Continuing Education Activity
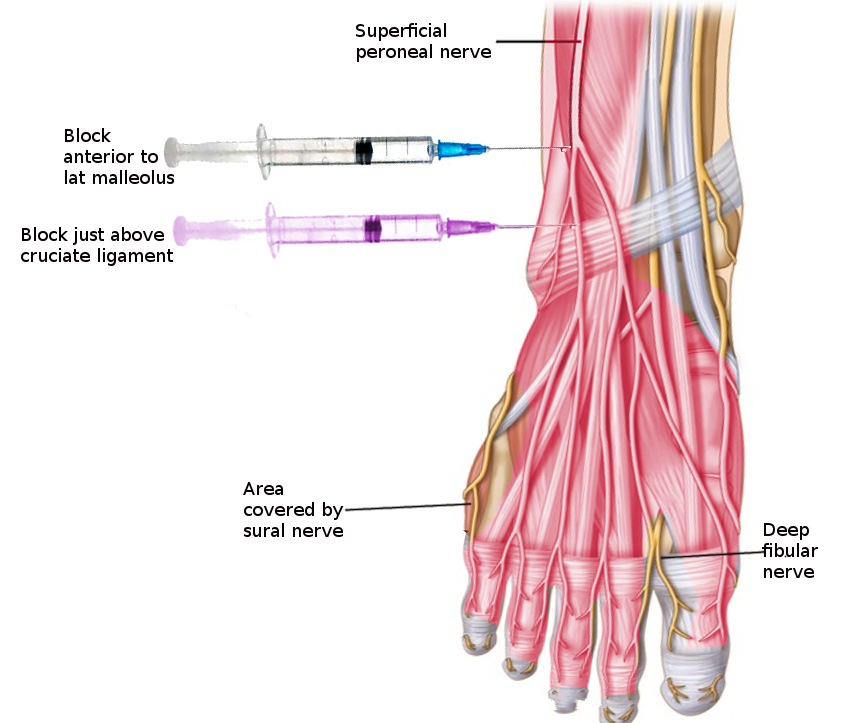
The superficial peroneal nerve (superficial fibular nerve) is a mixed nerve that carries sensory information from the anterolateral aspect of the leg and the greater part of the dorsum of the foot (except for the first web space). Entrapment of the superficial peroneal nerve is not uncommon and can present with pain in the sensory distribution of the nerve with or without paresthesia. Block of the superficial peroneal nerve provides relief of symptoms of the entrapment and also provides anesthesia for surgical procedures involving the dorsum of the foot. It is better to perform the block under ultrasound guidance to avoid collateral damage of the neurovascular structures and get a more effective block. This activity reviews the use of a superficial peroneal nerve block and highlights the role of the interprofessional team in using this technique.
Objectives:
- Describe the anatomy and anatomic variations of the superficial peroneal nerve.
- Outline a practical approach to diagnose the entrapment of the superficial peroneal nerve and ability to differentiate it from other causes of anterolateral leg pain.
- Describe land-mark and ultrasound-guided interventions for the management of the entrapment of the superficial peroneal nerve.
- Explain the importance of improving care coordination among the members of the interprofessional team to enhance the delivery of care for patients who are receiving a superficial peroneal nerve block.