Introduction
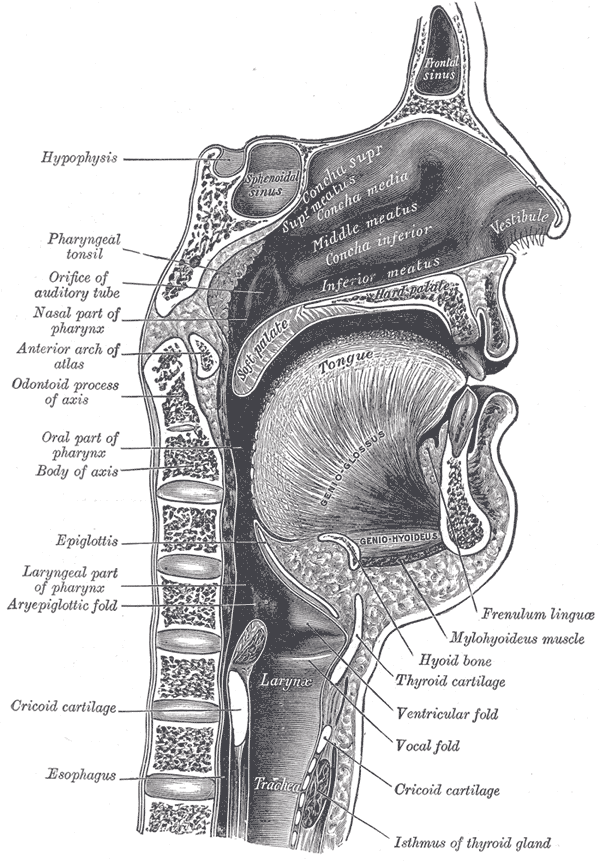
The larynx is continuous with pharynx superiorly and the trachea inferiorly. It is comprised of an intricate skeleton of cartilages held together by fibro-elastic membranes. Intrinsic muscles of the larynx moving these cartilages allow it to perform vital functions. Its most fundamental role is as a protective sphincter of the airway, but it also allows effort closure and vocalization. Understanding of the structure and function of the larynx is important for any clinical practitioner as pathology can be life-threatening or have a significant impact on patients’ quality of life.[1][2][3][4]
Structure and Function
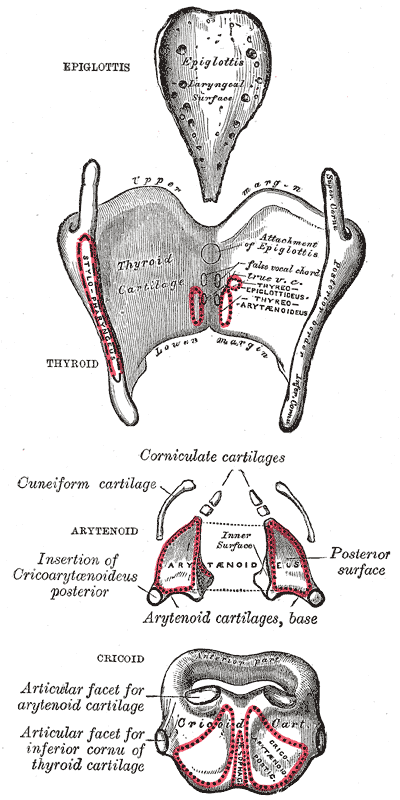
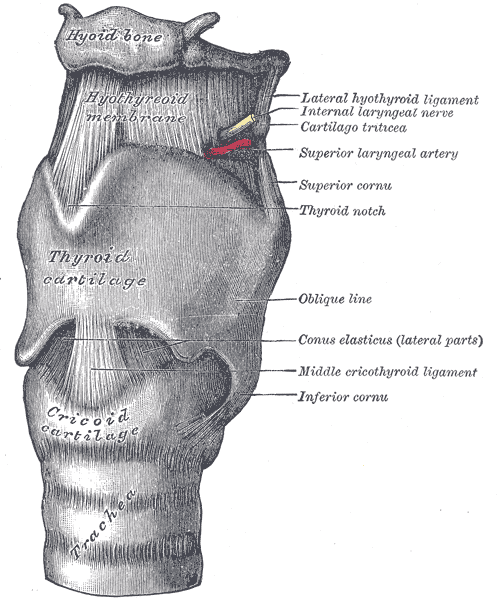
While not a component of the larynx, it is essential to appreciate the hyoid bone because of its close membranous connection to the laryngeal cartilaginous skeleton. This C-shaped bone sits superiorly to the larynx and is suspended in the midline of the anterior neck by suprahyoid and infrahyoid strap muscles.[5] These muscles can move the hyoid and, thereby, the larynx superiorly or inferiorly in a mid-sagittal plane. The skeleton of the larynx consists of three unpaired midline cartilages and four pairs of smaller cartilages. The three unpaired cartilages are the epiglottis, thyroid, and cricoid. The paired cartilages comprise of the arytenoids, corniculates, cuneiforms, and tritiates.
Thyroid cartilage
The thyroid cartilage is the largest cartilage of the larynx and is composed of hyaline cartilage. It sits beneath the hyoid bone to which it connects by the thyrohyoid membrane. Inferiorly it articulates with the cricoid cartilage. In an axial plane, it may appear as an incomplete triangle, with an apex anteriorly and two sides laterally but devoid of a base posteriorly. A large flat pentagonal plate called a lamina forms each side. The laminae meet anteriorly to form an apex with a v-shaped notch that can be appreciated externally as the laryngeal prominence or ‘Adam’s apple.’ During puberty in males, there is growth in the sagittal dimensions and prominence of the cartilage; this correlates with longer vocal cords and deepening of the voice. The interlaminar angle at the apex is more acute in males post-puberty, with an average of 76 degrees versus 94 degrees in females.[6] The appearance of the laryngeal prominence may be changed surgically for cosmetic reasons by altering the thyroid cartilage.[7][8] The body of each lamina is a thin, flat plate except for a diagonal ridge called the oblique line that is visible on the exterior surface of the laminae. This ridge serves as an attachment for sternothyroid and thyrohyoid strap muscles, which depress and elevate the larynx, respectively. At the posterior, superior corner of each thyroid lamina, there is a superior cornu (horn), which is a cartilaginous protrusion that runs upwards towards the hyoid bone.
Similarly, there is an inferior cornu that extends from the posterior, inferior corner and runs downwards to articulate with the cricoid cartilage. Just inferior to the thyroid notch, on the inner surface of the apex between the laminae, attachments for the thyroepiglottic ligament and vocal cords can be found. The joining of the vocal cords into the thyroid cartilage is known as the anterior commissure. Tumors of the vocal cords are often manageable by endoscopic intervention. However, if a tumor extends via the cords to the anterior commissure, it can invade the thyroid cartilage, necessitating a laryngectomy.[9] The hyaline cartilage of the thyroid calcifies progressively with age, from a posterolateral to anteromedial direction.[6] This calcification means laryngeal ultrasound can be used in young patients to assess vocal fold motion, but it makes this infeasible above 40 years of age.[10] Calcified hyaline cartilages such as the thyroid and cricoid may become visible on plain radiographs in adult patients.
Cricoid cartilage
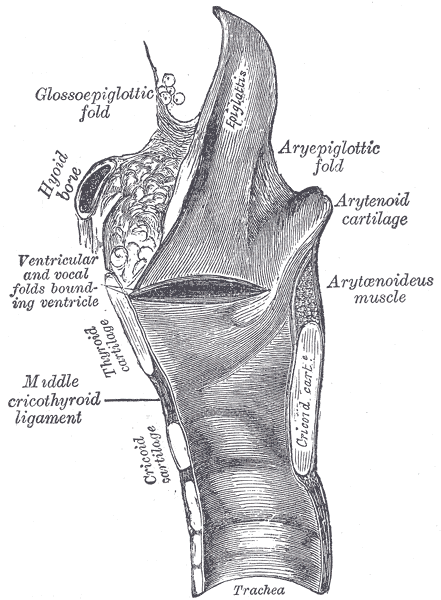
The cricoid is the only cartilage in the larynx that completely encircles the airway. It is composed of hyaline cartilage and resembles a signet ring in shape, being narrow anteriorly (approximately 5 mm) and tall posteriorly (approximately 20 mm).[11] The tall posterior portion of the cricoid is known as the cricoid lamina and the anterior portion of the cricoid arch. Its inferior border is a horizontal ring that is attached to the trachea by the cricotracheal ligament. The superior border runs obliquely, from the narrow arch anteriorly up to the tall lamina posteriorly. It sits beneath the thyroid cartilage to which it connects by the median cricothyroid ligament and the conus elasticus. Anteriorly, the cricoid arch can be palpated through the skin inferiorly to the laryngeal prominence, with the median cricothyroid ligament lying between them. These are important landmarks in airway management. Laterally, marking the border between arch and lamina are the articular facets for the articulation of the cricoid with the inferior cornu of the thyroid cartilage. This joint allows tilting of the thyroid on the cricoid in a sagittal plane, caused by the cricothyroid muscle and antagonized by the thyroarytenoid muscle. As the vocal cords are attached to the thyroid cartilage anteriorly, this tilting movement can stretch the cords resulting in increased tension and pitch of voice. Posteriorly, the cricoid lamina appears quadrilateral in shape. Atop its superior aspect sits the arytenoid cartilages, which provide the posterior attachment of the vocal cords. As a complete ring, the application of pressure on the cricoid muscle can cause compression of the esophagus, which can be employed during rapid sequence intubation to reduce gastric insufflation and reflux, although the evidence for its efficacy is uncertain.[12]
Arytenoid cartilages
The arytenoidhichs are paired hyaline cartilages, which each take the shape of a three-sided pyramid. Their base articulates with the superior part of the cricoid lamina, and the apex points upwards. The three surfaces are named anterolateral, medial, and posterior. The medial surfaces form the inter-cartilaginous component of the rima glottidis (the opening between the vocal cords and arytenoid cartilages). The anterolateral surface has attachments for the thyroarytenoid muscle and vestibular ligaments. This surface has two cartilaginous processes that extend from its base. The vocal process points anteriorly and connects with the vocal ligament. The muscular process points laterally and is a point of attachment for posterior and lateral cricoarytenoid muscles. The posterior surfaces connect by transverse and oblique fibers of the inter-arytenoid muscle. These intrinsic muscles of the larynx cause sliding or rotational movements at the cricoarytenoid joints. This motion defines the position of the vocal process and, by extension, the vocal cords. Changing the position of the vocal cords will alter the shape of the rima glottidis and the flow of air through it.[13][14]
Epiglottis
The epiglottis is a leaf-shaped elastic cartilage. Its stem arises from the inner surface of the thyroid interlaminar angle, to which the thyroepiglottic ligament connects it. Superiorly, the stem broadens to form a round leaf with a free upper edge that sits behind the tongue base. Each lateral edge is connected to the ipsilateral arytenoid cartilage by a quadrangular membrane. During swallowing, the hyoid and larynx are drawn upward by suprahyoid muscles. This action causes the base of the tongue to press on the epiglottis, which, combined with the contraction of the aryepiglottic muscle and weight of the food bolus, causes depression of the epiglottis. In this depressed position, it covers the laryngeal inlet and may deflect food boluses laterally in the hypopharynx. The contribution of the epiglottis to airway protection has long been debated, with some arguing it is vestigial with no important physiological role.[15] There are many reports of patients having success swallowing following surgical removal of the epiglottis.[15] However, there are also pediatric cases where chronic aspiration has been attributed to a hypoplastic epiglottis, and the debate continues.[16][17][16] Pathology of the epiglottis may compromise the airway. Acute epiglottitis caused by Haemophilus influenzae is a potentially life-threatening infection. However, this is now rare in the developed world following widespread vaccination.[1] In infantile laryngomalacia, tightening of the aryepiglottic folds can cause the epiglottis to obstruct the airway during inspiration partially.[2] This usually self resolves without the need for surgery.
Corniculate, cuneiform, and tritiate cartilages
These are small, paired hyaline cartilages. The corniculate cartilages sit atop the apex of the arytenoid cartilages. Along with the cuneiforms, they can be seen as elevations in the aryepiglottic mucosal fold on endoscopy. The triticeal cartilages are within the thyrohyoid membrane in around a third of the population.[18]
Embryology
Laryngeal cartilages begin to develop in the fourth week of embryogenesis. A 2018 study on fourteen human embryos has provided a new description of the embryology of the hyoid-larynx complex, which is distinct from traditional and textbook descriptions based on comparative embryology. The thyroid and cricoid cartilages arise from mesenchymal condensations in the neck regions, and not from fourth or sixth pharyngeal arch cartilages as previously described.[19]
Blood Supply and Lymphatics
Like all cartilages, the laryngeal cartilages are avascular. They derive nutrition via diffusion from the blood supply of the overlying mucosa and surrounding tissue, most of which are supplied by the superior thyroid branch of the external carotid artery.[11]
Nerves
While the cartilages are aneural, surgeons need to have an intimate knowledge of their anatomical relationships to the course of the laryngeal nerves, as described elsewhere.[20]
Muscles
The intrinsic muscles of the larynx mentioned above are important in moving the cartilages of the larynx to allow protection of the airway, effort closure, and vocalization. They are described in detail elsewhere.[21]
Clinical Significance
As discussed, it is essential to understand the anatomy of the laryngeal cartilages as pathology can cause airway compromise. Pediatricians must be aware of this when dealing with epiglottitis and croup. Surgeons, anesthetists, or emergency physicians attempting to gain emergency airway access in cases of ‘cannot intubate, cannot ventilate’ require a working knowledge of the surface anatomy of the thyroid and cricoid cartilages. This knowledge allows identification of the cricothyroid membrane and a cricothyroidotomy to insert an infraglottic endotracheal tube. Otolaryngologists must have a detailed understanding of the laryngeal cartilages as anatomical landmarks during surgery and as sites of invasion of laryngeal cancer that significantly impact staging, prognosis, and management.