Introduction
The corrugator (or corrugator supercilii) muscles are a pair of muscles located at the medial end of the eyebrow. They have recognition as significant muscles in the glabellar and central forehead regions. The corrugator supercilii muscles (CSM) play a major role in elevating the medial segment of the eyebrow, depressing the lateral portion of the eyebrow and are responsible for producing vertical frown lines.[1]
Structure and Function
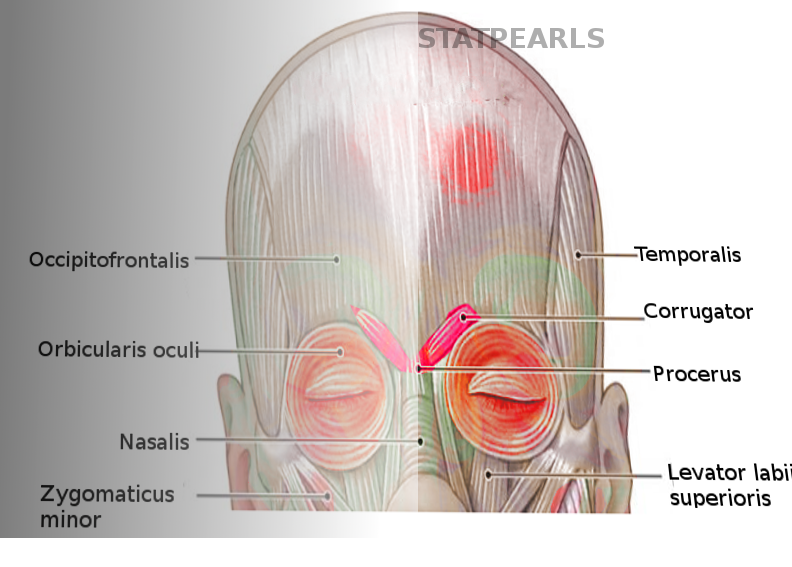
The corrugator supercilii muscles exist as a pair of small pyramidal muscles that lie deep to the frontal portion of the occipitofrontalis and the orbicularis oculi muscles. They arise from the medial supraorbital ridge of the frontal bone.[2] From the medial end of the eyebrow, the corrugator supercilii muscles travel laterally and above the orbital rim to become more superficial. They then insert into the dermis of the medial aspect of the eyebrow above the supraorbital margin.[1] The paired corrugator supercilii muscles have two heads: a transverse head and an oblique head. The transverse head arises from the superomedial part of the orbital rim that serves to pull the brows medially while the smaller oblique head runs parallel to the depressor supercilii and serves to depress the medial brow.[3] These actions lead to the vertical wrinkling of the supranasal skin of the forehead. Along with the glabellar muscles and procerus, the corrugator supercilii muscles also function as accessory protractors of the upper eyelid that aid to reduce glare under bright sunlight.[1] Additionally, the corrugator supercilii muscles serve as mimetic muscles that contract when one is angered or perplexed and form a major component of the superficial musculoaponeurotic system (SMAS) of the upper portion of the face.[1] A previous study demonstrated participants who categorized surprised facial expressions as negative exhibited greater corrugator supercilii muscle activity compared to those who viewed them as positive facial expressions. Therefore, corrugator supercilii muscles activity can help evaluate differences in positivity-negativity bias among different participants.[4]
Blood Supply and Lymphatics
The corrugator supercilii muscles receive blood supply from the supraorbital and supratrochlear arteries of the ophthalmic artery, which is a branch of the internal carotid artery.[5]
On the right side of the body, the common carotid arteries originate from the brachiocephalic trunk, and on the left side of the body, they come from the aortic arch. In the neck, at the upper margin of the thyroid cartilage, each common carotid artery runs within the carotid sheath and bifurcates into the internal and external carotid arteries.
In the temporal bone, the internal carotid artery enters the skull through the carotid canal and divides into the ophthalmic artery, which travels through the orbit through the optic canal. Inside the orbit, the ophthalmic artery divides into many branches, including the supraorbital artery, supratrochlear artery, lacrimal artery, central retinal artery, ethmoidal arteries, ciliary arteries, and inferior and superior muscular arteries. The supraorbital and supratrochlear arteries of the ophthalmic artery supply the corrugator supercilii muscles. The supratrochlear artery, which first traverses underneath the frontalis and corrugator supercilii muscles, gradually appears more superficial. The supratrochlear neuromuscular bundle passes through the corrugator supercilii muscles and provides sensation and vascularity to the forehead.[5]
Nerves
The corrugator supercilii muscles have a dual nerve supply from branches of the temporal, zygomatic, and buccal branches of the facial nerve. The motor nerve supply of the corrugator supercilii muscles originates from the frontal branch of the temporal division of the facial nerve while the zygomatic branch appears to innervate the oblique head. After receiving innervation from the zygomatic branch, the buccal branch forms the angular nerve to supply the corrugator supercilii muscles and procerus.[6]
The supratrochlear nerve (STN) and supraorbital nerve (SON), which are some terminal branches of the frontal nerve, are also closely associated with the corrugator supercilii muscles. After traveling over the orbit anteromedially, the supratrochlear nerve and supraorbital nerve pass through the corrugator supercilii muscles and enter the occipitofrontalis muscle to receive sensation from the mucosa of the glabella, skin of the lower forehead, and upper portion of the eyelid. The supratrochlear nerve also exits lateral to the origin of the corrugator supercilii muscles, enters the corrugator supercilii muscles where it splits into three or four small branches, and then penetrates the frontalis muscle.[7] In a study by Lee et al., among Asians, the supratrochlear nerve was found to emerge separately, coming from the supraorbital nerve at the medial aspect of the orbit, and either pass through the corrugator supercilii muscles as a single branch or bifurcate into two divisions before entering the corrugator supercilii muscles in 69% of cases. In the rest of the cases, the supratrochlear nerve was found to materialize from the orbit at the same location as the supratrochlear nerve and then pass through the corrugator supercilii muscles. The supratrochlear nerve was also found to always travel within the fibers of the corrugator supercilii muscles and not at a surface that is more superficial or deeper to the corrugator supercilii muscles. These results are different from those of a previous study that demonstrated the supratrochlear nerve penetrated the corrugator supercilii muscles in 84% of cases among people of the White race.[7][8] A complete understanding of the relationship between the supratrochlear nerve, supraorbital nerve, and the corrugator supercilii muscles and their anatomic locations allow for a more precise and tailored approach to corrugator supercilii muscle resection for forehead rejuvenation and surgical treatment of migraine headaches.
Muscles
The corrugator supercilii muscles consist of two heads. The transverse head arises from the superomedial margin of the orbital rim and inserts into the dermis at the middle third of the brow and interdigitates with the orbicularis oculi and frontalis muscles. The smaller oblique head runs parallel to the depressor supercilii after inserting into the medial brow.[3]
The corrugator supercilii muscles work with other muscles of the glabellar complex, including the procerus, depressor supercilii, and the orbicularis oculi muscles, to maintain a balanced brow position and shape.[1]
Physiologic Variants
The lateral margin of the corrugator supercilii muscles may differ among different individuals. In some cases, it may extend to the lateral third of the brow.
According to a review of the anatomy of the corrugator supercilii muscles, among the 30 articles included in the analysis, the corrugator supercilii muscles was found to arise mainly from the medial supraorbital rim and the medial frontal bone.[9] Forty-one percent of the articles mentioned the corrugator supercilii muscles traveled only through the frontalis muscle. The same number of articles also indicated the corrugator supercilii muscles could travel through the frontalis and orbicularis oculi while only 18% of the articles evaluated mentioned the corrugator supercilii muscles passed through the orbicularis oculi.[9] Fifty-nine percent of the articles mentioned the corrugator supercilii muscles course superolaterally, while 41% of the articles mentioned the corrugator supercilii muscles traverse laterally. The corrugator supercilii muscles mainly inserted to the middle of the eyebrow but could also insert to the glabella.[9] The temporal division of the facial nerve is the primary source of innervation to the corrugator supercilii muscles, but innervation could also come from the zygomatic division (17%) or the buccal and zygomatic branches (17%). In most cases, the corrugator supercilii muscles were found to pull the eyebrows downward and toward the midline of the face. However, they may also pull the medial portion of the eyebrow upward and depress the lateral part of the eyebrow. These anatomical variations require consideration during surgical procedures involving the corrugator supercilii muscles.[9]
Surgical Considerations
Complete comprehension of the anatomy of the corrugator supercilii muscles and its associated nerves and blood supply is essential for corrugator supercilii muscles resections during forehead rejuvenation and supraorbital nerve/supratrochlear nerve decompression in migraine headache treatment. With regards to forehead rejuvenation, cosmetic physicians may inject neurotoxins into the glabellar complex to maintain an aesthetically pleasing brow position and shape. Precise toxin injection is vital for retaining an aesthetically pleasing brow appearance. When treating the corrugator supercilii muscles near the origin, an injection with greater depth is necessary to grasp the depressor supercilii and the corrugator supercilii muscles fully. When treating the corrugator supercilii muscles more laterally, however, the injection should be more superficial because the corrugator supercilii muscles are at a more superficial surface. The glabellar complex needs 15 to 20 units of onabotulinum or incobotulinum or 38 to 50 units of abobotulinum at the procerus, which requires one location for injection, and the corrugator supercilii muscles, which require two locations for injection.[10]
Details regarding the physiological variations of the corrugator supercilii muscles also deserve consideration to reduce the risk of undesirable postoperative outcomes, such as forehead irregularities, asymmetries, and unequal muscle reactivation. Further, discrepancies in the location of the corrugator supercilii muscles and supratrochlear nerve among patients from different cultural groups require investigation as previous studies have demonstrated the positions of the corrugator supercilii muscles, and supratrochlear nerve between people of White race and Asians are different.[7][8] Therefore, it is inappropriate to apply the same surgical techniques to both patient groups.[7]
Clinical Significance
As a significant component of the glabellar complex, the corrugator supercilii muscles play an essential role in maintaining the position of the brow. Complete resection of the corrugator supercilii muscles has been a recommendation for forehead rejuvenation. Incomplete corrugator supercilii muscle resection can have harmful consequences, such as forehead asymmetries, skin dimpling, and recurrence of glabellar furrows and frown lines. One previous study suggested the amount of corrugator supercilii muscles resection can differ depending on the surgical technique used, with as much as one-third of the transverse corrugator supercilii muscles head remaining after the corrugator supercilii muscles are removed using transpalpebral methods. [3] Therefore, familiarity with the anatomy of the corrugator supercilii muscles with regards to fixed bony landmarks is essential for a more systematic approach to precise resection of the corrugator supercilii muscles.
Complete resection of the corrugator supercilii muscles has also been a recommended approach for the treatment of migraine headaches. There have been suggestions that migraine headaches are associated with peripheral nerve trigger points and the supraorbital nerve/supratrochlear nerve.[3] Chemodenervation of the corrugator supercilii muscles by botulinum toxin type A has been demonstrated to improve migraine headaches by decompressing the supraorbital nerve and the supratrochlear nerve and relaxing the nearby musculature. Patients who have complete corrugator supercilii muscles myectomy have also been shown to have long-term success.[3]
Patients with thyroid eye disease with upper eyelid retraction often have overactivity of the accessory muscles that play a role in eyelid closure and the glabellar muscles. They may have a staring facial expression with proptosis, upper lid retraction, and a glabellar frown. [1] The frown may have vertical glabellar furrowing and an altered eyebrow contour, with medial brow ptosis and a deep horizontal line over the nasal bridge. These facial lines mainly originate from a chronic contraction of the corrugator supercilii muscles and the procerus pulling on the skin. Botulinum A chemodenervation has been shown to flatten the glabellar region and enhance the medial eyebrow contour in patients with thyroid eye disease. [1]
Among patients with abnormal Parkinson disease, the “procerus sign” is a clinical sign that is often observed, particularly in patients with progressive supranuclear palsy (PSP). PSP may suffer misdiagnosis as the more well-known Parkinson disease. The procerus sign involves having vertical wrinkles on the forehead and a staring, astonished look with eyelid retraction and infrequent blinking. [11] It is often believed the procerus sign is secondary to dystonia of the procerus muscle. However, the term may be misleading as the corrugator supercilii muscles appear to be the main muscles to produce the frown or vertical creases. [11] Nevertheless, the generation of vertical creases on the forehead is a complex phenomenon, and the procerus sign should be prominent in early PSP.