[1]
Kiliç T,Akakin A, Anatomy of cerebral veins and sinuses. Frontiers of neurology and neuroscience. 2008;
[PubMed PMID: 18004050]
[3]
Shimizu Y,Imanishi N,Nakajima T,Nakajima H,Aiso S,Kishi K, Venous architecture of the glabellar to the forehead region. Clinical anatomy (New York, N.Y.). 2013 Mar;
[PubMed PMID: 22887451]
[4]
Sugahara K,Matsunaga S,Yamamoto M,Noguchi T,Morita S,Koyachi M,Koyama Y,Koyama T,Kasahara N,Abe S,Katakura A, Retromandibular vein position and course patterns in relation to mandible: anatomical morphologies requiring particular vigilance during sagittal split ramus osteotomy. Anatomy
[PubMed PMID: 33214345]
[5]
Kagaya Y,Arikawa M,Akazawa S, Superficial Temporal Vein and Alternative Middle Temporal Vein as Recipient Veins for Free-flap Reconstruction. Plastic and reconstructive surgery. Global open. 2022 Mar;
[PubMed PMID: 35284200]
[6]
Sharma A Sr,Sharma M, Sinus Pericranii (Parietal and Occipital) With Epicranial Varicosities in a Case of Craniosynostosis. Cureus. 2022 Feb;
[PubMed PMID: 35273853]
Level 3 (low-level) evidence
[7]
Kobayashi S,Nagase T,Ohmori K, Colour Doppler flow imaging of postauricular arteries and veins. British journal of plastic surgery. 1997 Apr;
[PubMed PMID: 9176003]
[8]
Hedjoudje A,Piveteau A,Gonzalez-Campo C,Moghekar A,Gailloud P,San Millán D, The Occipital Emissary Vein: A Possible Marker for Pseudotumor Cerebri. AJNR. American journal of neuroradiology. 2019 Jun;
[PubMed PMID: 31072972]
[9]
Chang L,Zixiang Y,Zheming F,Gongbiao L,Zhichun L,Rong Z,Aidong Z,Shuzhan L, Management of pterygoid venous plexus hemorrhage during resection of a large juvenile nasopharyngeal angiofibroma: a review of 27 cases. Ear, nose,
[PubMed PMID: 23599103]
Level 3 (low-level) evidence
[10]
Adams A,Mankad K,Offiah C,Childs L, Branchial cleft anomalies: a pictorial review of embryological development and spectrum of imaging findings. Insights into imaging. 2016 Feb;
[PubMed PMID: 26661849]
[11]
Koeller KK,Alamo L,Adair CF,Smirniotopoulos JG, Congenital cystic masses of the neck: radiologic-pathologic correlation. Radiographics : a review publication of the Radiological Society of North America, Inc. 1999 Jan-Feb;
[PubMed PMID: 9925396]
[12]
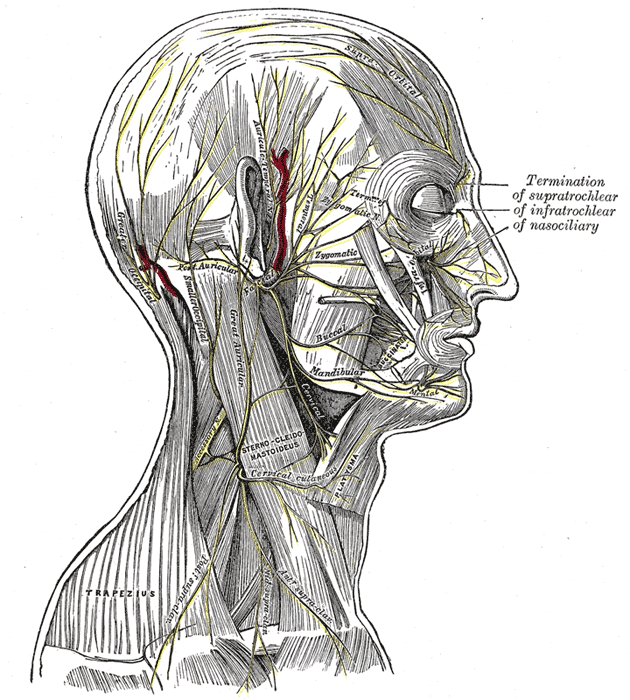
Kemp WJ 3rd,Tubbs RS,Cohen-Gadol AA, The innervation of the scalp: A comprehensive review including anatomy, pathology, and neurosurgical correlates. Surgical neurology international. 2011;
[PubMed PMID: 22276233]
[13]
Chen Z,Feng H,Zhu G,Wu N,Lin J, Anomalous intracranial venous drainage associated with basal ganglia calcification. AJNR. American journal of neuroradiology. 2007 Jan;
[PubMed PMID: 17213417]
[14]
Gulmez Cakmak P,Ufuk F,Yagci AB,Sagtas E,Arslan M, Emissary veins prevalence and evaluation of the relationship between dural venous sinus anatomic variations with posterior fossa emissary veins: MR study. La Radiologia medica. 2019 Jul;
[PubMed PMID: 30825075]
[15]
Yoon J,Puthumana JS,Nam AJ, Management of Scalp Injuries. Oral and maxillofacial surgery clinics of North America. 2021 Aug;
[PubMed PMID: 34092461]
[16]
Scalp Arteriovenous Malformation (Cirsoid Aneurysm) in Adolescence: Report of 2 Cases and Review of the Literature., Li D,Heiferman DM,Rothstein BD,Syed HR,Shaibani A,Tomita T,, World neurosurgery, 2018 Aug
[PubMed PMID: 29864562]
Level 3 (low-level) evidence
[17]
Matsushige T,Kiya K,Satoh H,Mizoue T,Kagawa K,Araki H, Arteriovenous malformation of the scalp: case report and review of the literature. Surgical neurology. 2004 Sep;
[PubMed PMID: 15336874]
Level 3 (low-level) evidence
[18]
Lee SJ,Kim JK,Kim SJ, The clinical characteristics and prognosis of subgaleal hemorrhage in newborn. Korean journal of pediatrics. 2018 Dec;
[PubMed PMID: 30304906]
[19]
Caranfa JT,Yoon MK, Septic cavernous sinus thrombosis: A review. Survey of ophthalmology. 2021 Nov-Dec;
[PubMed PMID: 33831391]
Level 3 (low-level) evidence
[20]
Matthew TJH,Hussein A, Atypical Cavernous Sinus Thrombosis: A Diagnosis Challenge and Dilemma. Cureus. 2018 Dec 4;
[PubMed PMID: 30761237]