics and gynecology. 2018 Mar:131(3):e91-e103. doi: 10.1097/AOG.0000000000002560. Epub
[PubMed PMID: 29470343]
Bobdiwala S, Saso S, Verbakel JY, Al-Memar M, Van Calster B, Timmerman D, Bourne T. Diagnostic protocols for the management of pregnancy of unknown location: a systematic review and meta-analysis. BJOG : an international journal of obstetrics and gynaecology. 2019 Jan:126(2):190-198. doi: 10.1111/1471-0528.15442. Epub 2018 Sep 20
[PubMed PMID: 30129999]
Level 1 (high-level) evidence
Use the mouse wheel to zoom in and out, click and drag to pan the image