Introduction
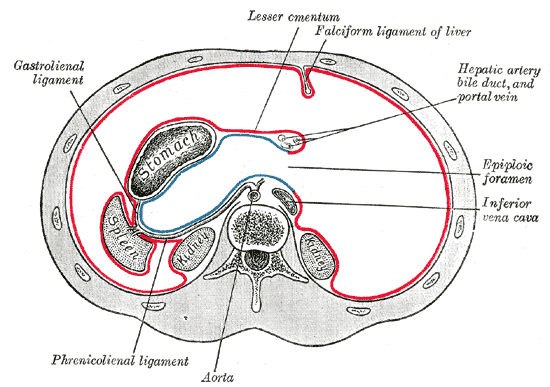
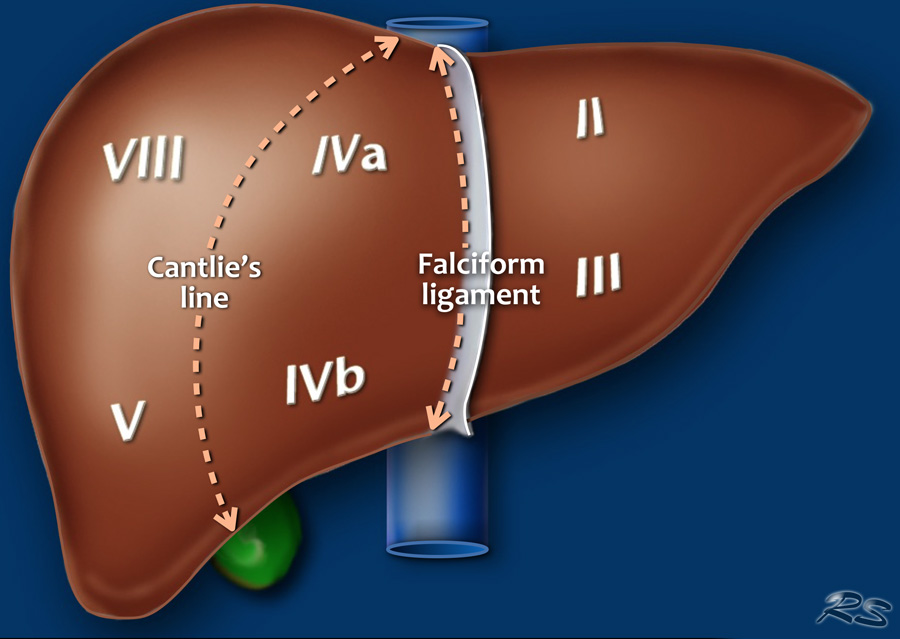
The falciform ligament is the thin, sickle-shaped, fibrous structure that connects the anterior part of the liver to the ventral wall of the abdomen. It can be seen drooping from the liver hilum when looking inside the abdomen during surgery. The falciform ligament attaches to the liver between the right and left lobes as well as attaching to the inferior diaphragmatic surface. The free, inferior border of the falciform ligament contains the paraumbilical veins and the round ligament of the liver (aka, ligamentum teres hepatis) which courses along a fissure situated between the inferior surface of the right and left lobes. Paraumbilical veins become prominent and more patent during portal hypertension when the portal vein, draining the gastrointestinal system, becomes engorged with blood which is unable to fully enter the liver. If the portal hypertension is severe enough, the paraumbilical veins will form a caput medusa of engorged blood vessels surrounding the umbilicus. The presence of a caput medusa is a stigmata of portal hypertension and severe liver dysfunction as seen in end-stage liver disease. (Note: When using the shorthand term of “round ligament” vs. “round ligament of the liver,” the term must not be confused with the round ligament of the uterus.)