Introduction
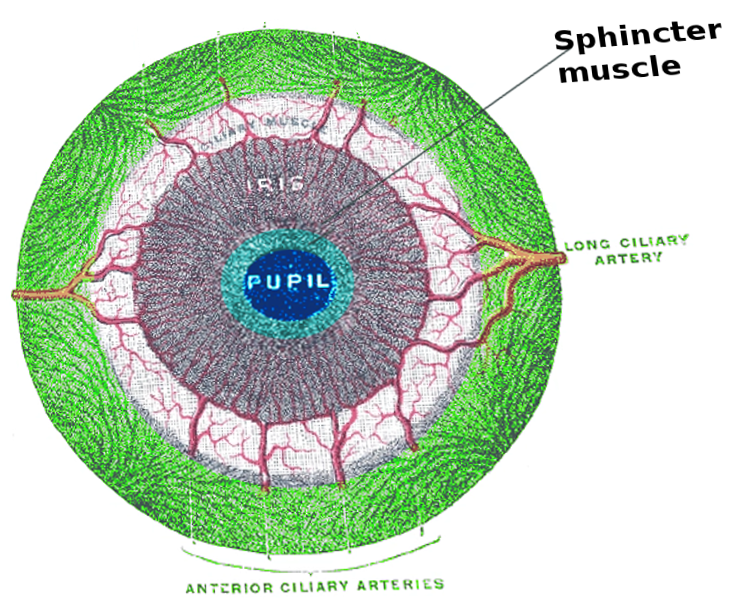
The iris sphincter muscle, also known as the pupillary sphincter or sphincter pupillae, is a muscle located in the colored part of the eye called the iris. The sphincter muscle fibers are located near the pupillary margin and are slightly anterior to the pigmented epithelium of the iris. It encircles the pupil of the iris and functions to constrict the pupil in bright light via the pupillary light reflex or during accommodation. By controlling the pupil's diameter, the iris controls the amount of light that reaches the back of the eye at the retina.
Structure and Function
The iris is a circular, pigmented diaphragm that lies anterior to the lens in a coronal plane. This diaphragmatic structure is attached peripherally to the ciliary body, with its unbound central border forming an aperture known as the pupil. The iris divides the space between the cornea and the lens into anterior and posterior chambers. The anterior chamber is bound by the cornea and iris. The anterior chamber communicates through the pupil with the posterior chamber, which is bound by the iris, ciliary processes, zonules, and lens. A fluid substance known as aqueous humor fills both chambers.
The iris, via the sphincter pupillae, is a part of the accommodative reflex. The accommodative reflex of the eye is an involuntary response when the visual focus switches from an object at a distance to one that is closer. The reflex is controlled by the parasympathetic nervous system and involves three actions - alteration of pupil aperture, lens shape, and convergence. The sphincter pupillae causes the narrowing of the pupil in order to prevent diverging light rays from the corneal periphery creating a blurred image.
Embryology
The vertebrate eye is made up of tissue from various embryonic origins. The lens and the cornea originate from the surface ectoderm. The retina and the epithelial layers of the iris and ciliary body originate from the anterior neural plate.[1] Within the stroma of the iris, the sphincter pupillae and dilator pupillae muscles develop from the optic cup neuroectoderm, along with the iris epithelium.
In contrast, the ciliary muscle, which is responsible for changing the shape of the lens, is derived from overlying mesenchyme. The optic cup is neuroectodermal in origin and gives rise to the neuronal retina, the retinal pigmented epithelium, the epithelial layers of the ciliary body and iris, and the iris musculature.[2]
Blood Supply and Lymphatics
Ocular blood flow is controlled both via direct autonomic influences on the vasculature of the optic nerve, choroid, ciliary body, and iris and by indirect influences on retinal blood flow.[3] The iris is supplied by the anterior ciliary arteries, the long posterior ciliary arteries, and anastomotic connections from the anterior choroid. Most of the venous drainage from the anterior segment of the eye drains into the choroid posteriorly and then into the vortex veins.
Nerves
The iris sphincter muscle receives parasympathetic innervation via the short ciliary nerves, leading to pupillary constriction (miosis) and accommodation.[3] The parasympathetic fibers that serve the sphincter muscle originate from the Edinger-Westphal nucleus of cranial nerve III. The signal synapses in the ciliary ganglia become terminated on muscarinic receptors of the muscle fibers.
Reciprocal function is primarily the responsibility of sympathetic innervation, which comes from the superior cervical ganglia. The sympathetic fibers help promote sphincter muscle relaxation, which is critical for periods of low-light or night vision. Sympathetic innervation from the superior cervical ganglion project to the dilator muscle of the iris via long ciliary nerves to control pupil dilation. The sympathetic and parasympathetic systems work in opposition to constantly adjusting the pupillary aperture.[3]
Muscles
There are two muscles of the iris, and they both consist of smooth muscle. The sphincter muscle contracts the pupil in a circular motion, while the dilator muscles enlarge the pupil by pulling the iris radially. The iris collarette is the thickest portion of the iris, where the sphincter and dilator muscles overlap. While the collarette is typically flat, this structure can be rather prominent in some cases.[4]
Physiologic Variants
Aniridia is characterized by iris hypoplasia and has been shown to be associated with mutations in the PAX6 gene.[5] Usually involving both eyes, it can be congenital or caused by a traumatic injury to the eye. Isolated aniridia is a condition that can be associated with low vision, macular or optic nerve hypoplasia, cataracts, and cornea changes. Aniridia also can be associated with WAGR syndrome or Gillespie syndrome. [6][7]
Surgical Considerations
Surgery to the iris sphincter is done for functional or cosmetic issues. Surgery is generally warranted if the patient has photophobia or blurry vision that cannot be controlled with drops. Patients can use pilocarpine drops to decrease the size of their pupils if some function of the sphincter remains. Reading glasses may also be necessary if the patient's eyes cannot accommodate. If inflammation occurs following trauma, the patient should be treated with steroid drops until the inflammation is resolved and re-assessed for sphincter function.
Clinical Significance
Adie syndrome, also known as Holmes-Adie syndrome, is a neuro-ophthalmological disorder distinguished by a lack of response to light and a pupil that is tonically dilated but is able to respond to accommodation (called Adie tonic pupil).[8] It is usually a benign entity. A variety of causes (usually infectious) lead to Adie tonic pupil and result from damage to postganglionic fibers of the parasympathetic innervation to the eye, which results in an inability to constrict the iris sphincter muscle. It is more common in women and manifests unilaterally in 80% of cases.[9] Adie tonic pupil has been reported in the literature to be associated with a number of related syndromes, including Adie syndrome, which involves diminished deep tendon reflexes.
Iridoplegia is the paralysis of the sphincter muscle of the iris. It often results from direct trauma to the orbit but can also result from inflammation or even from eyedrops. There are three types of iridoplegia:
- Accommodative iridoplegia: The inability of the pupil to constrict during accommodation
- Complete iridoplegia: Will not constrict regardless of stimulation
- Reflex iridoplegia: Also known as Argyll Robertson pupil, will not constrict to light but retains the ability for accommodation reflex
It is important to differentiate the ptosis in Horner syndrome from damage to the oculomotor nerve. In Horner syndrome, the ptosis occurs with a constricted pupil due to loss of sympathetic innervation to the eye (inability to dilate leads to constriction). This is compared to damage to the oculomotor nerve, where the ptosis is accompanied by a dilated pupil (due to damage to the parasympathetics and inability to constrict via the sphincter pupillae).
Other Issues
An iris coloboma is a hole in the iris usually due to incomplete closure of the fetal fissure during organogenesis. Colobomas can range from a simple hole in the iris to more severe involvement of the posterior pole, coloboma of the optic nerve of the choroid of the retina.[10] Colobomas also have a clinical association with CHARGE syndrome, a rare heritable disease caused by a mutation in the CHD7 gene that regulates chromatin remodeling.[11][12]
Traumatic mydriasis is usually the result of blunt injury to the eye and can present with iris sphincter tears that alter the shape of the pupil in the affected eye. Treatment initially involves cycloplegia to prevent posterior synechiae in patients with iritis. Patients are then observed clinically for the return of function. Surgical intervention can be considered if the function does not return and the patients are symptomatic. Ocular trauma can also cause pupillary miosis though this is less common than mydriasis and tends to be related to anterior chamber inflammation.