Continuing Education Activity
The rotator cuff, consisting of the muscle bellies and tendons of the infraspinatus, supraspinatus, teres minor, and subscapularis muscles, surrounds the shoulder joint. Rotator cuff syndrome encompasses various injuries or degenerative conditions affecting the rotator cuff, such as subacromial impingement syndrome, bursitis, tendonitis, and partial- (PTTs) or full-thickness (FTTs) rotator cuff tears. Rotator cuff syndrome is increasingly prevalent with age and is associated with metabolic syndrome, including diabetes, inflammatory arthritis, and thyroid disease. This condition encompasses various pathologies such as subacromial impingement syndrome, bursitis, tendonitis, and PTTs or FTTs of the rotator cuff. Chronic rotator cuff syndrome can elevate the risk of developing glenohumeral degenerative disease and rotator cuff arthropathy.
Radiographic imaging plays a vital role in diagnosing the condition, especially in acute or chronic shoulder pain. This condition poses a significant healthcare concern, leading to millions of office visits and considerable healthcare expenses worldwide. Therefore, timely evaluation, accurate diagnosis, and management of the condition are crucial, often necessitating an interprofessional team approach to ensure optimal patient care. This activity outlines the assessment and management of rotator cuff syndrome and highlights the integral role of the interprofessional healthcare team in delivering optimal patient care. In addition, this activity focuses on enhancing clinicians' abilities in examining, diagnosing, making decisions, and conducting clinical evaluations to treat patients suspected of having rotator cuff injuries.
Objectives:
Identify the signs and symptoms of rotator cuff syndrome in patients presenting with shoulder pain.
Implement evidence-based nonoperative treatment modalities for rotator cuff syndrome, including physical therapy and nonsteroidal anti-inflammatory drugs.
Select appropriate screening tools and imaging modalities, such as radiographs and MRI, to confirm the diagnosis of rotator cuff syndrome.
Collaborate with interprofessional healthcare providers to manage complex cases of rotator cuff syndrome, ensuring comprehensive treatment and rehabilitation.
Introduction
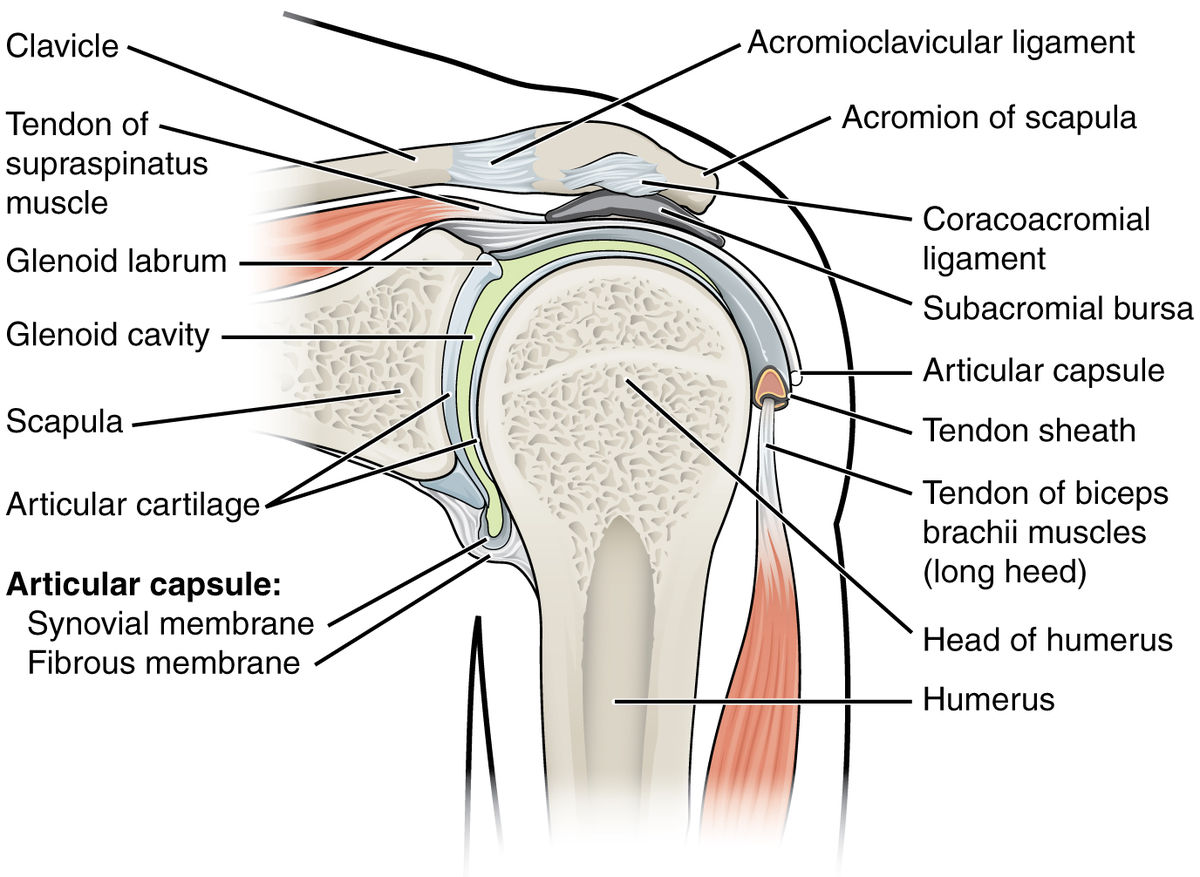
The rotator cuff is an anatomic coalescence of the muscle bellies and tendons of the supraspinatus (SS), infraspinatus (IS), teres minor (TM), and subscapularis (SubSc) surrounding the shoulder joint (see Image. Shoulder Joint Anatomy).[1] Rotator cuff syndrome constitutes a spectrum of diseases across various pathologies associated with injuries or degenerative conditions affecting the rotator cuff. These conditions include subacromial impingement syndrome, bursitis, rotator cuff tendonitis, and partial- (PTTs) or full-thickness (FTTs) rotator cuff tears. Chronic rotator cuff syndrome can elevate the risk of developing glenohumeral degenerative disease and rotator cuff arthropathy.[2][3][4] Rotator cuff syndrome is increasingly prevalent with age and is associated with metabolic syndrome, including diabetes, inflammatory arthritis, and thyroid disease.
Etiology
The correlation between subacromial impingement syndrome and rotator cuff syndrome remains a subject of controversy.[4]
Terminology
To best understand the clinical association of these conditions, it is essential to comprehend the constellation of symptoms implied by each clinical diagnosis and the associated terminology initially.
Rotator cuff tendonitis/tendinosis: These are acute or chronic tendinopathic conditions stemming from a vulnerable environment for the rotator cuff secondary to repetitive eccentric forces and predisposing anatomical or mechanical risk factors. Acute injuries and chronic overuse can result in focally weakened cuff regions. These vulnerable areas evolve into PTTs or FTTs, depending on the type of eccentric forces experienced by the rotator cuff.[5]
Shoulder impingement: This clinical term is frequently used nonspecifically to characterize patients who experience pain or symptoms during overhead activities.
Internal impingement: This condition is prevalent among overhead-throwing athletes, such as baseball pitchers and javelin throwers.[6] Impingement typically transpires at the posterior or lateral articular side of the cuff when it contacts the posterior or superior glenoid rim and labrum during the maximum abduction and external rotation of the shoulder, known as the "late cocking" phase of throwing.
- The term "thrower's shoulder" refers to a common set of anatomic adaptive changes that develop over time in this subset of athletes.
- These adaptive changes include, but are not limited to, increased humeral retroversion and posterior capsular tightness.
- Glenohumeral internal rotation deficit (GIRD) results from these anatomic adaptations, predisposing the thrower's shoulder to internal impingement.
External impingement: This term is often used interchangeably with subacromial impingement syndrome. External impingement involves external compressive sources, such as the acromion, which can lead to subacromial bursitis and injuries to the bursal side of the rotator cuff.[4]
Theories
One must also acknowledge the historical and evolving theories, as mentioned below, regarding the etiology and pathophysiology of the clinical spectrum of rotator cuff syndrome.
Extrinsic compressive theories: Historically, the predominant theory concerning the etiology of rotator cuff syndrome attributed it to extrinsic compression factors as the main instigator of the pathophysiologic cycle. These factors include anatomical structures that directly injure the cuff. In historical context, Watson-Jones described the pathological impingement of the lateral acromion on the rotator cuff during mid-arc shoulder abduction. Neer later popularized and modified the theory of degenerative acromial spurring and advocated for the clinical importance of the anterior aspect of the acromion as the predominant source of impingement. In addition to the anterior spurring, the coracoacromial ligament can become calcified in chronic subacromial impingement syndrome and serve as another source of extrinsic compression on the cuff.[3] Bigliani later highlighted the significance of acromial morphology, particularly the hooked-type acromion, in predisposing patients to subacromial impingement syndrome.[7] Several studies later documented an association between the hooked-type acromial morphology, impingement symptoms, and rotator cuff FTTs.[8][9] Other possible anatomical causes include acromioclavicular joint degenerative changes, subacromial spurs, and, in much rarer instances, symptomatic os acromiale.[10][11][12]
Subacromial impingement implies extrinsic compression secondary to a narrowing of the subacromial space. As knowledge of extrinsic compression has evolved, a particular subset of patients exhibiting a variation in rotator cuff pathology was documented in the literature with increasing incidence rate recognition. Internal impingement occurs secondary to the pathologic abutment of the articular side of the rotator cuff, between the posterior/superior glenoid rim, and greater tuberosity of the humerus when the arm is in maximum shoulder abduction, external rotation, and extension.[13][14] The theory of internal impingement provides a crucial differentiation from external compressive forces and a narrowed subacromial space, as these patients do not typically exhibit a pathologically narrowed acromiohumeral interval.
Intrinsic degenerative theories: These theories propose another set of etiological factors as the primary contributors to the pathology underlying the clinical presentation of patient-reported symptoms related to rotator cuff issues. Although opposing theories date back to the 1930s, with Codman and Akerson suggesting intrinsic tendon degeneration of the rotator cuff, more substantial evidence emerged in the 1990s. Multiple reports during this period highlighted increasing evidence supporting degenerative changes in the rotator cuff, particularly with advancing patient age.[15][16][17]
Generally, intrinsic degenerative theories suggest that degeneration of the rotator cuff eventually undermines the overall stability of the glenohumeral joint. As dynamic stability is compromised, the humeral head migrates superiorly, reducing the size of the subacromial space. Consequently, the cuff becomes vulnerable to secondary extrinsic compressive forces, which can result in degeneration and tearing.[3][18]
Vascular Changes
Several studies have identified regions of hypovascularity in the rotator cuff tendons, which may contribute to attritional degeneration of the cuff. Lohr et al initially demonstrated a distal area of the supraspinatus tendon on the articular side lacking blood vessel supply in a cadaveric study.[19] Rudzki et al also demonstrated an age-dependent manner of increasing degrees of hypovascularity in this tendinous region.[16] However, controversy arises from other studies proposing that attritional areas develop secondary to preceding impingement mechanisms. Consequently, blood vessel damage may occur, leading to ischemia, tenocyte apoptosis, gross tendinopathy, and attritional cuff damage.[20] Furthermore, many studies have reported increased vascularity in focal areas of the cuff, with hypervascularity associated with age-related changes, tendinopathy, and rotator cuff tears—PTTs and/or FTTs.[21][22]
Age, Sex, and Genetics
Histologically, age-related changes in the rotator cuff include collagen fiber disorientation and myxoid degeneration.[23] The literature indicates a higher frequency of rotator cuff abnormalities with advancing age. The prevalence of these abnormalities rises from 5% to 10% in patients aged 20 and younger, to 30% to 35% in individuals in their sixth and seventh decades of life, peaking at 60% to 65% in individuals aged 80 or older.[24]
Tensile Forces
According to Budoff et al, the primary mode of cuff failure is attributed to eccentric tension repeatedly placed on the rotator cuff.[25] Rotator cuff syndrome can also be associated with glenohumeral instability, PTTs and rotator cuff fatigue over time (especially with overhead overuse), and posterior capsular contractures.[26][27] As the subacromial bursa degenerates over time, it loses its physiologic protective potential for the cuff, becoming another source of mechanical compression.[4]
Environmental Factors
Sports and occupation: Various social and environmental factors contribute to the development of rotator cuff syndrome over time. Occupational mechanical risk factors encompass positions involving manual labor, significant heavy lifting, constant overhead work, and repetitive activities in general.[28][29] Miranda et al conducted a 20-year follow-up study of a cohort of workers in Finland, revealing the synergistic effect of multiple occupational mechanical risk factors in the development of rotator cuff syndrome and/or shoulder pain. Pertinent factors included occupational force requirements, shoulder posture during the actual work, and overhead activity requirements.[30] Similarly, as alluded to earlier, overhead activities in sports, such as throwing, also predispose patients to develop rotator cuff syndrome.[6]
Smoking: Multiple studies in the literature have supported a dose- and time-dependent association between smoking and rotator cuff tears. A 2010 study investigated 586 subjects with unilateral shoulder pain, noting almost two-thirds of the rotator cuff tear subgroup had a documented current or history of smoking.[31] Additional studies have suggested a correlation between smoking and rotator cuff degeneration, symptomatic cuff tears, and the enlargement of existing cuff tears.[32][33]
Medical comorbidities: Several medical conditions may contribute to the development and worsening of rotator cuff syndrome. Metabolic syndrome, along with its associated diagnoses such as dyslipidemia, hypertension, hyperglycemia, and abdominal obesity, has established links with rotator cuff pathology.[34][35] Moreover, individual medical conditions comprising the metabolic syndrome, as well as thyroid disorders, diabetes, and inflammatory arthritides, are considered additional risk factors for rotator cuff syndrome.[36][37][38][39]
Contemporary etiologies for rotator cuff pathology: The majority of rotator cuff tears occur in the anterior half of the supraspinatus tendon, typically beginning approximately 1 cm from its insertion point on the greater tuberosity. This specific area has been identified as the "anterior critical zone."[40][41] The hypovascularity observed in this critical zone has been linked to our current understanding that most rotator cuff tears originate at the articular side.[42]
Epidemiology
The prevalence of rotator cuff syndrome and its associated pathologies affects millions of patients worldwide. In the United States alone, shoulder pain results in approximately 4.5 million office visits and incurs about $3 billion in healthcare costs annually.[43] Rotator cuff syndrome affects patient populations in an age-dependent manner, ranging from 5% to 10% of patients aged 20 and younger to over 60% of patients aged 80 or older. Overall, chronic shoulder pain has a lifetime prevalence rate of 67% in the adult population.[24][44]
Subacromial impingement syndrome is recognized as the leading cause of both acute and chronic shoulder pain.[3][18] The literature supports an equal incidence of rotator cuff syndrome and tears when comparing male and female populations.[45][46]
Pathophysiology
The Extrinsic Compressive Theory
The extrinsic compressive theory of subacromial impingement syndrome suggests that the syndrome's onset is attributed to anatomical and/or mechanical factors that elevate pressure and result in pathological contact, thereby predisposing the cuff to susceptibility and tendinopathy.
Extrinsic mechanisms include both subacromial impingement syndrome and internal impingement.
The Intrinsic Compressive Theory
The intrinsic theory of subacromial impingement syndrome attributes the condition to a predisposition for a weakened cuff that degenerates progressively. Factors such as age, hand dominance, vascular changes, and repetitive eccentric forces contribute to this weakening, compromising the dynamic stability of the shoulder. As a result, the humeral head migrates proximally, reducing the acromiohumeral interval and heightening the susceptibility of the cuff to additional injury and degeneration.
Intrinsic mechanisms encompass factors such as tendon vascularity (particularly in the anterior critical zone of the supraspinatus tendon), tendon biology, tendon mechanical properties, tendon morphology, and genetic predisposition.
Histopathology
Histological changes observed in rotator cuff syndrome consist of the following:
- Rounded tenocytes indicating apoptosis
- Extracellular matrix disorganization and myxoid degeneration
- Vascular changes, including focal hypervascularity and hypovascular regions
- Reduced total cellularity
- Presence of calcified depositions
- Thinning of collagen fibers
- Degenerative changes in the acromion, reaching the level of cuff-arthropathy [21][22][23][47]
History and Physical
Clinicians assessing acute or chronic shoulder pain should gather a comprehensive history. Key features indicative of rotator cuff syndrome include:
- Atraumatic, insidious onset of pain
- Symptom exacerbation with overhead activity
- Pain experienced at night
A thorough history includes details such as current or past involvement in sports (including specific positions played), occupational background and current employment status, hand dominance, any prior shoulder and/or neck injuries or traumas, and pertinent surgical history.
Physical Examination Pearls
C-spine/neck exam: Coexisting cervical radiculopathy should be ruled out when evaluating neck and/or shoulder pathology. Observing neck posture, muscular symmetry, palpable tenderness, and assessing active/passive range of motion (ROM) is crucial. Special tests, including the Spurling maneuver, myelopathic testing, reflex examination, and a comprehensive neurovascular assessment, can be helpful in this context.[48]
Shoulder exam: Clinicians should assess the overall shoulder girdle for symmetry, shoulder posture, and muscle bulk and symmetry. Additionally, they should rule out scapular winging. Examination of the skin for previous surgical incisions, lacerations, scars, erythema, or induration is also important.
After the observational component of the physical examination, both active and passive ROM are assessed. In cases of rotator cuff syndrome, patients may display compromised active ROM but typically retain full passive ROM. Conversely, limited passive ROM, in the absence of advanced degenerative changes impacting the glenohumeral joint, is indicative of adhesive capsulitis and warrants a distinct treatment approach from that of rotator cuff syndrome/impingement.[18][49]
Rotator Cuff Muscle Strength Testing
The clinician may evaluate motor strength grading for C5 to T1 nerve roots and perform specific rotator cuff muscle strength testing. Specifically, rotator cuff strength and/or pathology can be assessed via the examinations mentioned below.
Supraspinatus (SS): Various tests are utilized to evaluate the function and identify potential pathologies of the supraspinatus muscle when assessing its integrity.
- Jobe test: A positive result manifests as pain or weakness when downward pressure is resisted. The patient's shoulder is positioned at 90° of forward flexion and abduction in the scapular plane, with the thumb facing downward.
- Drop arm test: The patient's shoulder is elevated to 90° of abduction in the scapular plane. Initially, the examiner supports the limb and then instructs the patient to slowly adduct the arm to the side of the body. A positive test includes the patient’s inability to maintain the abducted position of the shoulder and/or an inability to adduct the arm to the side of the trunk in a controlled manner.
Infraspinatus (IS): Various tests are utilized to evaluate the function and identify potential pathologies of the infraspinatus muscle when assessing its integrity.
- Strength testing: This test is performed while the shoulder is positioned against the side of the trunk, the elbow is flexed to 90°, and the patient is instructed to rotate the arm outward while the examiner resists this external movement.
- External rotation lag sign: The examiner positions the patient’s shoulder in the same position, and while holding the wrist, the arm is brought into maximum external rotation. The test is positive if the patient’s shoulder drifts into internal rotation after the examiner removes the supportive external rotation force at the wrist.
Teres minor (TM): Various tests are utilized to evaluate the function and identify potential pathologies of the teres minor muscle when assessing its integrity.
- Strength testing: This test is conducted with the shoulder at 90° of abduction and the elbow flexed to 90°, enabling optimal isolation of the teres minor muscle. The examiner then resists external movement to evaluate muscle strength.
- Hornblower’s sign: With the patient's shoulder in the same position, the examiner rotates the arm into maximum external rotation while holding the wrist. A positive result is indicated if the patient's shoulder drifts into internal rotation after the external rotation force at the wrist is removed.
Subscapularis (SubSc): Various tests are utilized to evaluate the function and identify potential pathologies of the subscapularis muscle when assessing its integrity.
- Internal rotation lag sign: The examiner passively brings the patient’s shoulder behind the trunk (about 20° of extension) with the elbow flexed to 90°. Then, the examiner internally rotates the shoulder by "handing off" the patient's back while supporting the elbow and wrist. A positive test occurs if the patient cannot maintain this position after the examiner releases support at the wrist (ie, the arm does not stay in internal rotation, and the dorsum of the hand drifts toward the back).
- Passive external rotation range of motion: An increase in passive external rotation compared to the contralateral shoulder may indicate a PTT or FTT of the subscapularis.
- Lift-off test: This test is more sensitive and specific for lower subscapularis pathology. In the same position as the internal rotation lag sign, the examiner places the dorsum of the patient's hand against the lower back and resists the patient's attempt to lift the hand away from the lower back.
- Belly press: This test is more sensitive and specific for upper subscapularis pathology. The examiner positions the patient's arm at 90° of elbow flexion, and internal rotation testing is performed by having the patient press the palm of their hand against the belly, bringing the elbow in front of the trunk plane. Initially supporting the elbow, a positive test occurs if the elbow cannot be maintained in this position when the examiner removes the supportive force.
External impingement/subacromial impingement syndrome: This refers to a common shoulder condition characterized by pain and restricted movement, often aggravated by certain maneuvers. Various diagnostic tests such as the Neer impingement sign and test, as well as the Hawkins test, are utilized to assess and confirm the presence of impingement symptoms.
- Neer impingement sign: This sign is positive if the patient reports pain with passive shoulder forward flexion beyond 90°.
- Neer impingement test: A positive result is noted after the examiner administers a subacromial injection, and the patient reports symptom improvement upon repeating the forced passive forward flexion beyond 90°.
- Hawkins test: A positive test occurs when the examiner positions the shoulder and elbow passively at 90° of flexion in front of the body, and the patient reports pain upon passive internal rotation of the shoulder.[50]
Internal impingement: In the internal impingement test, the patient is placed in a supine position, and the shoulder is moved into terminal abduction and external rotation. A positive test is indicated by the reproduction of the patient's pain.[3][51][52]
Evaluation
Radiographic imaging is essential for evaluating acute or chronic shoulder pain in all patients.
Radiographs
The recommended imaging protocol includes obtaining a true anteroposterior (AP) view of the glenohumeral joint, commonly known as the "Grashey" view. This image is obtained with the patient rotated between 30° and 45°, adjusting the coronal plane cassette accordingly. Alternatively, the beam can be angled while the patient remains in a neutral coronal plane position. Measuring the acromiohumeral interval, typically between 7 and 14 mm, helps assess for abnormalities such as advanced degenerative arthritis and rotator cuff arthropathy.
Additional radiographic imaging options include a 30° caudal tilt view, which aids in detecting acromial spurring. Furthermore, the "scapular Y" or "supraspinatus outlet" view provides valuable information regarding acromial morphology.
Pertinent Findings
The most common radiographic changes associated with external impingement/subacromial impingement syndrome and rotator cuff syndrome include rotator cuff arthropathy, which is characterized by proximal humeral migration and an acromiohumeral interval reduction to less than 7 mm.
Degenerative Findings
- Osteophytes on the acromion, proximal humerus, and/or glenoid are often seen in cases of advanced disease
- Calcification of the cuff arthropathy level and/or coracohumeral ligament
- Greater tuberosity cystic degeneration
- Acromioclavicular joint arthritis
"Hooked" acromion: The presence of a "hooked" acromion is best appreciated on the supraspinatus outlet view.
Os acromiale: Os acromiale is best visualized on an axillary lateral radiograph.
Ultrasound
Ultrasound is an underutilized imaging modality for assessing rotator cuff tendon and muscle belly integrity. A 2011 meta-analysis of over 6,000 shoulders showed a sensitivity of 0.96 and a specificity of 0.93 in detecting PTT or FTT cuff tears. Another study highlighted the potential challenges in differentiating between PTTs and FTTs, particularly those measuring approximately 1 cm in size.[18]
Magnetic Resonance Imaging
Magnetic resonance imaging (MRI) is valuable for assessing the extent and nature of rotator cuff pathology. MRI can provide accurate details about cuff tears, including PTTs and FTTs, as well as their size, location, and degree of retraction. Additionally, MRI can detect fatty degenerative changes in the cuff, particularly in chronic pathology, through T1-weighted sagittal sequence series.
Subdeltoid and/or subacromial bursitis are significant considerations as potential pain sources. Additionally, assessing the acromioclavicular joint, acromial morphology, and integrity of the long head of the biceps tendon provides valuable insights. A systematic review of shoulder MRIs is crucial, especially when aligning the findings with patient-reported symptoms and clinical examination.[3]
Treatment / Management
Given the complex nature of rotator cuff syndrome, treatment and management have been divided into the categories mentioned below.
Group 1: Partial- or Full-Thickness Rotator Cuff Tears, Asymptomatic Patient
Patients presenting with MRI evidence of rotator cuff tears, PTTs or FTTs, may not exhibit symptoms. The latest American Academy of Orthopaedic Surgeons (AAOS) clinical practice guideline summary notes the increasing recognition of incidental rotator cuff pathology on shoulder MRIs in asymptomatic individuals. Although rotator cuff disease prevalence rises with age, there's no conclusive evidence that surgical intervention prevents tear progression or symptom development. Therefore, the committee recommends managing symptoms through nonoperative modalities alone.
Group 2: Partial-Thickness Rotator Cuff Tears, Symptomatic Patients
Symptomatic patients with signs of external impingement/subacromial impingement syndrome and partial-thickness rotator cuff tears initially undergo nonoperative treatment modalities. The optimal timing for surgical intervention in this group varies, with literature suggesting intervals ranging from 3 to 18 months. Surgical intervention should be personalized based on the patient's symptoms, improvement with nonoperative modalities, and overall goals.
Group 3: Chronic Rotator Cuff Tears, Symptomatic Patients
The AAOS clinical practice guideline issues a "weak" recommendation for symptomatic patients with chronic rotator cuff tears due to limited evidence comparing rotator cuff repair with ongoing nonoperative treatments in this population. Individual patient assessment is crucial, and treatment decisions should be customized based on the patient's unique clinical circumstances.[53]
Nonoperative Rotator Cuff Syndrome Treatment Modalities
Physical therapy: Physical therapy is the primary first-line treatment for rotator cuff syndrome. PTTs, including aggressive rotator cuff, periscapular stabilizer strengthening programs, and ROM exercises, can be managed alone.
Anti-inflammatory medications:
- First-line nonoperative management also includes the use of nonsteroidal anti-inflammatory drugs (NSAIDs) in conjunction with physical therapy modalities.
- Although the AAOS clinical practice guidelines reported inconclusive evidence supporting the efficacy of NSAIDs, iontophoresis, transcutaneous electrical nerve stimulation (TENS), and similar modalities for FTTs, the committee reported a “moderate” recommendation grade for exercises and/or NSAIDs in cases of symptomatic rotator cuff syndrome in the absence of FTTs.
Cortisone injections: Cortisone injections are commonly administered into the subacromial space for external impingement/subacromial impingement syndrome. Patients often experience rapid symptomatic relief post-injection, facilitating their participation in subsequent physical therapy sessions.
Rest/activity modifications: Rest and activity modifications are beneficial for patients, particularly during the initial phase of treatment. It involves avoiding exacerbating activities such as repetitive overhead motions and heavy lifting, which can aid in symptom management and recovery.
Surgical Management
Surgical management options for rotator cuff syndrome encompass various techniques such as debridement, subacromial decompression, and/or acromioplasty, along with rotator cuff debridement. In cases without full-thickness rotator cuff tears, surgical intervention for external impingement/subacromial impingement syndrome typically involves:
Subacromial decompression:
- Extensive debridement of the subacromial space is recommended for patients experiencing persistent symptoms of external impingement/subacromial impingement syndrome despite failed nonoperative modalities over 4 to 6 months.
- A comprehensive bursectomy facilitates a thorough and precise evaluation of the bursal side of the cuff.
- Debridement of cuff arthropathy is advised in cases with significant fraying and/or calcification, as it serves as an additional source of impingement.
- A meta-analysis of 9 studies comparing open versus arthroscopic procedures demonstrated comparable surgical times, outcomes, and complication rates at the 1-year follow-up. However, the arthroscopic approach allowed for a quicker return to work compared to the open technique.
Acromioplasty:
- Shaving the undersurface of the acromion, particularly in cases with significant spurring, enhances the environment surrounding the cuff and increases clearance between the acromion and cuff during mid-arc and terminal range of motion, as well as impingement positions.
- In cases of hooked acromion morphologies, meticulous debridement of this area using a shaver, burr, or rasp is performed to flatten the undersurface.
- The anterior deltoid origin serves as the anterior boundary of the acromioplasty, and care should be taken to preserve this area during the debridement process. Impingement symptoms often arise from spurring in the anteroinferior region of the acromion.
Os acromiale: In cases of persistent symptoms associated with os acromiale, a 2-stage procedure is commonly used. Initially, bone grafting techniques are utilized to fuse the os acromiale, followed by a formal acromioplasty once the fusion has healed.[5][12][53][54]
Differential Diagnosis
The differential diagnosis for chronic shoulder pain includes several etiologies, as listed below.
Impingement
- External or subacromial impingement syndrome
- Subcoracoid
- Calcific tendonitis
- Internal impingement, including superior labrum anterior to posterior lesions, GIRD, little league shoulder, posterior labral tears)
Rotator Cuff Pathology
- PTTs versus FTTs
- Rotator cuff arthropathy
Degenerative
- Advanced degenerative joint disease, often associated with rotator cuff arthropathy
- Glenohumeral arthritis
- Adhesive capsulitis
- Avascular necrosis
- Scapulothoracic crepitus
Proximal Biceps
- Subluxation, often seen in association with subscapularis injuries
- Tendonitis and tendinopathy
Acromioclavicular Joint Conditions
- Acromioclavicular separation
- Distal clavicle osteolysis
- Acromioclavicular arthritis
Instability
- Unidirectional instability, often seen in association with an inciting event or dislocation (anterior, posterior, or inferior)
- Multidirectional instability
- Associated labral injuries or pathology
Neurovascular Conditions
- Suprascapular neuropathy, may be associated with paralabral cyst at the spinoglenoid notch
- Scapular winging, occurring in either a medial or lateral direction
- Brachial neuritis
- Thoracic outlet syndrome
- Quadrilateral space syndrome
Other Conditions
- Scapulothoracic dyskinesia
- Os acromiale
- Muscle ruptures, including pectoralis major, deltoid, and latissimus dorsi
- Fractures, arising from acute injury or pain resulting from long-standing deformities, malunions, or nonunions
Prognosis
Most patients with rotator cuff syndrome without FTTs typically show improvement with nonoperative management. According to the most recent clinical practice guidelines from the AAOS, initial treatment with NSAIDs and/or exercise programs received a "moderate" recommendation grade, supported by multiple level II studies in the literature. Additionally, insights from the MOON shoulder group in 2013 shed light on the management and outcomes of atraumatic FTTs of the rotator cuff.
In a cohort of almost 500 patients, nonoperative treatment resulted in 75% reporting positive patient-reported outcomes at a 2-year follow-up. Furthermore, patients opting for surgery (25%) typically made this decision between 6 and 12 weeks after the initial onset of symptoms.
Complications
Complications associated with rotator cuff syndrome can be categorized into nonoperative- and operative-related complications:
Nonoperative Management
- Persistent pain or recurrent symptoms may occur.
- In the setting of PTTs, a theoretical risk of tear propagation, lack of healing, fatty infiltration, atrophy, and retraction is apparent.
- A controversial topic, a 2017 study analyzed independent risk factors for symptomatic rotator cuff tear progression over 19 months of nonoperatively managed shoulders. Factors contributing to tear progression included:
- The initial presence of an FTT
- Medium-sized cuff tears, ranging from 1 to 3 cm
- Smoking
- Interestingly, while PTTs were included in the study, their presence was not identified as a risk factor for cuff tear progression.
- In cases of chronic or atrophic tears, especially with rotator cuff tear propagation, degenerative joint disease, and rotator cuff arthropathy ensue.
Surgical Management
- Surgical intervention is effective and typically considered for patients who have not experienced improvement or have reported persistent or worsening symptoms despite undergoing at least 4 to 6 months of comprehensive nonoperative treatment modalities.
- Common risks associated with surgery include recurrent pain or symptoms, infection, stiffness, neurovascular injury, and complications related to anesthesia.
- Specific surgical procedures may include:
- Subacromial decompression/acromioplasty
- Deltoid dysfunction: This complication can occur secondary to failed deltoid repair following an open acromioplasty or excessive debridement during arthroscopy.
- Anterosuperior escape: This complication occurs secondary to aggressive release of the cuff arthropathy level. This leads to a compromise of the coracoacromial arch and suspensory system. In massive, retracted, and irreparable rotator cuff tears, the humeral head may migrate superiorly and anteriorly, affecting patient functional outcomes.[55]
Postoperative and Rehabilitation Care
After undergoing subacromial decompression/acromioplasty (without rotator cuff syndrome), patients typically wear a sling for 1 to 2 weeks while beginning early passive ROM rehabilitation. However, clinicians should be cautious of excessive sling immobilization, especially when soft tissue repair protocols are unnecessary. Initially, patients are advised to refrain from heavy lifting and strenuous exercises to promote soft tissue healing. Cryotherapy devices are commonly used during the first 10 to 14 days postoperatively. Physical therapy usually commences after discontinuation of the sling. Full active ROM is typically achieved within 3 to 6 weeks. Return to sport-specific activities is generally permitted at 6 to 8 weeks, depending on individual tolerance levels.
Consultations
Primary care clinicians are often able to effectively manage the majority of rotator cuff syndrome cases, particularly focusing on nonoperative treatments. When these modalities have been exhausted, referral to an orthopedic surgeon is appropriate. While nonoperative management typically does not require a supervised physical therapy protocol, such guidance is recommended in the postoperative phase to optimize ROM and strength recovery.
Deterrence and Patient Education
Patients should receive comprehensive education regarding the nature of their condition, including the potential for continued chronic pain even after surgical management for persistent impingement/rotator cuff syndrome symptoms.
Enhancing Healthcare Team Outcomes
Rotator cuff syndrome encompasses a spectrum of clinical symptoms, from mild shoulder impingement to progressive PTTs and FTTs in the long term. Effective management of the condition requires collaboration among an interprofessional team of clinicians. When evaluating acute or chronic shoulder pain, it is crucial to integrate clinical examination findings with radiographic imaging, MRI, and response to nonoperative treatments such as physical therapy, NSAIDs, rest or activity modification, and injections.
In conservative management, pharmacists are critical in educating patients about pain management strategies, whereas physical therapists guide exercises to enhance muscle strength and joint mobility. Surgical intervention is considered when impingement symptoms persist or worsen despite conservative measures. Referral to an orthopedic surgeon becomes necessary in cases of longstanding persistent symptoms. Close communication and collaboration among interprofessional healthcare team members is vital to optimize patient outcomes.