Continuing Education Activity
Atrophie blanche (AB) is a morphologic pattern of scarring that occurs secondary to a clinicopathologic entity known as livedoid vasculopathy. This is a chronic condition that presents as recurrent, painful, ulcers of the lower leg, ankle, or dorsal foot, predominately occurring in young to middle-aged females with subsequent scar formation. Atrophie blanche describes the result of healed ulcers. This activity will review the diagnosis and management of atrophie blanche and highlights the role of the interprofessional health team in improving patient outcomes with this condition.
Objectives:
- Identify the etiology of atrophie blanche.
- Review the appropriate evaluation of atrophie blanche.
- Outline the treatment and management options available for atrophie blanche.
- Describe interprofessional team strategies for improving care coordination and communication among health care professionals managing patients with atrophie blanche and improve outcomes.
Introduction
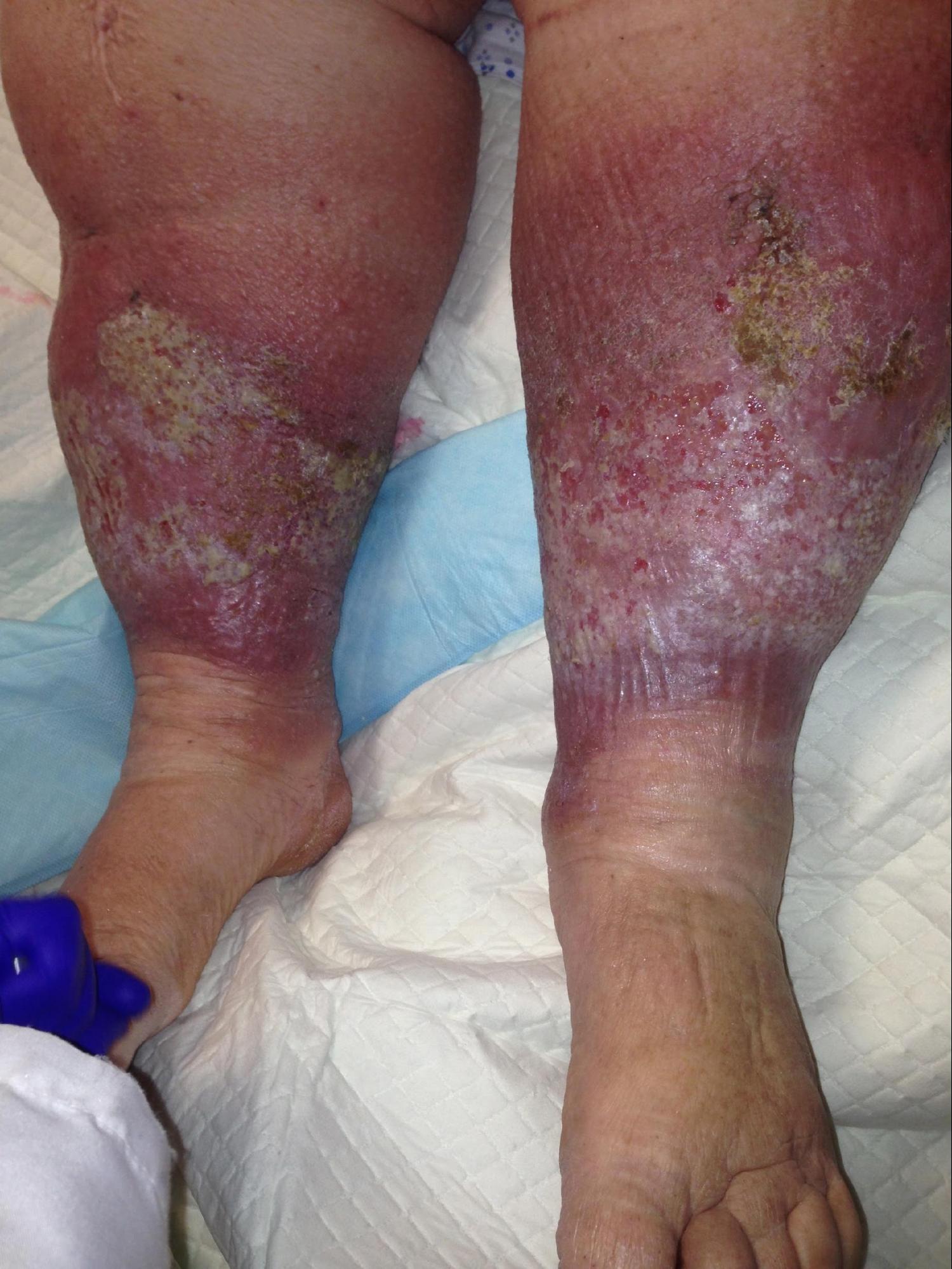
Atrophie blanche (AB) is a morphologic pattern of scarring that occurs secondary to a clinicopathologic entity known as livedoid vasculopathy. It is a chronic condition that presents as recurrent, painful, ulcers of the lower leg, ankle, or dorsal foot, predominately occurring in young to middle-aged females with subsequent scar formation. Atrophie blanche describes the result of healed ulcers. These characteristically present as a white, atrophic stellate scar with peripheral telangiectasias. Atrophie blanche is also known as livedoid vasculopathy, which in its purest form, is the primary, ulcerated lesion. Livedoid vasculopathy is poorly understood. It is believed to involve occlusion of the blood vessels in the superficial dermis with subsequent skin ulceration. There are several other less commonly used terms to describe this condition, such as segmental hyalinizing vasculitis, livedo reticularis with summer ulceration, and painful purpuric ulcers with reticular patterning on the lower extremities (PURPLE).[1] Physical exam findings will depend on the disease stage but classically present in a middle-aged woman with bilateral, painful, purpuric lower leg lesions that develop punched-out ulcerations.[2] These ulcers are chronic, slow to heal, and leave the classic stellate, white scars. Although it occurs more frequently in middle age females, it does occur in males, and there are a few case reports of disease in children.
Many other diseases may present with a similar end-stage as atrophie blanche. The causes of atrophie blanche-like lesions include cutaneous small-vessel vasculitis and antiphospholipid antibody syndrome. These other disorders can be distinguished from atrophie blanche as the history will lack preceding punched-out ulceration.[3]
Etiology
There are many theories regarding the cause of livedoid vasculopathy, but the exact underlying mechanism is poorly understood.[4] It is believed to involve occlusion of the blood vessels in the superficial dermis with subsequent skin ulceration.
Epidemiology
Atrophie blanche is an uncommon disease entity affecting 1% to 5% of the population and occurring primarily in middle-aged female adults with an average age of occurrence of 45-years-old. However, there are rare case reports of children with the disease.[5][6][7]
Pathophysiology
The pathophysiology of atrophie blanche can vary depending on the underlying etiology. It is often idiopathic but may be associated with several other disease processes, including autoimmune conditions and hypercoagulable disorders. The pathogenesis typically involves disturbances in fibrinolysis and/or coagulation, leading to thrombo-occlusion of blood vessels in the superficial dermis.[8] Several prothrombotic factors may share a correlation with atrophie blanche, including aPL antibodies, abnormalities in protein S and C, hyperhomocysteinemia, sticky platelet syndrome, antithrombin III deficiency, and factor V Leiden mutation.
Histopathology
The histologic examination can vary depending on the age of the lesion. A characteristic histopathologic finding is mild perivascular lymphocytic inflammation, extravasated red blood cells, superficial dermal vessels with thrombi, and hyalinized vessel walls. Biopsy of an active ulcer will show infarction of the papillary dermis, whereas biopsy of a healed lesion will show an atrophic epidermis and dermal sclerosis. Immunofluorescence examination is non-specific in early lesions. In later lesions, immunoglobulins, routinely IgM, and C3 are deposited within the vessel walls.[9]
History and Physical
Physical exam findings depend on the disease stage. The patient often initially complains of bilateral, painful, purpuric lesions that progress to punched-out ulcers, with or without surrounding livedo reticularis. These lesions will heal with porcelain-white, stellate scars, with or without surrounding telangiectasias. History typically reveals that the ulceration is recurrent and is often exacerbated in the summer and during pregnancy.[9]
It is essential to rule out other possible causes, so history should focus on eliminating underlying diseases such as peripheral arterial disease, venous stasis, and malignancy. A patient with atrophie blanche-like lesions will lack a history or physical exam finding of punched-out ulcers.[3]
Evaluation
Since the end manifestations of many diseases can produce atrophie blanche-like lesions, excluding these other causes is necessary to diagnosis true atrophie blanche, i.e., livedoid vasculopathy. Many studies will help a clinician to rule in or rule out other disease etiologies. The following is not an exhaustive list:
- Doppler studies and ankle-brachial index are aids to rule-out venous stasis and arterial occlusion[10]
- A skin biopsy to rule out cutaneous vasculitis
- Screening coagulation studies to evaluate for antiphospholipid antibody syndrome
- Lab work should include hemoglobin A1C
- Complete blood count with differential
- Basic metabolic panel
- Antinuclear antibody (ANA)
- Rheumatoid factor and C-reactive protein (CRP) to aid differentiation of diabetes mellitus, autoimmune syndromes, and malignancy
Treatment / Management
Treatment of atrophie blanche in the absence of underlying disease often starts with antiplatelet, anticoagulation, and fibrinolytic therapies, including aspirin, dipyridamole, pentoxifylline, and heparin. Sulfasalazine, danazol, or stanozolol can work as single agents or in addition to other treatments. Other options that have shown success include hyperbaric oxygen and PUVA (psoralen and ultraviolet A radiation). For patients with refractory disease, rivaroxaban, oral steroids, prostanoids, and IVIG (intravenous immunoglobulin) have been used with varying success. Patient education should include recommendations to stop smoking, to avoid irritants and poorly fitting shoes, as well as basic wound care of the lower extremities, i.e., leg elevation, compression therapy, and occlusive wound dressings.[6][11][12]
Differential Diagnosis
Many other diseases may present with a similar end-stage as atrophie blanche. The causes of atrophie blanche-like lesions include cutaneous small-vessel vasculitis, hydroxyurea-related ulcers, sickle cell disease, and antiphospholipid antibody syndrome. These other disorders can be distinguished from atrophie blanche as the history will lack preceding punched-out ulceration.[13]
Prognosis
The prognosis of atrophie blanche varies but it tends to be a chronic, recurring disease.[4]
Complications
Infection, scarring, pain, ulceration, blood loss, stricture formation, and poor quality of life are all potential complications of atrophie blanche.
Deterrence and Patient Education
Patient education is important. It should include recommendations to discontinue tobacco to avoid irritants and poorly fitting shoes as well as basic wound care of the lower extremities, i.e., leg elevation, compression therapy, and occlusive wound dressings.[11]
Enhancing Healthcare Team Outcomes
Lower extremity ulcers can pose a diagnostic dilemma. The cause of a lower extremity wound may be due to a myriad of diagnoses, including arterial or venous disease, infection, trauma, and diabetes mellitus, among other etiologies.
As a patient may present to various medical professionals, i.e., nurses, clinicians (wound care, podiatry, family medicine, etc.), home health aides, prompt communication with an interprofessional group must optimize the timeliness of diagnosis and appropriate care.
The diagnosis is often complicated and requires exhaustive studies. Even after making the diagnosis, the treatment is not straightforward. Not everyone responds to the same treatment, and one may need to try several different approaches to heal the ulcers. Patients should be provided with realistic expectations of the outcome. Irrespective of the treatment, the importance of a wound care nurse cannot be overstated. These patients need long-term wound care with daily dressing changes and regular debridement. Pain management is an issue, and a pharmacist and a pain specialist must be involved. Empirical prescription of opioid pain medications should be avoided to prevent addiction and tolerance.
Since many patients develop stress and anxiety, mental health professionals may be consulted. Patient ambulation should be encouraged to prevent dependent edema, worsening of pain, and pressure sores.
Open and effective communication is key for good patient outcomes. [Level 5]. An interprofessional approach to atrophie blanche is essential. Clinicians will likely be the ones diagnosing the condition. Nursing will be involved with history taking and preparing the patient for examination. They can also provide counseling and monitor the patient's response to pharmaceutical therapy. As always, the pharmacist should verify the clinician's agent selection and dosing, and also offer feedback regarding potential drug interactions, and report these back to the team. If there is a psychological element to the case, counseling professionals can assist and keep the team appraised of progress on that front. All these various individuals need to communicate across interprofessional lines, to ensure all members of the team have all the latest information, and together drive positive outcomes. [Level 5]