Introduction
The infraspinatus is a thick triangular muscle that occupies much of the infraspinous fossa of the scapula. It is a member of the rotator cuff, commonly remembered by the mnemonic “SITS” (supraspinatus, infraspinatus, teres minor, subscapularis). These muscles contribute to help form the glenohumeral joint, which aids in shoulder joint motion and stability. These muscles allow the shoulder joint to have stability while being one of the most mobile joints in the body. The main functions of the infraspinatus are assisting in external rotation of the shoulder joint, scaption, and lateral rotation of the humerus.[1][2][3][4]
Structure and Function
The infraspinatus is a portion of the rotator cuff muscles composed of the supraspinatus, infraspinatus, teres minor, and subscapularis. These muscles act to stabilize the glenohumeral joint. The tendons of these muscles are nonlinear, viscoelastic, and heterogeneous. A major component of these tendons is collagen, which creates a matrix providing extensibility. The transition point of a tendon to bone insertion can be broken down into the following four zones: tendon mid-substance, fibrocartilage, calcified fibrocartilage, and bone.[5] In addition to the rotator cuff muscles, the glenohumeral joint is further stabilized by ligaments and connective tissues.
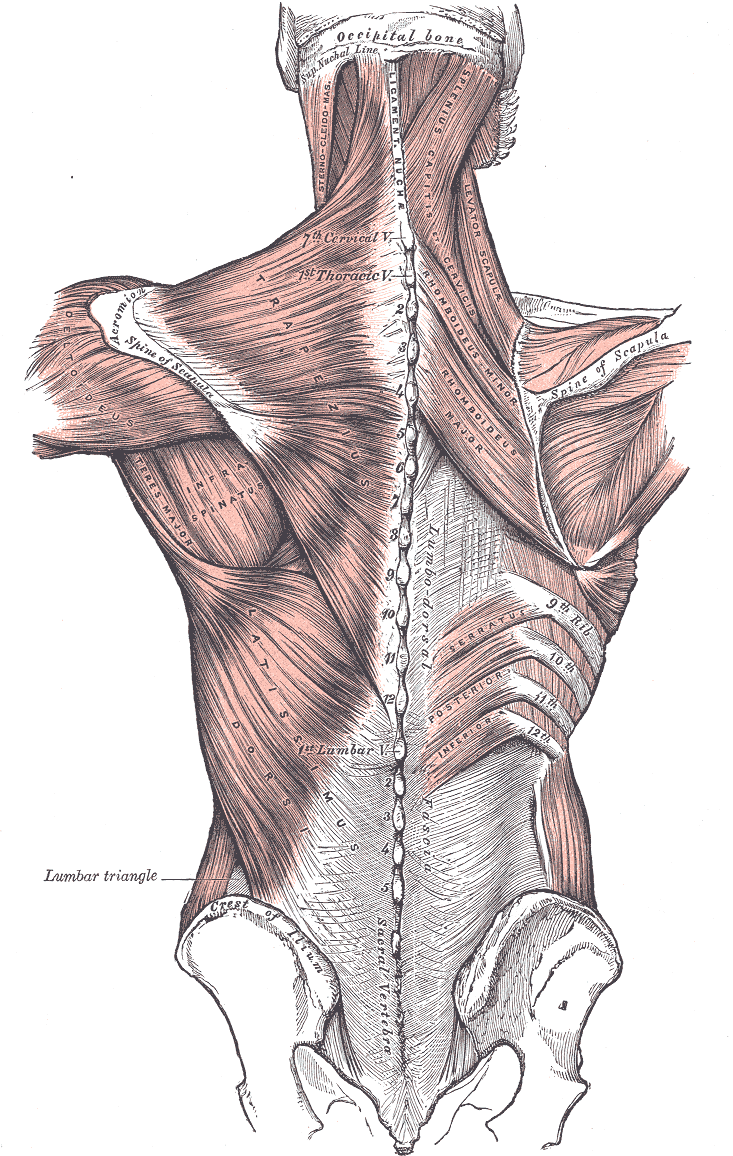
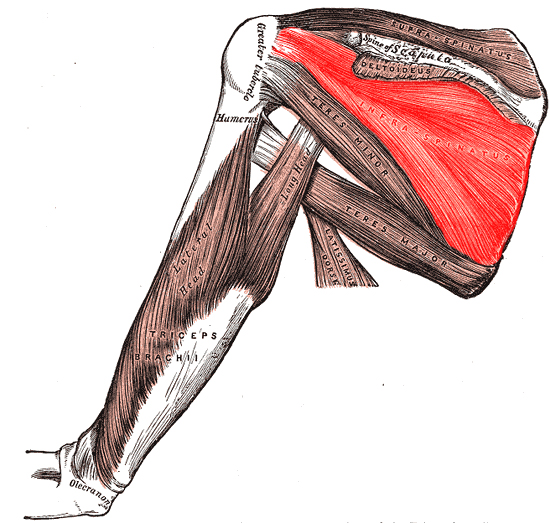
The infraspinatus originates from the medial three-quarters of the infraspinous fossa and the dorsal part of the scapula inferior to the scapular spine. The infraspinous fossa is found on the posterior scapula. The scapular spine divides the posterior aspect of the scapula into the supraspinous and infraspinous fossae. Of note, the teres minor muscle also originates from the infraspinous fossa. The distal tendinous portion runs along the lateral border of the scapular spine then passes across the posterior aspect of the shoulder joint to its insertion on the middle facet of the greater tuberosity of the humerus. This attachment is bounded by the attachments of the supraspinatus and teres minor, superiorly and inferiorly, respectively. The infraspinous fascia covers the muscle and creates a distinction between itself and the teres minor and major.[5]
The infraspinatus muscle's action on the shoulder is primarily through its function as a rotator cuff muscle providing glenohumeral stability. The rotator cuff applies compression upon the head of the humerus that allows for the stabilization of the humeral head during shoulder abduction. The muscles of the rotator cuff provide opposing forces to balance the movement of the shoulder. The infraspinatus is involved in anterior-posterior force balance as the infraspinatus provides the posterior force, and the subscapular provides the anterior force. When the rotator cuff muscles are deficient (for example, a torn infraspinatus tendon), the humeral head will elevate partially out of the glenoid fossa, decreasing the efficiency of the deltoid muscles abduction action.
The infraspinatus has actions on the head of the humerus. The infraspinatus insertion at the middle facet of the glenoid tubercle allows it to exert a lateral or external rotational force. This force is synergistic with the teres minor, as it inserts on the inferior facet of the glenoid tubercle. Compared to the other rotator cuff muscles, the infraspinatus has the second-largest anatomic footprint on the humerus. The subscapularis has the largest.
The infraspinatus also acts on the scapula. When the shoulder is held in anatomic position, the infraspinatus allows the abduction of the inferior angle of the scapula, termed scaption. Scaption makes the scapula more mobile, which assists the other shoulder muscles in allowing for full shoulder abduction.
Embryology
The infraspinatus is composed of cross-striated muscles of mesodermal origin. The shoulder muscles arise from a common early-muscle mass that is continuous with the pectoral mass and the common arm sheath known as the upper limb bud. The upper limb bud lies in opposition to somites C4, C5, C6, C7, C8, T1, and T2. In the fifth week of development, mesodermal cells from these somites travel into the limb bud and form the posterior and anterior condensation. The posterior condensation allows the creation of the following muscles: deltoid, supraspinatus, infraspinatus, teres minor, teres major, subscapularis, triceps brachii, anconeus, brachioradialis, extensor carpi radialis longus, extensor carpi radialis brevis, extensor digitorum, extensor digiti minimi, extensor carpi ulnaris, supinator, abductor pollicis longus, extensor pollicis brevis, extensor pollicis longus, and extensor indicis.
When the embryo is about 11 mm in size, the muscular mass of the deltoid begins to be transected horizontally as the scapular spine develops, and concurrently the acromion, the origin of the deltoid, forms. This muscle mass further divides to give rise to a muscle mass that soon becomes the supraspinatus and infraspinatus. This division occurs in an 11-mm to 15-mm embryo. The infraspinatus further separates itself from the teres minor and covers more of the scapula fossa with the development of the embryo, with full coverage of the fossa approximately in a 20-mm embryo.
Blood Supply and Lymphatics
The infraspinatus is supplied arterially by the suprascapular and circumflex scapular arteries.
The suprascapular artery either originates from the thyrocervical trunk or the subclavian artery. The artery runs inferolateral to the anterior scalene muscles, phrenic nerve, subclavian artery, and brachial plexus crossing posterolateral and parallel to the clavicle. Then it passes superior to the transverse scapular ligament to the supraspinous fossa. Finally, it courses laterally to the scapular spine (deep to the acromion) to the infraspinous fossa on the posterior surface of the scapula to supply the infraspinatus. The subscapular artery, a branch of the third portion of the axillary artery, gives rise to the circumflex scapular artery. The circumflex scapular artery courses around the lateral border of the scapula in its entrance into the infraspinous fossa and anastomoses with the suprascapular artery to provide a source of collateral circulation.
The lymphatic drainage is primarily of the subscapular (posterior) nodes. The subscapular nodes consist of 6 or 7 lymph nodes that lie along the posterior axillary fold. These lymph nodes run along the course of the subscapular blood vessels. The subscapular, pectoral, and humeral nodes’ efferent drainage passes through the central axillary nodes. The central axillary nodes consist of 3 or 4 nodes placed deep to the pectoralis minor near the base of the axilla, near the second part of the axilla. Efferent drainage from these central nodes passes to the apical nodes, which lie at the apex of the axilla near the medial side of the axillary vein and the first part of the axillary artery. Efferent vessels that arise from the apical group run across the cervicoaxillary canal. These efferent vessels combine to form the subclavian lymphatic trunk. The subclavian lymphatic trunk either joins the jugular and bronchomediastinal trunk to form the right lymphatic duct or may directly enter the right venous angle.
Nerves
The suprascapular nerve (C5-C6) innervates the infraspinatus. It originates at the superior trunk of the brachial plexus. It runs laterally across the lateral cervical region to supply the infraspinatus and also the supraspinatus.
Muscles
The infraspinatus is most closely associated with the subscapularis, supraspinatus, and teres minor, as they all combine around the shoulder to encircle the glenohumeral joint. These muscles act to stabilize and move the glenohumeral joint. The infraspinatus and teres minor act synergistically as external rotators of the shoulder.
Infraspinatus
- Origin: infraspinous fossa
- Insertion: greater tubercle of the humerus
- Action: lateral rotation of the humerus, external rotation of the shoulder, scaption
- Innervation: suprascapular nerve
Physiologic Variants
There are not many variants of the infraspinatus muscle in current literature, although the muscle has been found fused with the teres minor in some individuals.
Subchondral cysts can be found at the insertion of the supraspinatus and infraspinatus on the humeral head. These can be confused with rotator cuff pathology or a degenerative change. When the cysts are found on the dorsal insertion sites are typically asymptomatic. When cystic changes are identified on the anterior aspect of the humerus, a potential subscapularis lesion needs to be assessed.[4][6]
Surgical Considerations
As a muscle that forms part of the glenohumeral joint, the infraspinatus is susceptible to rotator cuff tears, usually due to anterior dislocations. In anterior shoulder dislocations, a Hill-Sachs lesion is common. The lesion is on the posterior head of the humerus resulting from the translation of the humeral head back into the glenoid cavity. In the repair of these types of lesions, the infraspinatus is used to fill the defect.[7][8][9]
A rotator cuff repair can be managed surgically or conservatively. Surgery is commonly recommended when symptoms have lasted 6 to 12 months, the tear is more than 3 cm, significant weakness or loss of function, or recent acute injury.
If surgical treatment is pursued, various approaches can be used, including open repair, arthroscopic repair, and mini-open repair.
Surgeons use the plane between the infraspinatus and teres minor as the posterior approach for shoulder arthroscopy. This posterior approach is also used for repairs of glenoid fractures and osteotomy. When preparing for an arthroscopic repair of a rotator cuff repair, it is common to begin by outlining key landmarks, including the acromion, clavicle, coracoid process, and portal placement. The posterior portal is placed distal and medial to the lateral acromion. The anterior portal is placed between the acromioclavicular joint and the coracoid process. The lateral portal is placed in line with the clavicle. During the operation, the surgeon will investigate the anatomy of the shoulder, including all four rotator cuff muscles. During the operation, the surgeon may elect to perform a subacromial bursectomy or acromioplasty. Before repairing the tendon, a debridement will be performed, and the footprint will be prepared for insertion of anchors.
Clinical Significance
Rotator cuff-related pathologies lead to 4.5 million visits and 40,000 surgical procedures annually in the United States alone. The rate of rotator cuff pathology is estimated to affect 16 to 34% of people, with incidence increasing with age. Causes of rotator cuff-related pain include acute and chronic injury patterns, including trauma, repetitive activity, impingement, and degeneration. When investigating rotator cuff pathologies, an MRI is the imaging modality of choice. The muscle group is best demonstrated on a sagittal oblique T1 weighted section.[10]
On physical exam, if there are signs of atrophy of the supraspinatus and infraspinatus muscles, there is usually an associated compression of the suprascapular nerve near the scapular notch. This compression can be seen in overhead throwing motion athletes such as swimmers or baseball players and superior labrum anterior and posterior (SLAP) tears. If there is isolated weakness or atrophy of the infraspinatus muscle, there is usually an associated nerve compression at the spinoglenoid notch. The compression of the nerve at the spinoglenoid notch is usually due to a ganglion cyst. Atrophy of the muscle may also be due to tendinous ruptures greater than five centimeters or chronic rotator cuff tears. Weakness in external rotation of a 90-degree flexed arm may be an indication of rotator cuff tears or tendinous rupture of the infraspinatus.[11]