Introduction
The sacroiliac (SI) joint articulates surfaces of the sacrum and the ilium and functions as the transition between the spine and the pelvis. The main roles of the SI joint are to provide stability and offset the load of the trunk to the lower limbs. The stability of the joint is provided by an extensive architecture of ligamentous structures. [1][2][3][4]
Structure and Function
The SI joint is a diarthrodial synovial joint. It is surrounded by a fibrous capsule containing a joint space filled with synovial fluid between the articular surfaces. The articular surface is made up of two, strong, C-shaped layers. It is distinguished from other synovial joints by the unusual articulation of two different types of cartilage. The sacral capsular surface is composed of hyaline cartilage while the iliac capsular surface is composed of fibrocartilage. There are three main types of cartilage found in the body: hyaline, fibrocartilage, and elastic. Hyaline cartilage is made from type II collagen and is the weakest type of cartilage. Fibrocartilage is made from type I collagen and is the strongest type of cartilage.
The SI joint is also unique in that its articular surfaces have multiple ridges and depressions that develop and deepen over one's lifetime. During the natural bone maturation process, the morphology and characteristics of the sacroiliac joint change. The joint surfaces are relatively flat in early life and allow for a gliding motion between the sacrum and ilium in all directions. However beginning in the second and third decades of life, the sacroiliac joint surfaces develop distinct angulations and lose their flat surface. The joint develops an elevated ridge along the iliac surface and a depression along the sacral surface. This produces a functional interlocking between the 2 bones. This interlocking limits the movement at the SI joint which creates the overall stability of the joint. This increase in the sacroiliac joints’ stability makes dislocations very rare.[5][6]
Biomechanically, the sacroiliac joint performs several functions. Primarily, its purpose is to attenuate the distribution of force loads from the lower extremities. It functions both as a shock absorber for the spine above and converts torque from the lower extremities into the rest of the body. The primary plane of motion is anterior-posterior along a transverse axis. Nutation refers to anterior-inferior movement of the sacrum while the coccyx moves posteriorly relative to the ilium. Counternutation refers to a posterior-superior movement of the sacrum while the coccyx moves anterior relative to the ilium. In most individuals, this motion is limited to 2 to 4 mm of movement due to the bony architecture and ligamentous structures of the joint.
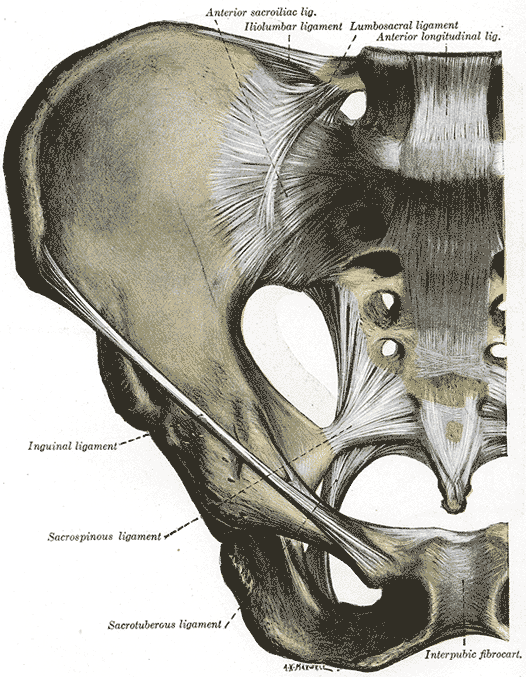
A strong ligamentous architecture stabilizes the SI joint. The interosseous sacroiliac ligament forms the major connection between the sacrum and the ilium. It is the strongest ligament in the body and prevents anterior and inferior movement of the sacrum. The posterior (dorsal) sacroiliac ligament connects the posterior-superior iliac spine (PSIS) and the iliac crest to the third and fourth segments of the sacrum. The ligament resists counternutation and can be palpated directly below the PSIS. The sacrotuberous ligament blends with the posterior sacroiliac ligament and functions to resist nutation of the joint. The sacrotuberous ligament then passes behind the sacrospinous ligament. The sacrospinous ligament originates on the ischial spine and attaches to the lateral sacrum to oppose the nutation of the sacrum during weight-bearing and gait. The presence of the sacrotuberous and sacrospinous ligaments creates the greater sciatic foramen and the lesser sciatic foramen. These ligaments help prevent flexion and rotation of the ilium past the sacrum. Of note, the pudendal nerve lies between these two ligaments and may become entrapped, leading to perineal pain. The anterior sacroiliac ligament is an anterior-inferior thickening of the fibrous capsule that is not as well defined as other SI ligaments. It is the thinnest of all ligamentous structures and most vulnerable to injury making it a common source of pain.
Embryology
At two months of gestational age, the sacroiliac joint can be identified. At this time, a well-formed articular joint can be identified with a thin and pliable capsule anteriorly. The stability of the immature joint is provided by the posterior ligamentous architecture. The joint surfaces are smooth and flat which allows for ample gliding movement in all directions. At five months of gestational age, a thin fibrous septum joins the two surfaces. At 37 weeks gestation, a synovial membrane lines the joint capsule. The cartilage on the sacral side is 3-5 times thicker than the iliac side at this point of development. The two distinct cartilage types can be identified. The iliac cartilage consisting of hyaline cartilage and the sacral sides consisting of fibrocartilage. During the first decade of life, the joint grows proportionally and the capsule develops into a tough, fibrous structure. The articular surfaces of the joint remain flat and allow for gliding motion in all directions. In the second and third decades of life, the articular surfaces begin to become uneven and the iliac surface has a convex ridge that runs in a sacral groove. The posterosuperior to anteroinferior motion is limited by this bony development. [7]
Blood Supply and Lymphatics
The common iliac artery bifurcates into the external and internal iliac artery. The origin of the internal iliac artery is commonly found at the spine levels L5-S2 anteriorly and superiority to the sacroiliac joint. The superior gluteal artery is found posteriorly to the sacroiliac joint at the spine levels of S2-S3.
Many blood vessels supply the sacroiliac joint. The posterior aspect is supplied by the median sacral artery and lateral sacral artery which arise from the internal iliac. The anterior aspect is supplied by the iliolumbar artery which originates either from the internal iliac or common iliac artery. The venous drainage of the joint flows into the internal iliac vein thus correlating to the arterial supplies described above. [8]
Nerves
The sacroiliac joint is well innervated but the pattern of innervation varies among individuals. The sacroiliac joint receives its innervation from the ventral rami of L4 and L5, superior gluteal nerve, and dorsal rami of L5-S2. The nerve supply to the SI joint varies between individuals and innervation may be almost exclusively derived from the sacral dorsal rami. This may account for the variable patterns of referred pain from the SI joint.
Physiologic Variants
Accessory sacroiliac joints have been reported in the current literature. These accessory joints are additional articular facets found within the primary sacroiliac joint. The accessory joints have their own capsule, cartilage and synovial membrane. There is a wide range of prevalence with an accessory joint found in 8-40% of dissected specimens. The accessory joints are found most commonly in men, on the right side of the body, and in older individuals. Although rare, individuals can have multiple accessory joints. [8]
Clinical Significance
The incidence of lower back pain originating from the sacroiliac joint may be as high as 27%. Patients often describe a specific trauma or inciting event, although this is not always true. Pain originating from the sacroiliac joint is likely more common than most providers realize due to difficulty in localizing symptoms and referred pain patterns. Using a pain diagram to map out the location of the pain is often very helpful in diagnosis. SI joint pain is commonly found 10 cm caudally and 3 cm laterally from the patient's posterior superior iliac spine. SI joint pain is commonly referred to the buttocks, lower lumbar region, groin, and lateral thigh. Patients with sacroiliac joint dysfunction describe their pain being aggravated by getting out of a chair, prolonged standing or sitting, with climbing stairs or morning stiffness. Numbness and tingling in the leg may also be present. Risk factors for sacroiliac joint pain include leg length discrepancy, age, arthritis, history of spine surgery, pregnancy, and trauma.[9][10][11]
The potential differential diagnosis of lower back pain is extensive. Therefore the clinical examination of the patient with sacroiliac joint dysfunction begins with an evaluation of gait, leg-length inequality, and examination of the lower lumbar region. During a physical examination, localization over the SI joint should be attempted using the Fortin finger test. The test is considered positive when the point of tenderness is within 2 cm inferomedial to the posterior superior iliac spine. In addition to the physical exam maneuvers above, the hip joint and spine should be properly evaluated to rule out other pathologies. [12]
Sacroiliac Joint Dysfunction
Sacroiliac joint dysfunction is a broad term that refers to the abnormal biomechanical function of the SI joint. Some causes of sacroiliac joint dysfunction include the following:
Trauma
Increased mobility of the SI joint may be the result of injury to the supporting ligaments. This can be seen in high impact injuries such as a motor vehicle accident, fall, or repetitive trauma from weight lifting or sports.
Hypermobility
Hypermobility can also be genetic, a term often labeled "multidirectional instability" for ligamentous laxity at multiple joints, not strictly the sacroiliac joint. Other causes of inherited laxity can include Marfan syndrome and Ehlers-Danlos syndrome.
Hormonal changes may also cause hypermobility. The ligaments of the sacroiliac joint slacken during pregnancy due to the hormone relaxin. This loosening, along with that of the related symphysis pubis, permits the pelvic rim to widen during the birthing process. The ligaments may also be stretched due to increased lumbar lordosis. Therefore, SI joint pain is common in pregnancy. However, this pain may persist after pregnancy if the ligaments do not return to physiologic tension. Risk factors include extended labor and delivery of large babies.
Degeneration
Structural abnormalities of the SI joint may also cause dysfunction. Individuals with altered gait patterns, spinal deformities or leg-length discrepancies can have reduced interlocking ability leading to laxity and pain. This equates to repetitive and uneven stress to the SI joint articular surfaces, causing laxity and pain.
Osteoarthritis of the SI joint is also common, and the incidence increases with age. Other risk factors for osteoarthritis include previous trauma.
Inflammation
Inflammation of the sacroiliac joints is termed sacroiliitis. There are many causes of sacroiliitis, with some mentioned above. An infectious cause of sacroiliitis includes the presentation of arthritis from brucellosis. Sacroiliitis may also be related to other inflammatory conditions such as inflammatory bowel disease and seronegative spondyloarthropathies. [13]