Introduction
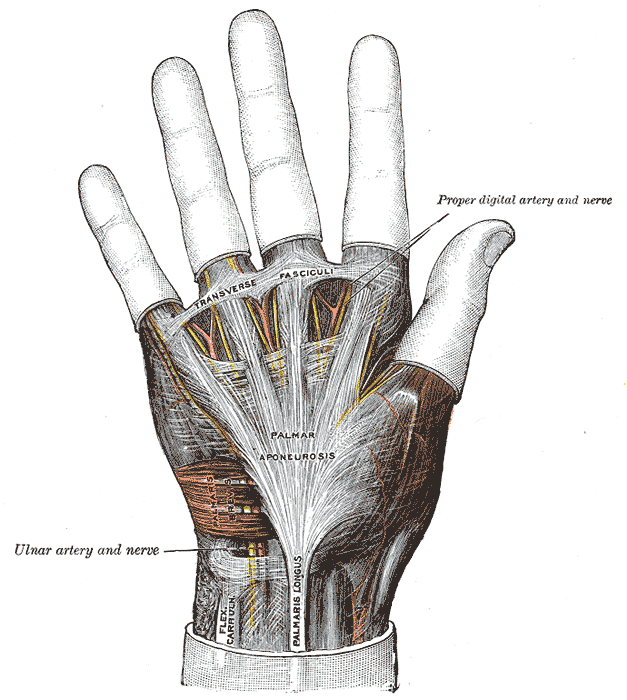
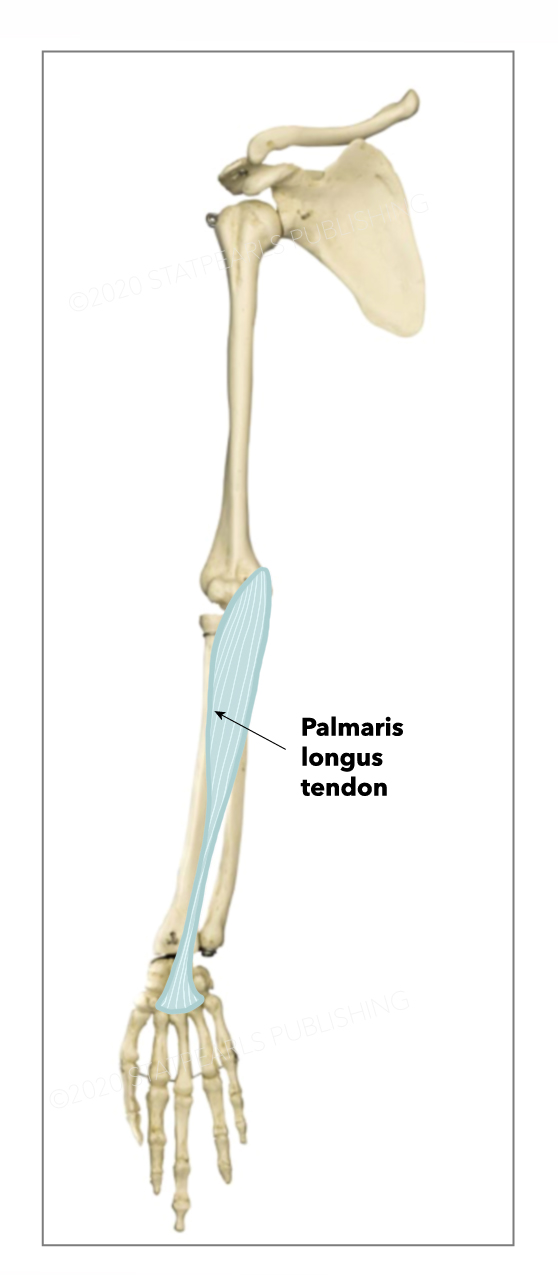
The palmaris longus is a small, fusiform-shaped muscle located on the anterior forearm of the human upper extremity. This muscle belongs to the superficial forearm flexor group, with a most common proximal attachment at the medial epicondyle of the humerus via the common forearm flexor tendon and a most common distal attachment into the connective tissue fibers of the palmar aponeurosis and the flexor retinaculum, a ligamentous structure forming the roof of the carpal tunnel and containing the median nerve and digital flexor tendons.[1] The palmaris longus can be morphologically quite variable but most commonly has a tendinous proximal attachment, a mid-length, spindle-shaped muscle belly, and a long and thin tendinous distal portion. The majority of fibers in the palmaris longus tendon pass superficially to the flexor retinaculum, the tendon broadens into a flattened collection of fibers, and the fibers interweave with the palmar aponeurosis.[1]
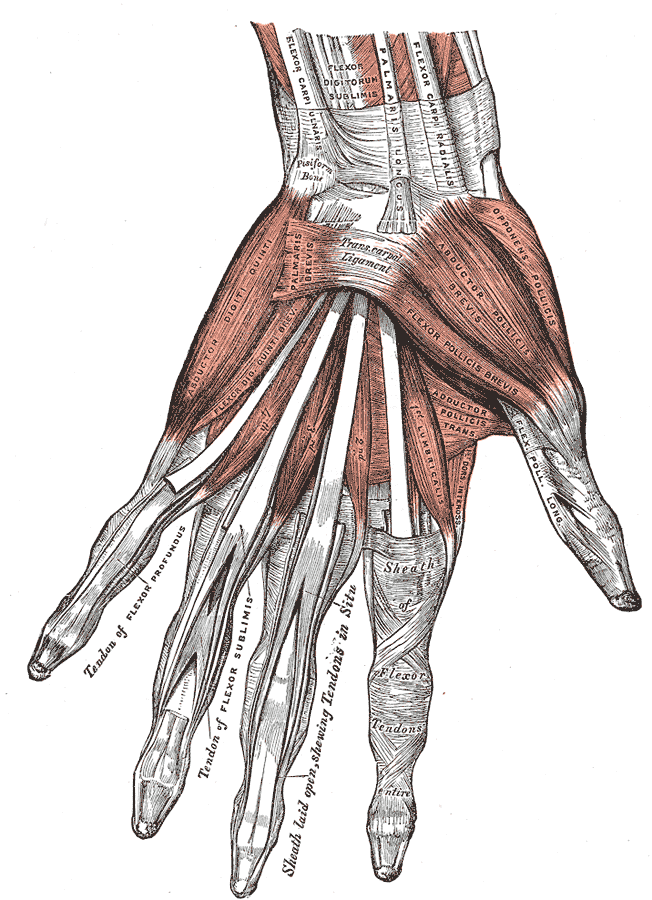
The functional contribution of the palmaris longus appears to be minimal, but it has clinical significance due to its frequent intraoperative harvest for many surgical procedures, often involving tendon repair in the upper extremity. The thin distal tendinous portion, superficial location, and lack of functional significance make the muscle easily accessible and ideal for intraoperative harvest for tendon reconstruction and other surgical procedures.[1] The palmaris longus muscle is commonly present but may be absent in a small percentage of the population, ranging from 2.5% to 26% of individuals, depending on the studied population.[1],[2] The palmaris longus tendon is located near the anatomical center of the anterior wrist, medial to the tendon of flexor carpi radialis, and lateral to the tendon of flexor carpi ulnaris.[1] The muscle’s presence can be assessed clinically by several physical exam maneuvers, with the Schaeffer test being the most commonly used. To perform the Schaeffer test, ask the patient to touch the pads of the thumb and little finger together while flexing the wrist, and if present, the tendon of palmaris longus should protrude anteriorly at the wrist joint.[3] Congenital absence of the muscle is common but has demonstrated decreased grip strength or any other functional deficit.[4]