Introduction
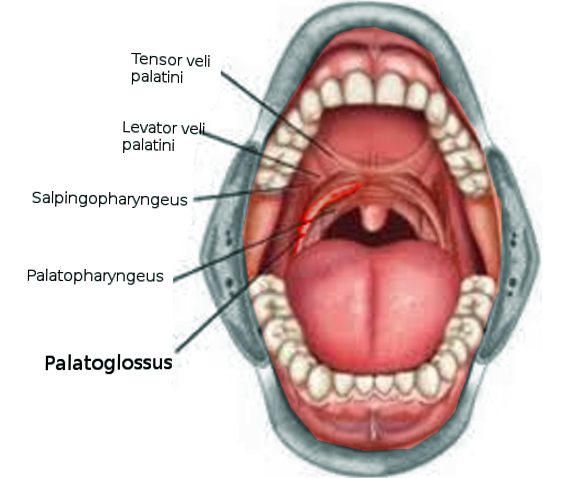
The palatoglossus muscle, also known as musculus palatoglossus, is among the four extrinsic muscles of the tongue and the paired muscles of the soft palate. The right and left palatoglossus muscles create ridges in the lateral pharyngeal wall, referred to as the palatoglossal arches (anterior faucial pillars). These pillars separate the oral cavity and the oropharynx — the muscle functions as an antagonist to the levator veli palatini muscle.
Structure and Function
The palatoglossus muscle functions to elevate the posterior portion of the tongue. It also draws the soft palate inferiorly, thereby narrowing the diameter of the oropharyngeal isthmus. This action plays a significant role during swallowing by propelling the food bolus towards the esophagus and occluding the oral cavity, thereby preventing retrograde flow of the food.[1] Also, it prevents the spillage of saliva from the vestibular region into the oropharyngeal region by maintaining the palatoglossal arch.
It has also been shown to be active in some individuals during speech.[1] According to some authors, during the pronunciation of vowels such as “u,” constriction of a larger area of the oropharyngeal isthmus is necessary. This is significantly affected by the activity of the palatoglossus muscle. The pronunciation of uvular fricatives requires constriction of a smaller area (incomplete closure) of the isthmus. This requires the palatoglossus muscle to pull in a downward and forward direction along with the activity of the palatopharyngeus muscle in a downward and backward direction. The combined activity of both muscles provides a sling effect.[2]
Embryology
Palatoglossus is the only tongue muscle derived from the fourth branchial arch. All the other muscles of the tongue derive from the occipital myotomes. This is the reason that all the other tongue muscles receive innervation from the twelfth cranial nerve (hypoglossal nerve) except the palatoglossus muscle, which is innervated by the tenth cranial nerve (vagus nerve).
Blood Supply and Lymphatics
The arterial supply is from the lingual artery, which is the branch of the external carotid artery. Some collateral circulation also comes from the branch of the facial artery (tonsillar artery). The lymphatic drainage is into the deep cervical group of lymph nodes.
Nerves
The palatoglossus muscle receives innervation from the pharyngeal branch of the cranial nerve X (vagus nerve).[3]
Muscles
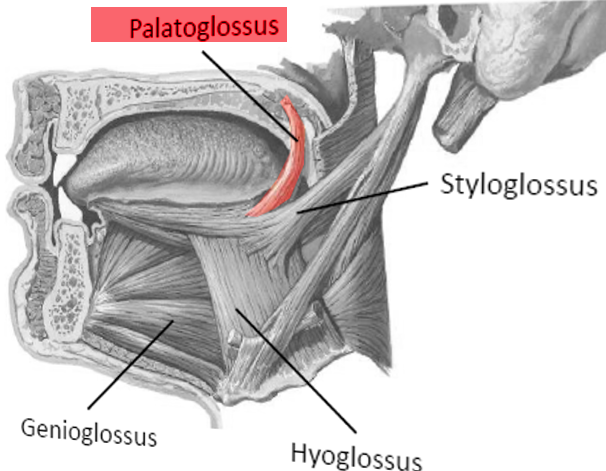
The muscle has its origin from the inferior surface of the palatine aponeurosis. It descends along with the muscle of the contralateral side in an inferior, forward, and lateral direction anterior to the palatine tonsil and gets inserted into the posterolateral surface of the tongue. Some fibers of the muscle spread over the dorsal surface of the tongue while the other fibers pass deep into the substance of the tongue and intermingle with one of the intrinsic muscles of the tongue (transverses linguae).
In comparison to the other palatal muscles, the palatoglossus muscle is relatively small. The muscle separates the superior part of the tonsil from the “supratonsillar fat.”[4] The muscle forms the anterior boundary of the tonsillar pillar.
Physiologic Variants
Variation in the region of attachment of the palatoglossus muscle in the soft palate has been observed. In some individuals, this region is near the uvula. In such cases, the mechanical ability of the palatoglossus muscle in elevating the tongue may be limited due to the lack of a rigid anchoring point towards which the tongue elevates. However, this attachment is favorable to lower the soft palate. This action is based on a class II lever system where the load (the bulk of soft palate) is present between the fulcrum (the posterior rim of the hard palate) and the force applied (action of the palatoglossus muscle). In some individuals, the attachment area of the muscle is relatively large into the anterior portion of the velum. In such instances, a considerable increase in the ability of the muscle to elevate the tongue exists. However, this attachment is not favorable to lower the soft palate. This action is based on a class III lever system where the force applied lies between the load and the fulcrum. The primary mechanism in these individuals to approximate the tongue and soft palate during swallowing is tongue elevation rather than lowering of the soft palate.[1]
Surgical Considerations
In patients with obstructive sleep apnoea, the lateral pharyngeal wall has been shown to collapse during the airflow as compared to patients without apnea. This collapse may exist because, during the expiratory-inspiratory transition, there may be a delay in the relaxation of the constrictor muscles. The lateral pharyngoplasty is a technique developed to act on these pathophysiological aspects of apnea. By myotomy of the superior constrictor muscles and suturing of the lateral pedicle flaps to the palatoglossus muscle, the lateral pharyngeal wall is reconstructed.[5]
During the surgical procedure of zeta-pharyngoplasty, anterior mucosa gets removed, and splitting of the soft palate is done in the midline. For this, the palatoglossus muscle is cut and then the posterior palatal mucosa is sewed to the anteriorly resected margin.[6]
Role in Glossectomy: During a surgical procedure for resecting tongue tumor, the area of resection is governed by the extent of tumor spread. The procedure of glossectomy can be divided into various categories based on the area of resection. Type IIIb glossectomy, also known as compartmental hemiglossectomy, includes the mucosa, submucosa, intrinsic muscles (transversalis, verticalis, inferior longitudinalis, and superior longitudinalis) and extrinsic muscles (genioglossus, hyoglossus, styloglossus and the inferior portion of the palatoglossus muscle) on the ipsilateral side of the lesion.[7]
Clinical Significance
The palatoglossus muscle along with the palatopharyngeus muscle functions to elevate the velar region and this in conjunction with the function of the levator veli palatini muscle provides velar positioning.[8]
Role in obstructive sleep apnoea: Studies have shown that if the nerve to the palatoglossus muscle is electrically stimulated, retropalatal space can be dilated which in turn aids in reducing the burden of obstructive sleep apnoea. The mechanism behind this function is that when the nerve is stimulated, it causes forward movement of the tongue base which may result in the advancement of the palate by anteriorly displacing the anterior palatal pillar. Simultaneously, the palatoglossus muscle also moves the soft palate in the anterior direction and help in increasing the retropalatal space.[9]
Role in tonsillar cancer: Tonsillar cancer, which in the majority of cases has its origin from the anterior tonsillar pillar, has a tendency to spread locally anteroinferior to the tongue, superomedial to the soft palate, or nasopharynx region. Through the anterior tonsillar pillar and the palatoglossus muscle, the tumor can involve the palatal region (hard and soft palate) or the base of the tongue. If the tumor involves the palate, it may affect the tensor palatine, levator palatine, and the pterygoid musculature.
Role in tongue base cancer: Tumor of the base of the tongue, particularly involving the posterior third, may spread along the palatoglossal muscle and involve the anterior tonsillar pillar.[10] It may extend to the soft palate through the palatoglossus muscle and then further to the nasopharyngeal region via the veli palatini muscles.
Role in cleft lip and palate: In cleft patients, to close the cleft involving the soft palate, both continuity and function of the soft palate require attaining an adequate length of the soft palate; this requires the reconstitution of the levator veli palatini, the palatopharyngeus, and the palatoglossus muscles.
Other Issues
The peritonsillar abscess usually occurs superior to the tonsillar region, where the base of the uvula and the anterior tonsillar pillar intersects, deep to the palatoglossus muscle.