Continuing Education Activity
Coronary artery anomalies (CAAs) are a varied group of congenital disorders that refer to abnormalities involving the origin, course, and structure of the coronary arteries. This activity outlines and reviews the etiology, epidemiology, pathophysiology, evaluation, and treatment of isolated coronary artery anomalies. It also highlights the role of the interprofessional team in improving care for patients with this condition.
Objectives:
- Identify the pathophysiology of isolated coronary artery anomalies.
- Review the evaluation of coronary artery anomalies.
- Summarize the management guidelines for isolated coronary artery anomalies.
- Explain some interprofessional team strategies for improving care coordination and communication to advance isolated coronary artery anomalies and improve outcomes.
Introduction
Coronary artery anomalies (CAAs) are a varied group of congenital disorders that refer to abnormalities involving the origin, course, and structure of the coronary arteries. By definition, anomalies are a coronary feature or pattern that is present in less than 1% of the general population.[1] In the era of coronary angiography and advanced cardiac imaging, more of these disorders are being diagnosed, and more variants are being described. Knowledge of normal and variant anatomy is becoming increasingly vital. Variations in coronary anatomy are commonly seen in association with congenital heart disorders. Coronary artery normal and abnormal development has been reviewed in recent years.[2] This article, however, will be focused on coronary artery anomalies in the absence of congenital disorders (i.e., isolated coronary artery anomalies).
Etiology
The exact pathogenetic mechanisms for the development of coronary artery anomalies (CAAs) are not well understood. Extensive embryological research has been done and has provided us with some clues into the formation of coronary anomalies. Coronary artery development is an intricate process that is dependent on many factors. These factors include the formation of coronary sinuses on the embryologic bulbus cordis that later becomes the aorta, formation of cardiac sinusoids, the formation of coronary arteries in the epicardial atrioventricular and interventricular grooves that eventually meet up with the coronary buds, and the matching of the coronary arteries to their sinuses of origin.[3][4] A defect in any one of these systems can lead to anomalies in the coronary circulation.
Epidemiology
Since the advent of advanced cardiac imaging, such as coronary computed tomographic (CT) angiography and cardiac magnetic resonance angiography, the incidence of coronary artery anomalies in the population has increased dramatically. It is suggested that important coronary artery anomalies are present in 1,300,000 of the U.S. population and are one of the main causes of sudden cardiac death. In the past, the incidence has generally been reported as 1%, but in a recent prospective angiographic study of 1950 cases, it is determined that the true incidence is around 5.6%.[5] It may be difficult to generalize this to the population, but it indicates that the incidence is higher than what was previously believed. No racial or sexual predisposition is yet known. Anomalous origin of coronaries is found in 12% to 33% of young athletes with sudden cardiac death (SCD) at autopsy.[6]
Pathophysiology
Normal Coronary Anatomy
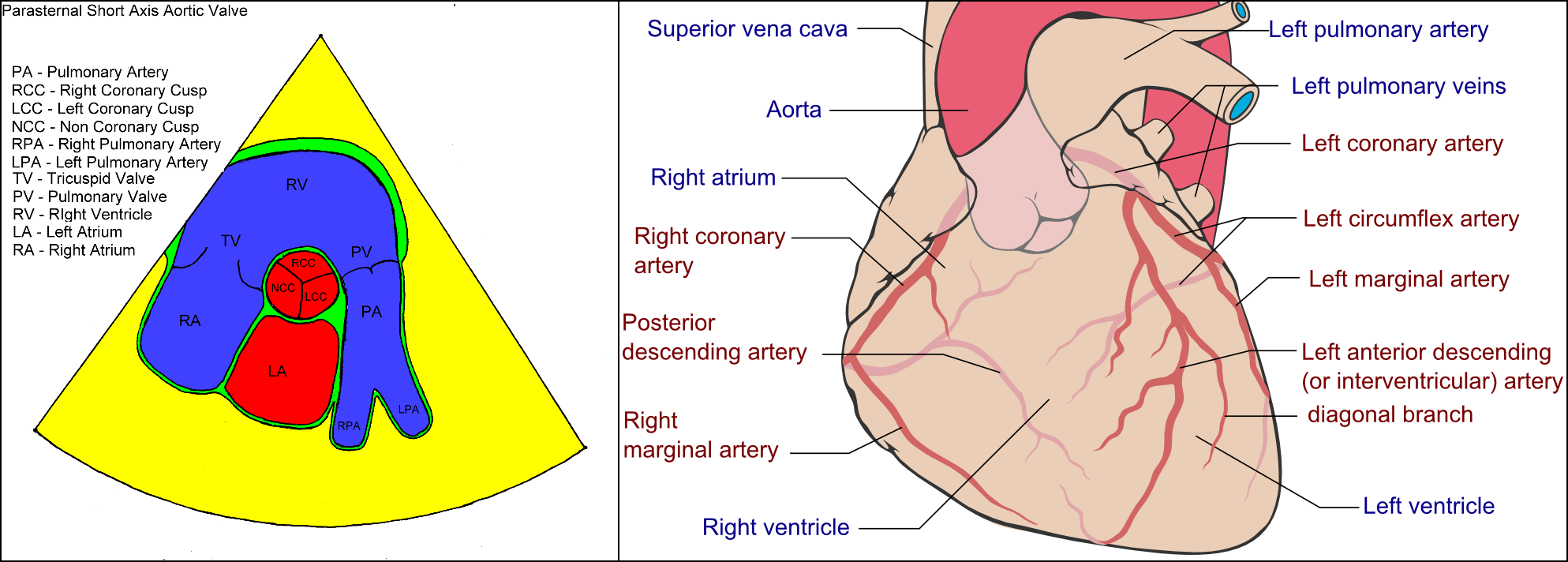
The coronary arteries arise from the aortic sinuses as two main branches, the right coronary artery, and the left main coronary artery. The right coronary artery (RCA) arises from the right sinus of Valsalva (RSV), whereas the left main coronary artery (LM) arises from the left sinus of Valsalva (LSV) (image 1). The LM passes between the main pulmonary artery and the left auricle and further divides into the left anterior descending (LAD) and left circumflex (LCX). The LAD courses down towards the apex of the heart via the anterior interventricular sulcus. It will further give rise to the diagonal and septal branches and supply the anterior wall and the anterior half of the interventricular septum. The LCX courses through the coronary sulcus and onto the diaphragmatic cardiac surface give rise to one or more obtuse marginal branches and supply the lateral wall.[7][3]
After its origin, the RCA courses through the right atrioventricular sulcus to the acute margin of the heart and then continues posteriorly into the diaphragmatic surface and base of the heart. The RCA gives rise to the atrial branch, SA nodal, and AV nodal branches and supplies the right atrium, right ventricle, sinoatrial (SA) and atrioventricular (AV) nodes, the interatrial septum, portion of the left atrium, posterior one-third of the interventricular septum, and a portion of the posterior part of the left ventricle.[3]
Many variations exist in the coronary anatomy and are considered normal. One such example is that of coronary dominance. The artery that supplies the posterior descending artery (PDA) and the posterolateral branch determines coronary dominance. In most individuals (70% of cases), the PDA arises from the RCA, which makes it a right dominant system. If the supply is from the LCX, then it is considered a left dominant system (10% of cases). Co-dominance is also possible in about 20% of cases. The dominant artery usually also supplies the AV nodal branches. Variations can exist within that as well.[3]
There exist a number of variations in regards to the blood supply of the inferior wall. The supply can be from PDA, distal RCA, LCX, obtuse marginal branches of the LAD, or “wraparound LAD.”[3]
Another variance is not in the origin of the coronary arteries but in their course. Coronary arteries typically are surrounded by epicardial fat. In some cases, coronaries can dip into the myocardium for a variable length. This phenomenon is known as myocardial bridging and can be found in up to 25% of patients. The clinical significance of this is controversial and is thought to be dependent on the length and depth of the myocardial bridge. Systolic contraction of the myocardium can result in compression of the coronary artery and may cause myocardial ischemia and angina.[3]
In about 2% of the population, the angle between the LM and the LCX can be less than 45 degrees. This phenomenon is known as the acute take-off of LCX. This can cause technical difficulties during invasive coronary angiographic procedures.[3]
High take-off of the coronary ostium can also exist and is considered a normal variant. This is defined as the position of the coronary ostium 5 mm above the aortic sinotubular junction. The RCA is most frequently implicated and is present at increased frequency in those with a bicuspid aortic valve. The higher the position, the higher the risk of coronary hypoperfusion as the coronary sinuses facilitate optimal diastolic coronary perfusion.[3]
Coronary Artery Anomalies
Many different classifications have been proposed, but no single universal one exists. We will describe anomalies associated with each artery in turn rather than use these classifications for practical reasons.
Left Circumflex Anomalies
LCX can originate from the left or right sinus of Valsalva, or the RCA. These anomalies are relatively common and usually benign.
Right Coronary Artery Anomalies
RCA can have its origin from the left sinus of Valsalva with an incidence of about 0.1%. When this happens, the RCA will course between the aorta and the pulmonary artery, and due to this, it is implicated in sudden cardiac death. Some recent studies have reported a prevalence of about 30% in young individuals who have suffered sudden cardiac death.[8]
Left Main Coronary Artery Anomalies
The left main can be absent, leading to split origin or separate ostia of the LAD and the LCX, and usually, this is of no clinical significance. LM can have an anomalous origin from the right sinus of Valsalva, which is quite rare, with a reported incidence of 0.03-0.15%.[9] This is considered clinically significant due to the course that the LM coronary artery takes when it arises from the opposite sinus, and it is associated with sudden cardiac death, especially during vigorous exercise.[10] LM can have an anomalous origin from the pulmonary artery, which is rare (incidence of 1 in 300,000 live births) but very significant as, if not corrected with surgery, it can lead to death within the first year of life.[11]
Left Anterior Descending Artery Anomalies
The origin of the LAD can be from the RCA, the right sinus of Valsalva, the latter with a reported incidence of about 0.03%.[12] There can be a duplication of the LAD, which has been reported in a case series but is not associated with sudden cardiac death.
Anomalies of the LM coronary artery have been most implicated in sudden cardiac death, and many mechanisms for this have been presented. Normally LM originates from the LSV at an angle perpendicular to the aorta. If the anomalous LM arises from the opposite coronary sinus, then it comes off at an acute angle and has sharp bends. During exertion, the aortic root expands and further exaggerates the angle leading to compression and subsequent ischemia.
If the anomalous artery is between two major vessels such as RCA originating from the LSV, then overexpansion of the aorta and pulmonary artery from hypertension can cause extrinsic compression and ischemia. Angelini et al. have demonstrated with intravascular ultrasound the compression of the anomalous artery when it courses between the great vessels.[1] Some authors also suggest endothelial damage in anomalous coronaries leading to vasospasms, which can also be a contributing factor to myocardial ischemia.
History and Physical
The majority of adults with coronary artery anomalies (CAAs) are asymptomatic, and the first presenting symptom usually is sudden cardiac death. In addition, patients can also present with myocardial ischemia and congestive heart failure. In less than 30% of patients, symptoms may be reported as anginal chest pain at a relatively young age, syncope with exercise, dyspnea on exertion, palpitations, and fatigue. Most often, however, the relationship between the anomaly and the presenting symptoms is not clear, and these symptoms rarely raise suspicion for coronary artery anomaly (CAA).
Evaluation
Most patients with coronary artery anomalies (CAAs) either die suddenly or have no characteristic presentation and are asymptomatic for a large portion of their lives. An atypical chest pain syndrome is the most common reason they are referred for coronary angiography, where CAAs are usually diagnosed.[5] Due to this, a screening protocol has been difficult to establish. If a CAA is suspected, a stepwise approach should be used for diagnosis going from least invasive to most invasive. Focused expert echocardiography (transthoracic and, if needed, transesophageal) with Doppler can be used to identify the anatomy of the coronaries but lacks functional evaluation.[13] Echocardiography, however, is not the most reliable means to diagnose the disorder. A prospective study by Frommelt et al. noted the incidence of a specific type of CAA (anomalous coronary artery from the opposite sinus) to be 0.17% when examining a series of routine echocardiograms whereas the incidence was 1.07% when found by coronary angiography.[14][15]
Other non-invasive tests include coronary computed tomographic angiography (coronary CT angiography) and cardiac magnetic resonance angiography (CMRA). Reports regarding the use of these modalities to diagnose CAAs have been encouraging, especially since three-dimensional reconstructions of the coronary anatomy can be now done. Currently, coronary CT angiography is the gold standard in diagnosing CAAs.[3] A recent study showed that the prevalence of CAAs is much higher with CT than with coronary angiography, which suggests a possible underestimation of CAAs when using invasive coronary angiography.[16] Both of these modalities use intravenous contrast agents that carry significant side effects in certain patient populations, especially those with renal disease. CT angiography exposes patients to relatively high doses of ionizing beam radiation. In contrast, CMRA does not and thus is the preferred imaging modality in younger patients if echocardiography fails to yield a diagnosis. CMRA is good for visualizing the origin of the coronaries, but due to lack of spatial resolution, the capability of this modality in visualizing anomalies in smaller coronary branches is still a limiting factor.[3]
For those with identified CAAs, nuclear stress test should be done to evaluate for effort-induced ischemia, scars and, most importantly, to establish a baseline for follow-up in case intervention is needed in the future.[5] If any symptoms are present in a patient with known CAAs, invasive coronary angiography with intravascular ultrasound (IVUS) is indicated to determine whether intervention is needed.[1]
Treatment / Management
Management of coronary artery anomalies (CAAs) remains controversial. Coronary artery anomalies contain many entities, and no one group has collected large enough data to clarify the natural prognosis of each entity, which contributes to the difficulty in understanding their clinical implication. With that in mind, the consensus is that the decision process should be individualized, taking into account the symptoms and the type of anomaly. Patients with high-risk anomalies, such as those with arteries that arise from the opposite coronary sinus should be restricted from excessive and unnecessary exertion. As mentioned before, patients should have an evaluation with a nuclear stress test to evaluate for reversible ischemia and coronary angiography with IVUS to determine the degree of stenosis, area of dependent myocardial territory, and risk of sudden cardiac death. Patients then have three treatment options: conservative management with medical treatment and observation, coronary angioplasty with stenting, or surgical correction.[5] Surgical correction is preferred in young patients over percutaneous intervention (PCI) due to limited data available on the success of PCI in this patient population. PCI can be considered in older adults who present with CAAs.[7]
Differential Diagnosis
The symptoms of isolated coronary artery anomalies (CAAs) mimic other disorders of coronary arteries and heart. Following differentials should be kept in mind while evaluating a patient of CAAs.
- Coronary artery atherosclerosis
- Dilated cardiomyopathy
- Hypertrophic cardiomyopathy
- Myocardial ischemia
- Pulmonary embolism
- Valvular dysfunctions
- Ventricular arrhythmias
Prognosis
As previously mentioned, the prognosis is dependent on the type of anomaly. Most anomalies are clinically benign and do not affect the outcomes of patients. Some are associated with sudden cardiac death, myocardial ischemia, early endocarditis, and congestive heart failure. The most common anomalies associated with SCD are the origin of the left main coronary artery from the right sinus of Valsalva and the origin of the right coronary artery from the left sinus of Valsalva.[8]
Complications
Coronary artery anomalies (CAAs) are known to be associated with sudden death, myocardial ischemia, endocarditis, and congestive heart failure. They also cause difficulty during cardiac procedures such as coronary angiography, percutaneous coronary intervention, and cardiac surgery. CAAs are the second most common cause of sudden cardiac death in athletes and military recruits.[1][8] Myocardial ischemia can occur in those with anomalous origin of the left coronary artery and sometimes the right coronary artery when it originates from the pulmonary artery or the right ventricle. Some CAA can result in fistulas, which can alter hemodynamics. Large coronary artery fistulas can cause shunting, which can result in volume overload. This can result in congestive heart failure. Coronary artery fistulas may also result in an increased risk for endocarditis, depending on the location.
Deterrence and Patient Education
Young fit athletes who develop symptoms of dyspnea, angina, syncope, and palpitations should go to a healthcare provider promptly for evaluation to prevent adverse outcomes like sudden cardiac death. Those with coronary artery anomalies should consult with an interprofessional team including interventional cardiology, cardiac surgery, and congenital heart specialist for best options for evaluation and treatment. Avoid strenuous activity until correction of the anomaly is performed.
Enhancing Healthcare Team Outcomes
Coronary artery anomalies (CAAs) are a complex condition that remains a top cause of sudden cardiac death in young athletes. Evaluation and management guidelines are limited and controversial. Management of this condition requires a multidisciplinary approach with close patient follow-up. The primary care provider (PCP) is the first point of medical contact for most patients experiencing symptoms. The PCP should take a detailed history and be careful not to dismiss young fit patients with the aforementioned symptoms easily and, if appropriate, refer the patient to a specialist. For those with diagnosed CAAs, an interprofessional team of interventional cardiologists, cardiac surgeons, and congenital heart defect specialists should be established to determine the course of treatment and enhance and improve outcomes. For those who have undergone surgical correction, post-op nursing care is extremely important for the prevention of surgical site infections. Cardiac rehabilitation has proven to be extremely effective in regaining function after surgery, so a physical and occupational therapist should be involved early on in the postoperative period.