Introduction
The following seven bones form the orbit:
- Sphenoid
- Frontal
- Zygomatic
- Ethmoid
- Lacrimal
- Maxilla
- Palatine
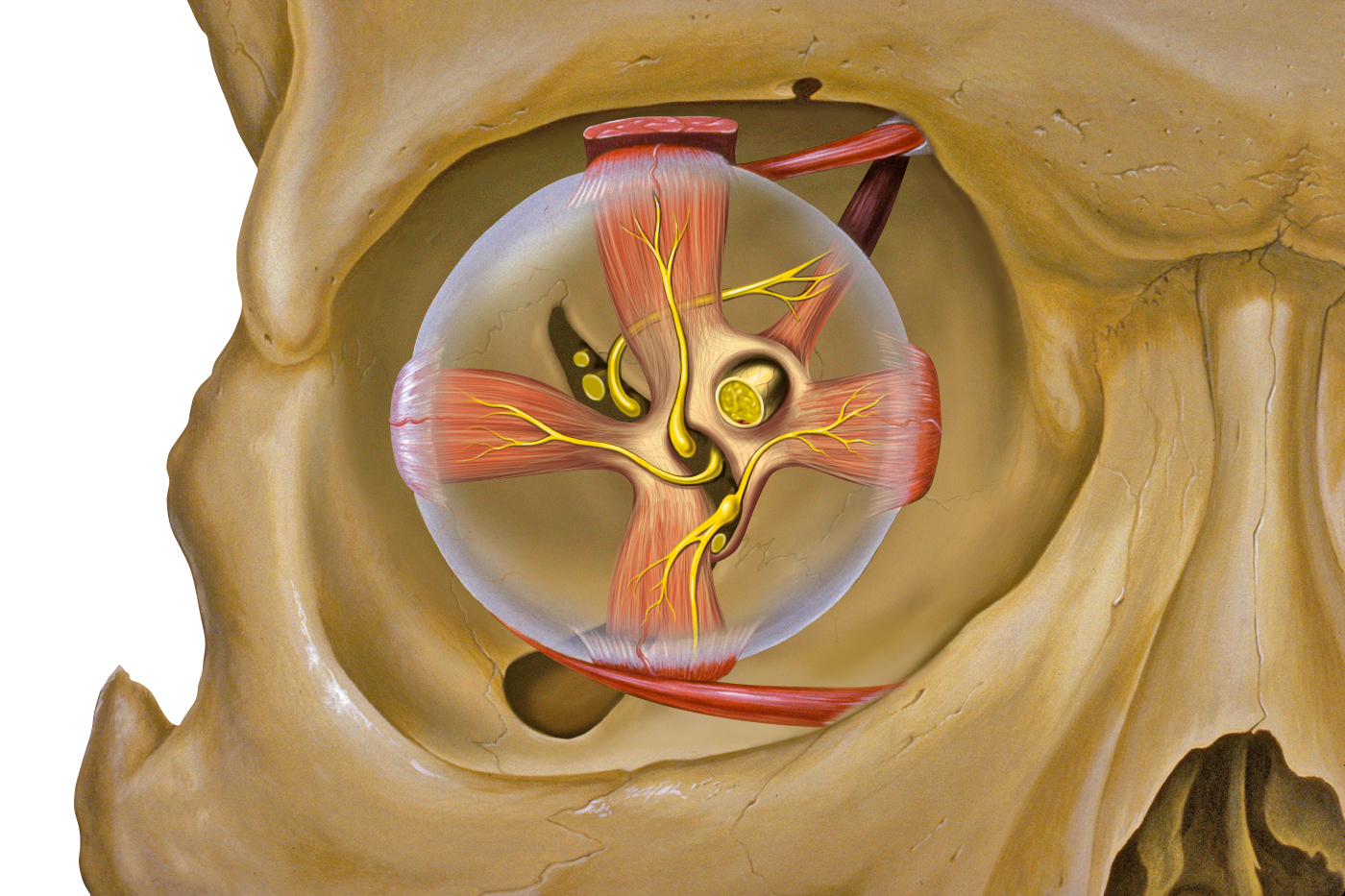
The orbit is a pear shape, with the optic nerve at the stem, and holds approximately 30 cc volume. The entrance to the globe anteriorly is approximately 35 mm high and 45 mm wide. The depth from orbital rim to the orbital apex measures 40 to 45 mm in adults. The maximum width is 1 cm behind the anterior orbital margin. Both race and gender can affect the measurements of the bony orbit. The orbital cavity contains the globe, nerves, vessels, lacrimal gland, extraocular muscles, tendons, and the trochlea as well as fat and other connective tissue. An increase in the volume of the extraocular structures within the orbit can cause proptosis, which is protrusion of the globe and/or displacement (deviation) of the globe from its normal position.
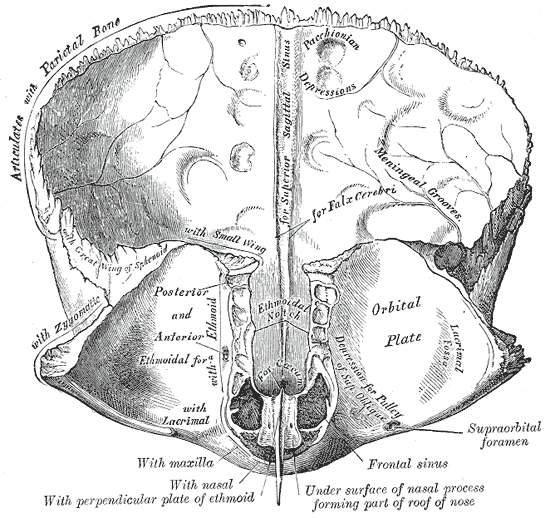
The orbital margin is the anterior opening of the globe and has a quadrilateral spine formed by several of the bones that make up the orbit. The roof of the orbit is formed by the orbital plate of the frontal bone and the lesser wing of the sphenoid. The fossa of the lacrimal gland lies anterolaterally, behind the zygomatic process of the frontal bone.
Walls of the Orbit
The orbital roof consists of two parts of two bones, the orbital plate frontal bone and the lesser wing of the sphenoid bone. The fossa of the lacrimal gland is in the orbital roof, and it lies anteriorly and laterally behind the zygomatic process of the frontal bone. The trochlear fossa is medial and about 4 mm from the orbital margin. This is where the pulley of the superior oblique is attached.
The medial orbital wall consists of four bones, the frontal process of the maxillary bone: the lacrimal bone, the orbital plate of the ethmoid bone, and the lesser wing of the sphenoid bone. The largest part of the medial wall is from the ethmoid bone. The frontal process of the lacrimal fossa and the bony nasolacrimal canal are continuous and extend into the inferior meatus of the nasal cavity. The medial wall of the ethmoid bone is actually very thin and is called the lamina papyracea.
The floor of the orbit consists of three bones: the maxillary bone, the palatine bone, and the orbital plate of the zygomatic bone. This part of the orbit is also the roof of the maxillary sinus. There is an infraorbital groove along the floor and it travels into a canal anteriorly where it eventually exits as the infraorbital foramen. This is the structure that lies below the orbital margin of the maxillary bone. Along the floor of the orbit is the origin of the inferior oblique muscle. This is the only extraocular muscle that does not originate at the apex of the orbit.
Lateral Orbital Wall
The lateral orbital wall is formed by two bones: the zygomatic bone and the greater wing of the sphenoid. This is the strongest of the walls of the orbit. There is a lateral orbital tubercle, which is an elevation of the orbital margin of the zygomatic bone and is an attachment for many important structures. These are the ligament of the lateral rectus muscle, the suspensory ligament of the eyeball (Lockwood ligament), lateral palpebral ligament, aponeurosis of the levator palpebrae superioris muscle, and the Whitnall ligament.
Orbital Foramina, Fissures, and Ducts
Several openings in the bones of the orbit have anatomic and clinical applications.
The optic nerve, the ophthalmic artery, and choroid plexus sympathetic fibers come from the middle cranial fossa and travel into the orbit via the optic foramen. The optic foramen passes through the lesser wing of the sphenoid bone and travels inferiorly, anteriorly, and laterally as it enters the orbit.
The supraorbital foramen is on the superior margin of the orbit and contains blood vessels and the supraorbital nerve.
The anterior ethmoidal foramen is in the frontoethmoidal suture, while the posterior ethmoidal foramen is located at the junction of the orbit's roof and medial wall. These two foramina transmit the anterior ethmoidal vessels and nerve and the posterior ethmoidal vessels and nerve, respectively.
The nasolacrimal duct drains tears from the eye into the inferior meatus of the nose.
The infraorbital canal comes from the infraorbital groove. This contains the infraorbital nerve, which is the maxillary division of CN V.
The superior orbital fissure lies between the greater and lesser wings of the sphenoid bone. Passing through the superior orbital fissure into the orbit and above the common tendinous ring are the lacrimal nerve of CN V1, the frontal nerve of CN V1, CN IV (trochlear nerve), and the superior ophthalmic vein. Passing through the superior orbital fissure and the common tendinous ring are the superior and inferior divisions of CN III (oculomotor), the nasociliary branch of CN V1, sympathetic roots of the ciliary ganglion, and CN VI (abducens).
The inferior orbital fissure lies on the floor of the orbit. The superior border is the greater wing of the sphenoid, and the maxilla and palatine bone compose the inferior border, with the zygomatic bone laterally. The zygomatic nerve and the infraorbital nerve pass through this fissure as well as some infraorbital vessels.
The infraorbital vessels then travel along the floor of the orbit and pass through infraorbital groove anteriorly.[1][2][3]