Continuing Education Activity
Peripheral nerve injury can vary wildly in severity and presentation, ranging from mild soreness to severe muscle weakness. Axillary nerve injuries typically respond well to conservative management, though a surgical intervention may be required. Failure to accurately diagnose and manage patients may lead to life-long disability that can affect the overall quality of life. While axillary nerve lesions are somewhat rare, they must be considered in patients presenting with shoulder weakness and sensory loss. This activity reviews the evaluation and management of patients with axillary nerve injuries and highlights the role of the interprofessional team in caring for affected patients.
Objectives:
- Identify the typical presentation of a patient with an axillary nerve injury.
- Describe the proper evaluation of a patient with a suspected axillary nerve injury.
- Summarize the treatment options available for patients with axillary nerve injuries.
- Explain the importance of improving care coordination amongst the interprofessional team to enhance the delivery of care for patients with axillary nerve injuries.
Introduction
Peripheral nerve injury can vary wildly in severity and presentation, ranging from mild soreness to severe muscle weakness. Axillary nerve injuries typically respond well to conservative management, though a surgical intervention may be required. Failure to accurately diagnose and manage patients may lead to life-long disability that can affect the overall quality of life. While axillary nerve lesions are somewhat rare, they should be considered when patients present with shoulder weakness and sensory loss.
Anatomic Course
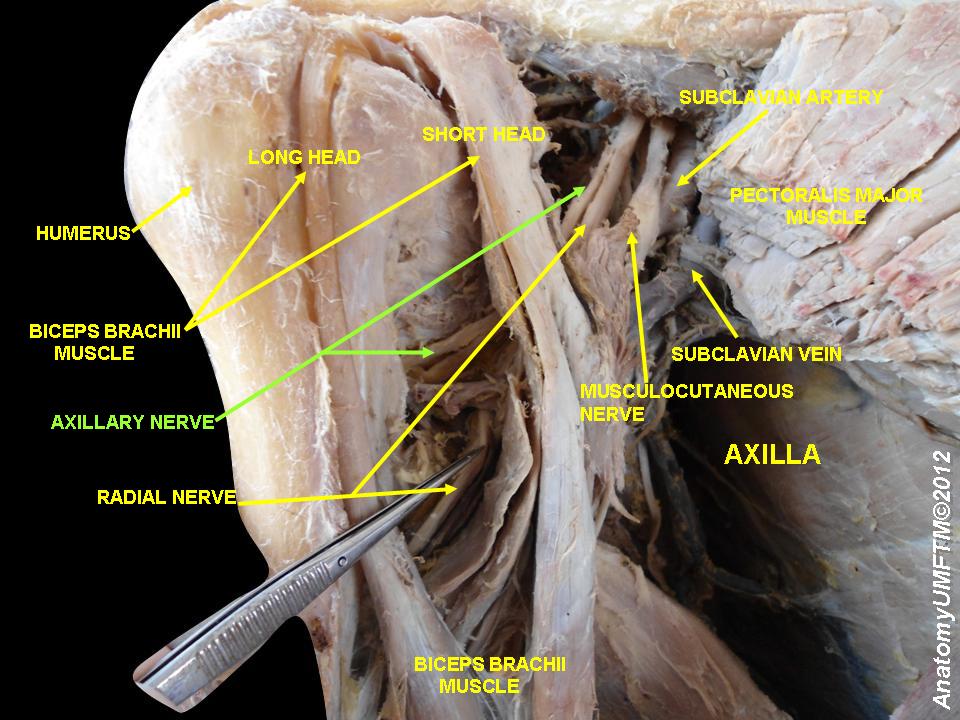
The axillary nerve diverges from the posterior cord of the brachial plexus anterior to the subscapularis muscle, running posterior to the axillary artery. It then travels inferior to the glenohumeral joint capsule and passes through the quadrangular space with the posterior humeral circumflex artery. The axillary nerve proceeds to split into anterior and posterior divisions. The anterior division supplies motor innervation to the anterior and middle heads of the deltoid. The posterior division provides motor innervation to the posterior deltoid and teres minor before eventually terminating as the superior lateral cutaneous nerve and innervating the lateral shoulder.[1] The axillary nerve is a bilateral upper extremity peripheral nerve and receives significant contributions from C5 and minor contributions from C6.[2]
Functional Anatomy
As stated above, the axillary nerve innervates the deltoid and teres minor muscles. The deltoid muscle, divided into three parts, performs and assists in a variety of actions. The primary function of the deltoid muscle is glenohumeral abduction, performed by the middle muscle belly. The anterior muscle belly assists in glenohumeral flexion and internal rotation. The posterior muscle belly assists in glenohumeral extension and external rotation.[3] The teres minor functions in glenohumeral external rotation.[4] The deltoid and teres minor stabilize the glenohumeral joint, with the teres minor contributing a greater role as a part of the glenohumeral rotator cuff.[5] Lastly, the axillary nerve transmits afferent sensory input from the lateral shoulder.[1] Several studies have claimed the axillary nerve innervates the long head of the triceps brachii. Still, a recent cadaver study by Wade et al. showed no axillary nerve innervation to the triceps brachii.[6]
Etiology
Axillary nerve injury typically presents with other brachial plexopathies. Axillary neuropathies are due to traumatic injuries, traction injuries, quadrilateral space syndrome, and brachial neuritis (also called neuralgic amyotrophy or Parsonage-Turner syndrome).[3]
An anterior dislocation and forced abduction of the shoulder joint appear to be common causes of axillary nerve injury in young people.
Epidemiology
An axillary nerve mononeuropathy is a rare event, occurring in about 0.3 to 6% of all brachial plexus injuries.[2] Axillary nerve injuries constitute 6% to 10% of all brachial plexus injuries during shoulder surgery.[7] Recent research showed that the risk of axillary nerve injury after glenohumeral dislocation increased with age. Approximately 65% of patients over 40 were diagnosed by electromyography (EMG) with an axillary nerve lesion.[8] Brachial neuritis has an estimated incidence of 1 to 3 per 100,000 annually with a female predilection.[9]
Pathophysiology
The axillary nerve injury may occur due to over-stretching of the axillary nerve during anterior should dislocation. The axillary nerve is most susceptible to injury at the origin from the posterior cord, in the quadrilateral space, the anteroinferior aspect of the shoulder capsule, and within the subfascial surface of the deltoid muscle.
History and Physical
The principle presenting symptoms are a weakness in glenohumeral abduction with or without numbness to the lateral shoulder area. Patients may also present with weakness in glenohumeral external rotation; however, this may not be apparent due to the ability of the infraspinatus. In patients presenting after dislocation or fracture, signs of trauma will be evident on physical exam. During external rotation and abduction, one may note the weakness of the deltoid and teres minor muscles.
Nevertheless, patients may not report muscle weakness or paresthesia due to acute pain and limited range of motion.[2] A compressive neuropathy may occur after blunt trauma to the deltoid muscle. Atraumatic neuropathy preceded by localized pain presents in brachial neuritis.[2][10] Patients with quadrilateral space syndrome (QSS) present with vascular symptoms such as cyanosis and pallor of the distal upper extremity and splinter hemorrhages in addition to neurologic symptoms.[11]
Evaluation
A proper history is essential in determining the correct intervention necessary. At the very least, the provider should obtain information on symptom onset, palliative and provoking factors, quality of the symptoms, radiation of symptoms to other regions, the severity of pain (if applicable), and timing. Key questions to consider are trauma, focal weakness, numbness and tingling, cyanosis, limitations in the range of motion, and pain.
The physical exam should begin with a visual inspection of the upper extremity, noting the presence or absence of trauma. The provider should palpate the ipsilateral neck and upper extremity for tenderness and muscle tone, followed by evaluating passive and active ranges of motion. Next, a neurologic exam focused on the axillary nerve and shoulder should also include assessing the spinal accessory, suprascapular, long thoracic, musculocutaneous, and radial nerves.[2] Several specialty clinical tests that evaluate the deltoid and teres minor muscles exist that may guide providers during assessment for axillary nerve injury in the absence of trauma, muscle strain, or known tendinopathies. The swallow-tail, deltoid extension lag, and Bertelli tests have been used to examine deltoid muscle weakness.[12][13] The external rotation lag, drop arm, and Patte tests evaluate the function of the teres minor muscle.[14]
Radiographs of the shoulder can help identify fractures involving the shoulder region after traumatic events. Shoulder magnetic resonance imaging (MRI) should be ordered if compressive neuropathy or inflammatory processes are suspected or in cases of chronic neuropathy that has resulted in muscle atrophy. The gold standard for diagnosis confirmation is EMG. Additionally, EMG findings can help establish a patient's baseline to evaluate recovery.[2]
Treatment / Management
Most axillary nerve injuries are treatable conservatively; however, select cases should require surgical management. For atraumatic injuries, a baseline EMG should occur within 1 month, and treatment with physical therapy (PT) should begin. In traumatic shoulder injury involving the axillary nerve, most patients may recover with non-operative treatment; however, there is the possibility of permanent paralysis. In many cases, then the shoulder is reduced, the need for surgical intervention is minimal. The reduced shoulder is immobilized for 4-6 weeks (young patients) or 7-10 days (elderly). This is then followed by extensive rehabilitation to regain muscle strength and shoulder mobility.
Surgical intervention can be considered in closed trauma if EMG shows no improvement after 3 months; however, acute nerve lesions warrant expedited surgical management. Neurorrhaphy, neurolysis, and nerve grafting are all possible surgical options. In patients with chronic muscle atrophy, muscle transfer may be a therapeutic option.[2]
For patients with neuropraxia, full recovery occurs over 6-12 months. The muscle weakness spontaneously recovers without any specific treatment.
For those with axonotmesis, the recovery rates are about 70% to 80% and often take many months. The patient should be followed with serial electromyogram (EMG) studies to assess for regeneration. If by 6-9 months, there are no signs of recovery, surgical exploration may be considered.
For those with neurotmesis, there is never any recovery without surgical intervention.
Differential Diagnosis
The following should be potential differentials when considering an axillary nerve lesion:[2][15]
- Cervical radiculopathy
- Thoracic outlet syndrome
- Rotator cuff tear
- Brachial plexopathy
- Quadrilateral space syndrome
- Brachial neuritis
- Glenohumeral fracture/dislocation
- Subacromial impingement syndrome
- Herpes zoster
Prognosis
Most injuries to the axillary nerve are considered low-grade following glenohumeral dislocation and will often result in complete recovery within 7 months.[8] A systematic review showed 85% of nerve graft patients and 79% of nerve transfer patients reached muscle strength grades 4/5 or greater at 18 to 24 months post-op.[16]
Complications
Chronic axillary nerve lesions result in permanent numbness to the lateral shoulder region, atrophy of the deltoid and teres minor muscles, and possibly chronic neuropathic pain.
Postoperative and Rehabilitation Care
Rehabilitation Care:
Frizziero et al. developed a rehabilitation protocol for axillary nerve injury which divides into two phases over two months. The initial phase focused on the restoration of scapular kinesis, glenohumeral stabilization, and strengthening of the deltoid muscle. The second phase focused on a return to function with particular attention to motor, postural, and proprioceptive control.[17]
Deterrence and Patient Education
Patient Education:[8][18]
- The axillary nerve is the most common damaged nerve in glenohumeral dislocation
- Low-grade axillary nerve injuries should resolve within 12 weeks
- High-grade axillary nerve injuries require surgical intervention
- Athletes in contact sports are at an increased risk of axillary nerve injury by traumatic processes that result in compression and lesion
Enhancing Healthcare Team Outcomes
Injury to the axillary nerve is a serious and common complication of glenohumeral dislocation. Complex dislocations (those associated with secondary injury to other bones, nerves, vessels, or tendons) should be identified as soon as possible by the primary care provider and nurse practitioner to minimize long-term deficits. Studies have shown an increased risk of axillary nerve injuries if dislocations have not been reduced within 12 hours. If prolonged axillary nerve deficits persist, surgical intervention is required, with better results seen with early intervention.[8] Iatrogenic axillary nerve injury is also commonly reported during surgical osteosynthesis, especially when utilizing the anterolateral approach.[19] Koshy et al. found no significant differences in post-op muscle strength recovery to 4/5 between patients undergoing surgical nerve transfers versus nerve grafting.[16]
Management of axillary nerve injuries is best with an interprofessional team, including physicians/mid-level practitioners, nursing, and physical therapists. In cases where medication is part of the regimen, pharmacists as well.