Introduction
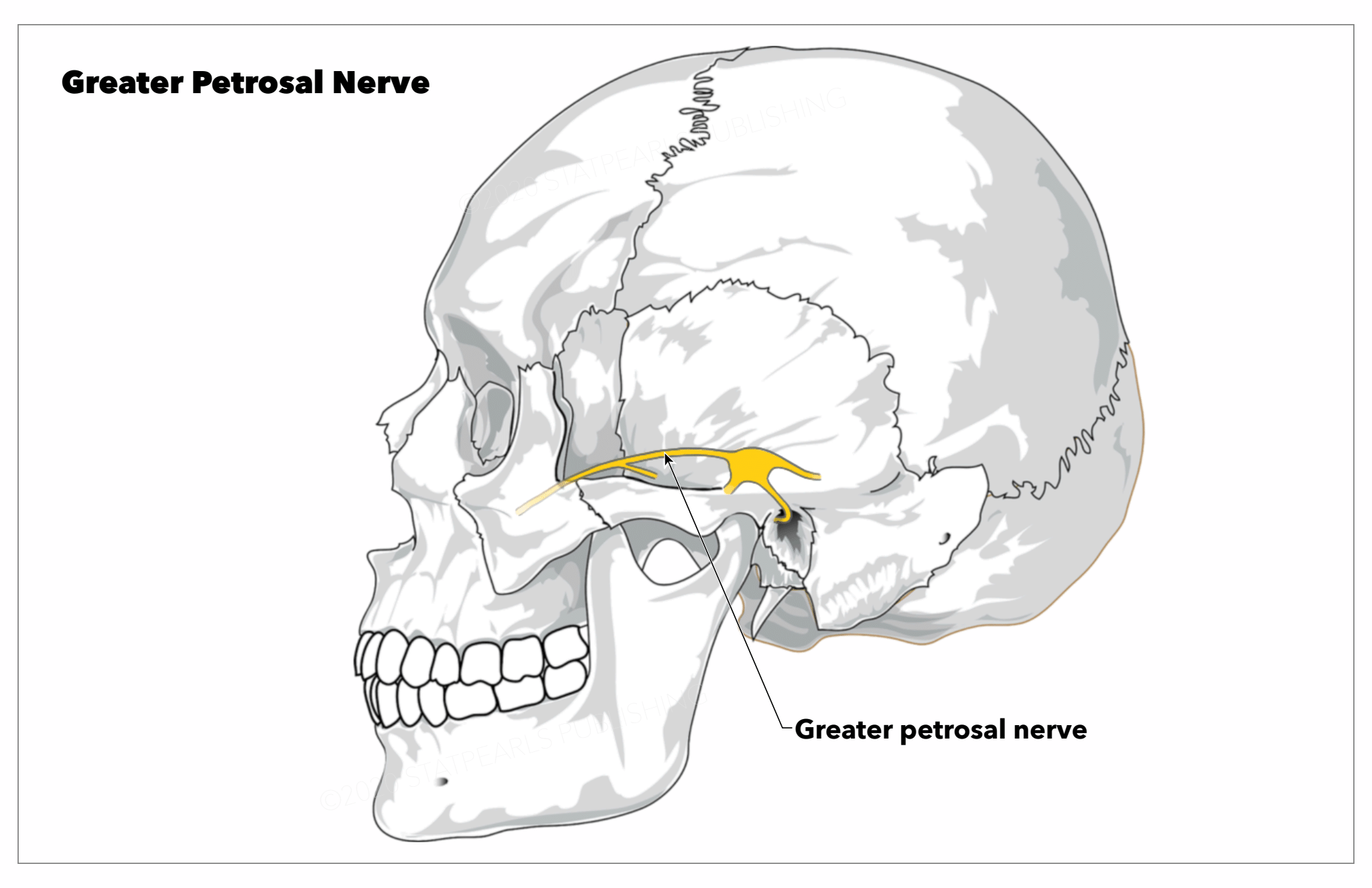
The greater petrosal nerve or superficial petrosal nerve is a branch of the nervus intermedius (nerve of Wrisberg) that carries parasympathetic, taste, and sensory fibers of the facial cranial nerve (CN VII). See Image. Greater Petrosal Nerve.
The preganglionic parasympathetic fibers develop from the superior salivatory nucleus of the tractus solitarius in the pontine tegmentum and progress in the nervus intermedius before joining the facial nerve proper.[1] These fibers transverse the geniculate ganglion without synapsing and exit the ganglion anteriorly as the greater petrosal nerve.[2] The nerve proceeds anteromedially and exits the superior surface of the temporal bone through the hiatus of the greater petrosal nerve (facial hiatus/hiatus fallopii) and into the middle temporal fossa.[3] While in the facial hiatus, this nerve travels alongside the middle meningeal artery. The greater petrosal nerve crosses the floor of the middle temporal fossa, medially to the lesser petrosal nerve and laterally to the internal carotid artery, anteromedially and slightly inferiorly passing beneath the Gasserian ganglion in Meckel’s cave and onwards towards the foramen lacerum, and the pterygoid (vidian) canal.[2][4][5][1][3] This course has led some authors to divide the nerve into four segments: the intrapetrosal segment running from the geniculate ganglion to the facial hiatus; the suprapetrosal segment running from the hiatus to the foramen lacerum; the segment of the foramen lacerum; and the segment of the pterygoid canal.[6]
In the proximal region of the pterygoid canal, the greater petrosal nerve is joined by the deep petrosal nerve, forming the nerve of the pterygoid canal - also called the Vidian nerve.[7][8] At this juncture, the Vidian nerve carries preganglionic, sensory and taste fibers from the greater petrosal, and postganglionic sympathetic fibers from the internal carotid plexus via the deep petrosal nerve. The Vidian nerve continues anteriorly within the pterygoid canal to the pterygopalatine fossa.[3] The sympathetic fibers from the deep petrosal nerve cross the pterygopalatine fossa without synapsing and provide all branches of the maxillary division of the trigeminal nerve (V2) with sympathetic innervation. The parasympathetic fibers synapse at the pterygopalatine ganglion (sphenopalatine ganglion). Postganglionic parasympathetic fibers proceed to provide secretory and vasomotor innervation to the lacrimal, nasal, and palatine glands.[5][3]