Continuing Education Activity
Adenomyomatosis is a benign condition that can present with right upper quadrant pain and is characterized by hyperplasia of the gallbladder wall mucosa and muscularis propria, with pathognomonic epithelial invaginations forming cystic pockets (Rokitansky-Aschoff sinuses). Although this condition is benign, it can be difficult to distinguish from gallbladder cancer based on the diagnostic imaging findings, in which case it may be treated with cholecystectomy. This activity reviews the evaluation and management of adenomyomatosis and highlights the interprofessional team's role in caring for patients with this condition.
Objectives:
- Describe the epidemiology of adenomyomatosis.
- Explain how to diagnose adenomyomatosis.
- Identify the differential diagnosis for adenomyomatosis.
- Review the roles of various interprofessional teams in coordinating care to improve outcomes for patients with adenomyomatosis.
Introduction
Adenomyomatosis, also known as adenomyoma or adenomyomatous hyperplasia of the gallbladder, is one of the two hyperplastic cholecystoses. The other hyperplastic cholecystosis is cholesterolosis, also known as "strawberry gallbladder." Adenomyomatosis is a benign condition that is pathologically characterized by hyperplasia of the gallbladder wall mucosa and muscularis propria, with pathognomonic epithelial invaginations forming cystic pockets (Rokitansky-Aschoff sinuses). These sinuses may contain calculi or cholesterol crystals. The gallbladder wall thickening, Rokitansky-Aschoff sinuses, and the calculi or cholesterol crystals that are often found in sinuses characterize the imaging appearance of adenomyomatosis.
Sometimes, mainly when the characteristic imaging findings are not present, adenomyomatosis can be challenging to distinguish from gallbladder cancer based on the diagnostic imaging findings. Adenomyomatosis is often asymptomatic and incidentally detected, requiring no specific treatment. Adenomyomatosis also can be associated with right upper quadrant pain. In cases where it is challenging to distinguish adenomyomatosis from gallbladder cancer or when adenomyomatosis is associated with right upper quadrant pain, this condition may be treated with cholecystectomy.[1][2]
Etiology
The cause of adenomyomatosis is unknown, although some have proposed that it is a response to chronic inflammation of the gallbladder. Since patients are most frequently diagnosed in their 50s, the idea of chronic inflammation as the etiology seems plausible.[3][4] Adenomyomatosis of the gallbladder was initially recognized as a precancerous lesion; recent studies currently consider it a benign alteration of the gallbladder that is often associated with cholecystitis and cholecystolithiasis. Gallbladder carcinoma is an extremely malignant disease with a 5-year survival rate of less than 5 percent.[4]
Epidemiology
Adenomyomatosis has been found in 1 to 8.7 percent of cholecystectomy specimens. Although there is a wide age range of patients diagnosed with adenomyomatosis, patients are most frequently diagnosed in their 50s. There are discrepancies in the literature regarding the prevalence of adenomyomatosis in males and females. It is well known that adenomyomatosis is more prevalent in women than in men (3 to 1). Other authors declare that the prevalence is similar in men and women. There is no known race predilection.[5]
Pathophysiology
Hyperplasia of the wall of the gallbladder is seen with characteristic Rokitansky-Aschoff sinuses. Another finding is the presence of calculi and cholesterol crystals form within the sinuses. The cause of hyperplasia and sinus formation is unknown, although reactive changes to chronic inflammation have been proposed. The hypothesis of chronic inflammation as the underlying cause of adenomyomatosis is supported by the fact that patients are most frequently diagnosed in their 50s.
Histopathology
Several Rokitansky-Aschoff sinuses are seen on histopathologic examination of an adenomyomatosis specimen. Thickening of the subserosa is seen. Nerve trunks are often seen in the subserosa. There is often smooth muscle hypertrophy in the gallbladder wall. The surface epithelium has a variable appearance, sometimes showing reactive epithelial changes, having a papillary appearance, or showing metaplasia. More rarely, there is a perineural and intraneural invasion into the subserosa.
History and Physical
Most patients with adenomyomatosis of the gallbladder are thought to be asymptomatic. Right upper quadrant pain has been seen in association with adenomyomatosis. Some patients have coexistent cholelithiasis, which can be symptomatic.
Evaluation
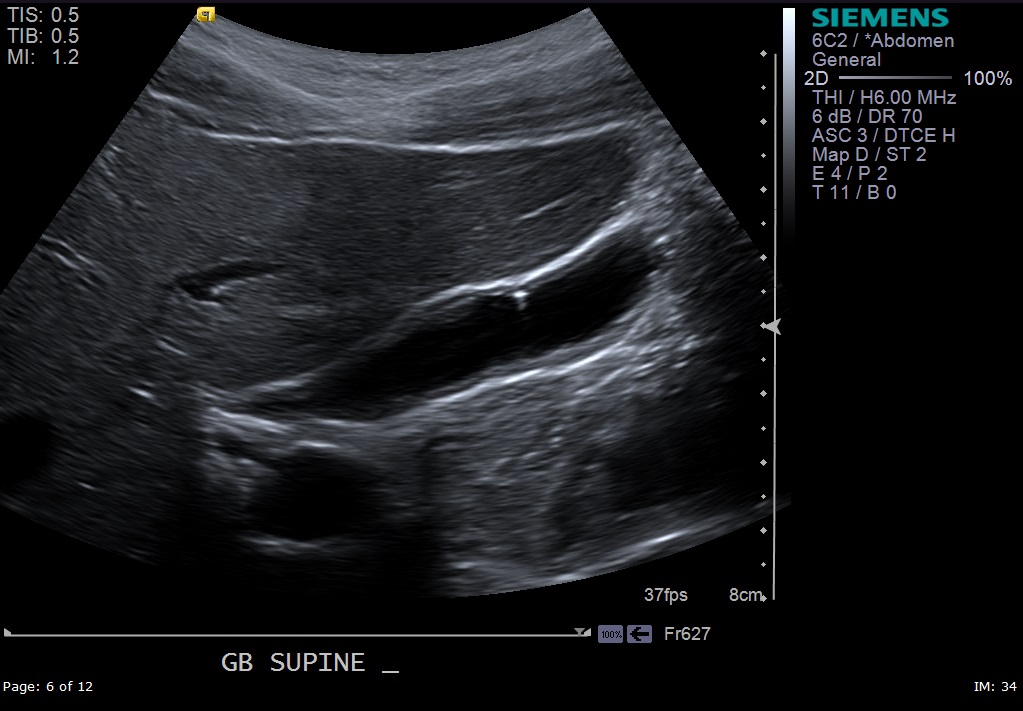
During the evaluation of patients presenting with right upper quadrant abdominal pain, ultrasound should be the primary modality to assess such patients initially. The ultrasound findings could be characteristic of adenomyomatosis, and it could be of great benefit to help providers reach a diagnosis. Sometimes, gallbladder wall thickening is seen on ultrasound but cannot be well characterized. In such a case, further characterization could be achieved via magnetic resonance imaging (MRI) of the abdomen. Gallbladder wall thickening could be an incidental finding on computed tomography (CT) scan; an ultrasound or an MRI scan may be useful for further characterization. The characteristic findings of adenomyomatosis are gallbladder wall thickening, Rokitansky-Aschoff sinuses, and the calculi or cholesterol crystals often found in sinuses. On ultrasound scanning, adenomyomatosis is seen as gallbladder wall thickening, intramural cystic spaces, and echogenic intramural foci (cholesterol crystals in the Rokitansky-Aschoff sinuses) that show comet tail artifacts. In most cases, all of the characteristic findings are not present.[6][7][8]
Of the ultrasound findings described, the echogenic foci with associated V-shaped comet tail artifacts have been described as specific for adenomyomatosis. On MRI, adenomyomatosis shows gallbladder wall thickening and T2 hyperintense intramural cystic spaces. Calculi are seen as signal voids. The T2 hyperintense cystic areas can align in a curvilinear fashion, producing a “pearl necklace sign.” On CT imaging, nonspecific gallbladder wall thickening and wall enhancement are sometimes seen. The “rosary sign” can be present, which is caused by a thin layer of enhancing epithelium lining the intramural diverticula, which is surrounded by hypo-enhancing hypertrophied muscularis, causing the gallbladder wall to resemble a rosary.
Treatment / Management
In cases where it is difficult to distinguish adenomyomatosis from gallbladder cancer or adenomyomatosis is associated with right upper quadrant pain, adenomyomatosis may be treated with cholecystectomy. If adenomyomatosis is found incidentally and is asymptomatic, no treatment is recommended.[9][10]
Differential Diagnosis
The differential diagnosis for adenomyomatosis of the gallbladder includes gallbladder malignancies (e.g., adenocarcinoma, cholangiocarcinoma, metastatic disease), gallbladder polyps, and benign gallbladder tumors (e.g., adenoma). Normal variant appearances of the gallbladder, such as gallbladder folds (“Phrygian cap”), are also within the differential diagnosis.
Prognosis
Apart from the right upper quadrant abdominal pain that some patients experience, this is a benign condition and carries a good prognosis. Not all patients are symptomatic. Adenomyomatosis is often asymptomatic and detected incidentally. It is important to note that gallbladder malignancy can have a similar appearance to adenomyomatosis on imaging, and gallbladder carcinoma has a much worse prognosis than adenomyomatosis. Therefore, it is vital to ensure that the imaging diagnosis of adenomyomatosis is confident before dismissing this abnormality.
Complications
Adenomyomatosis has not been definitively linked to cancer but can have inflammatory complications.
Consultations
- Radiologists
- Radiology technologist
- Registered diagnostic medical sonographers
- Gastroenterologists
- Internal medicine providers
- General surgeon
- Nurse practitioners
Deterrence and Patient Education
Patient education is key to the successful management of patients presenting with right upper quadrant abdominal pain. The nurse plays a crucial role in collaboration with providers in educating patients about the signs and symptoms of adenomyomatosis of the gall bladder. The nurse should encourage patients to report any deterioration of their symptoms to their providers instantly. Written information leaflets should be provided to patients with adenomyomatosis of the gallbladder.
Pearls and Other Issues
Adenomyomatosis of the gallbladder is frequently asymptomatic and detected incidentally. However, adenomyomatosis can also be a cause of right upper quadrant pain. Adenomyomatosis is characterized by gallbladder wall thickening and the formation of Rokitansky-Aschoff sinuses, which can collect internal cholesterol crystals and stones. The appearance of adenomyomatosis on diagnostic imaging is closely related to these histopathological changes (gallbladder wall thickening/intramural cystic spaces/cholesterol crystals). On ultrasound, the presence of echogenic foci with V-shaped comet tail artifacts in the gallbladder wall is thought to be specific for adenomyomatosis. Adenomyomatosis is frequently asymptomatic and, in those cases, requires no treatment. However, adenomyomatosis can sometimes be difficult to distinguish from gallbladder cancer. Therefore, in cases where it is right upper quadrant abdominal pain or where a gallbladder abnormality/gallbladder wall thickening cannot be confidently described as adenomyomatosis rather than gallbladder malignancy, cholecystectomy may be indicated.
Enhancing Healthcare Team Outcomes
Adenomyomatosis of the gallbladder is a rare presentation but can be mistaken for several other gastrointestinal tract disorders. Because the condition is benign, it is important for the primary care provider or nurse practitioner to consult with a gastroenterologist or general surgeon to deliver the best standard of care for such patients. Most cases do not require any treatment. However, if the RUQ (right upper quadrant) pain persists, the onus is on the healthcare provider to rule out a malignancy.
The nurse plays a very crucial role in assisting the provider during the diagnosis and management of cases with adenomyomatosis of the gallbladder. The nurse should ensure that the patients could understand the underlying pathology and their diagnosis and its implications. The nurse should help the patients and their families throughout the process of decision-making. The nurse should ensure that patients are provided with the necessary written information leaflets about their condition. The nurse should liaise with the various healthcare team members involved in patient care with adenomyomatosis of the gallbladder. The nurse should ensure that patients are well-informed about their care plans at all times. The nurse should alert the provider if any untoward changes in the course of the patient's illness. To achieve the best standard of care for patients with adenomyomatosis of the gallbladder, effective communication and collaboration among the interprofessional team are mandatory. [Level 5]