Continuing Education Activity
Peripheral neuropathy is a condition present in a wide range of etiologies. Of these etiologies, diabetes remains the most common cause of peripheral neuropathy, with about 50% of diabetic patients experiencing some form of peripheral neuropathy. However, many patients also experience peripheral neuropathy secondary to other etiologies, making the diagnoses and treatment of these conditions difficult. Although other forms of non-invasive testing are available, once these have been exhausted the sural nerve biopsy becomes a valuable option for potential diagnosis and treatment. In this activity, we will discuss the anatomy, indications, procedural technique, complications, and follow up needed for a sural nerve biopsy.
Objectives:
- Identify the anatomical structures, indications, and contraindications of a sural nerve biopsy.
- Describe the equipment, personnel, preparation, and technique in regards to a sural nerve biopsy.
- Review appropriate evaluation of the potential complications and clinical significance of a sural nerve biopsy.
- Summarize the guidelines for sural nerve biopsy.
Introduction
Peripheral neuropathy is a condition present in a wide range of etiologies. Of these etiologies, diabetes remains the most common cause of peripheral neuropathy, with about 50% of diabetic patients experiencing some form of peripheral neuropathy.[1] However, many patients also experience peripheral neuropathy secondary to other etiologies, making the diagnoses and treatment of these conditions difficult. Although other forms of non-invasive testing are available, once these have been exhausted the sural nerve biopsy becomes a valuable option for potential diagnosis and treatment.[2] This activity discusses the anatomy, indications, procedural technique, complications, and follow up needed for a sural nerve biopsy.
Anatomy and Physiology
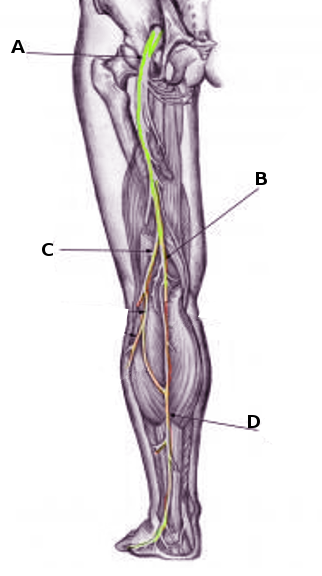
The sural nerve provides sensory feedback from the lateral ankle and foot. It forms from two branches of periphery nerves: the tibial nerve and the peroneal nerve. Around the level of the gastrocnemius muscle origin, the medial sural cutaneous nerve branches from the tibial nerve. This branch merges with the lateral sural cutaneous nerve, which is a branch of the common peroneal nerve given off around the level of the fibular head. Although variations in anatomy can be present, one study showed that 85% of cadaveric specimens had these innervations.[3] The combined sural nerve then travels down the posterior/lateral leg, diving deep and posterior to the fibular malleolus before it terminates at the level of the fifth metatarsal tuberosity as the lateral dorsal cutaneous nerve.[4]
During the harvesting of the sural nerve, the surgeon will also encounter the lesser saphenous vein. This vein originates at the level of the venous arch of the foot around the fifth digit, courses posteriorly and laterally with the sural nerve, and terminates between the heads of the gastrocnemius muscle into the popliteal vein.[5]
The sural nerve typically functions as a purely sensory nerve, although some studies have found small motor fibers in post-mortem biopsy.[6] This quality, along with its ease of access, make it an attractive option for harvesting and/or biopsies.
Indications
Due to morbidity associated with a sural nerve biopsy, all conservative diagnostic techniques must be exhausted before performing a biopsy. These include a thorough patient history and physical examination, electromyography, nerve conduction velocity, and others. Bevilacqua et al. recommended that once these methods are exhausted, a biopsy should be performed only if the condition meets three criteria[1]:
- There is evidence that the condition might be different than diabetic peripheral neuropathy
- The disease suspected causes histopathological changes in the nerve
- The biopsy results will change the treatment plan
As a valuable diagnostic tool for over 50 years, conditions possibly warranting a sural nerve biopsy include[7][8][9]:
- Vasculitic neuropathy as the diagnosis responds well to immunosuppressive agents.
- Neuropathy secondary to leprosy
- Chronic inflammatory demyelinating neuropathy
- Hereditary sensory-motor neuropathy
- Acute and chronic axonopathy
- Demyelinating neuropathies
Contraindications
Absolute contraindications for the procedure include the presence of active infection, arterial insufficiency, neuropathy explained by more likely causes, and others.
Equipment
No special equipment is needed to perform a sural nerve biopsy. Standard instrumentation such as a scalpel, retractors, forceps, and suture material may be used during the biopsy. Microsurgical loupes may assist the surgeon during the procedure. A tourniquet is typically not used, but a bipolar cautery is an option for hemostasis. The laboratory receiving the specimen should be contacted before procurement as each facility may differ in their requirements for analysis.
Personnel
The procedure can be performed by a variety of professionals including general surgery, neurosurgery, podiatry, orthopedics, and others. A team approach is always recommended for optimal patient outcomes.
Preparation
All less invasive methods must be exhausted before performing the sural nerve biopsy due to the morbidity associated with the procedure.
Comprehensive patient history and physical exam should be performed, including the identification of nerves affected and functional ability.
Laboratory workup should include a complete blood count, comprehensive metabolic panel, rheumatologic panel, as well as lab tests tailored towards specific diagnoses. For example, if vasculitic neuropathy is suspected, inflammatory markers such as C-reactive protein (CRP), erythrocyte sedimentation rate (ESR), urinalysis, and others may be ordered. Additionally, if diabetic peripheral neuropathy is suspected a hemoglobin A1c level, glucose level, kidney function, and other markers should be ordered.
Nerve conduction velocity testing and advanced imaging (such as ultrasound or MRI to potentially identify diseased nerve segments) should be ordered or performed.[10] Consultation with the patient's other managing services such as neurologists or neurosurgeons can assist in establishing the highest possible level of care.
Finally, the patient should be educated regarding the risks, benefits, and expected outcomes after the procedure to establish reasonable expectations in the post-operative state.
Technique or Treatment
Typically, the procedure begins at the posterior aspect of the fibula. A modified approach has been described in the proximal calf to minimize complications.[11] The patient can be positioned prone for ease of access to the posterior/lateral leg.
The area between the Achilles tendon and posterior border of the fibula is marked approximately 5 to 7 cm proximal to the lateral malleolus. An incision is made, and the lesser saphenous vein is identified. The vein is then retracted superficially to expose the sural nerve.
At this point, the surgeon may harvest the entire nerve, or fascicular portions depending on pathological requirements. Bevilacqua et al. recommend a biopsy of the entire nerve if the pathology may not involve all of the fascicles, and the patient's symptoms are severe. Likewise, if the patient's symptoms are minimal and the pathology may be localized in the fascicles, then a fascicular biopsy should be performed.[1]
For a complete nerve biopsy, untied sutures are placed into both ends of the nerve, and the nerve is transected above these sutures. The nerve is then removed using these sutures as a sling to avoid nerve compression. For a fascicular biopsy, the nerve is partially transected and sent using similar techniques. Care should be taken to avoid compression or curling of the nerve during harvesting and fixation. Individual laboratories vary on specimen fixation techniques required; therefore, guidance is necessary for local facilities.
During a fascicular biopsy, the surgeon can attempt a repair after harvest by carefully matching nerve patterns and performing an end-to-end repair of remaining structures under a microscope.[12] Many products, including collagen-based conduits and nerve-wraps, are available in an attempt to decrease morbidity and risks of neuroma formation after the procedure.[13]
Complications
One prospective study looked at 50 patients who underwent a sural nerve biopsy. Their findings were that the biopsy changed the diagnosis in 14% of cases, and altered management in 60% of cases.[14] Further, 33% of patients reported an increase in pain at six months; however, one study of 16 patients reported complete resolution in post-surgical pain following both fascicular and whole nerve biopsy.[14][15] This study also reported that the main complaining symptom five years after both whole and fascicular biopsy was tactile induced dysesthesias located to the sural nerve distributional area.[15]
Reduced sensation in the sural nerve distribution occurred in 18.4% of patients who underwent a whole nerve biopsy (n=717).[16] Sensation loss has been shown not to differ based on whether patients had a fascicular or whole nerve biopsy.[15]
Clinical Significance
With the proper pre-operative workup, management of patient expectations, and specimen analysis with highly experienced pathologists, a sural nerve biopsy offers valuable insight into a patient's cause of neuropathy. Although not without morbidity, the sural nerve biopsy is the gold standard in the diagnosis of certain conditions such as peripheral nerve vasculitis.[10]
Enhancing Healthcare Team Outcomes
In 2010, the Peripheral Nerve Society published guidelines on performing and evaluating the nerve biopsy. Their Class IV recommendations are as follows [17]:
- The biopsy should only be performed after exhaustion of lab testing, electrophysiological findings, and thorough clinical investigation
- All providers involved should have a good working relationship as well as the open sharing of information in regards to the patient.
- The specimens should be evaluated by those with training and expertise in the matter
- The laboratory performing the analysis should have the ability to interpret frozen and fixed sections
- Although not necessary, additional tests that may be useful are immunohistochemistry, electron microscopy, fiber analysis, and others.
Nursing, Allied Health, and Interprofessional Team Interventions
Proper labeling and handling of the surgical specimen are crucial for ensuring optimal patient outcomes. Proper specimen handling, identification, documentation, and transportation to the laboratory should be standardized, and OR staff should be trained in this process.[18]
Nursing, Allied Health, and Interprofessional Team Monitoring
Patients should be monitored in the immediate post-operative setting for acute complications such as hemodynamic instability, one of the main predictors of deterioration.[19] Guidelines and patient safety milestones reached prior to discharge vary by individual facility, and the nursing staff should be trained in these prior to the procedure.