[1]
Regional nerve blocks of the face., Moskovitz JB,Sabatino F,, Emergency medicine clinics of North America, 2013 May
[PubMed PMID: 23601486]
[2]
Robson AK,Bloom PA, Suturing of digital lacerations: digital block or local infiltration? Annals of the Royal College of Surgeons of England. 1990 Nov;
[PubMed PMID: 2241053]
[3]
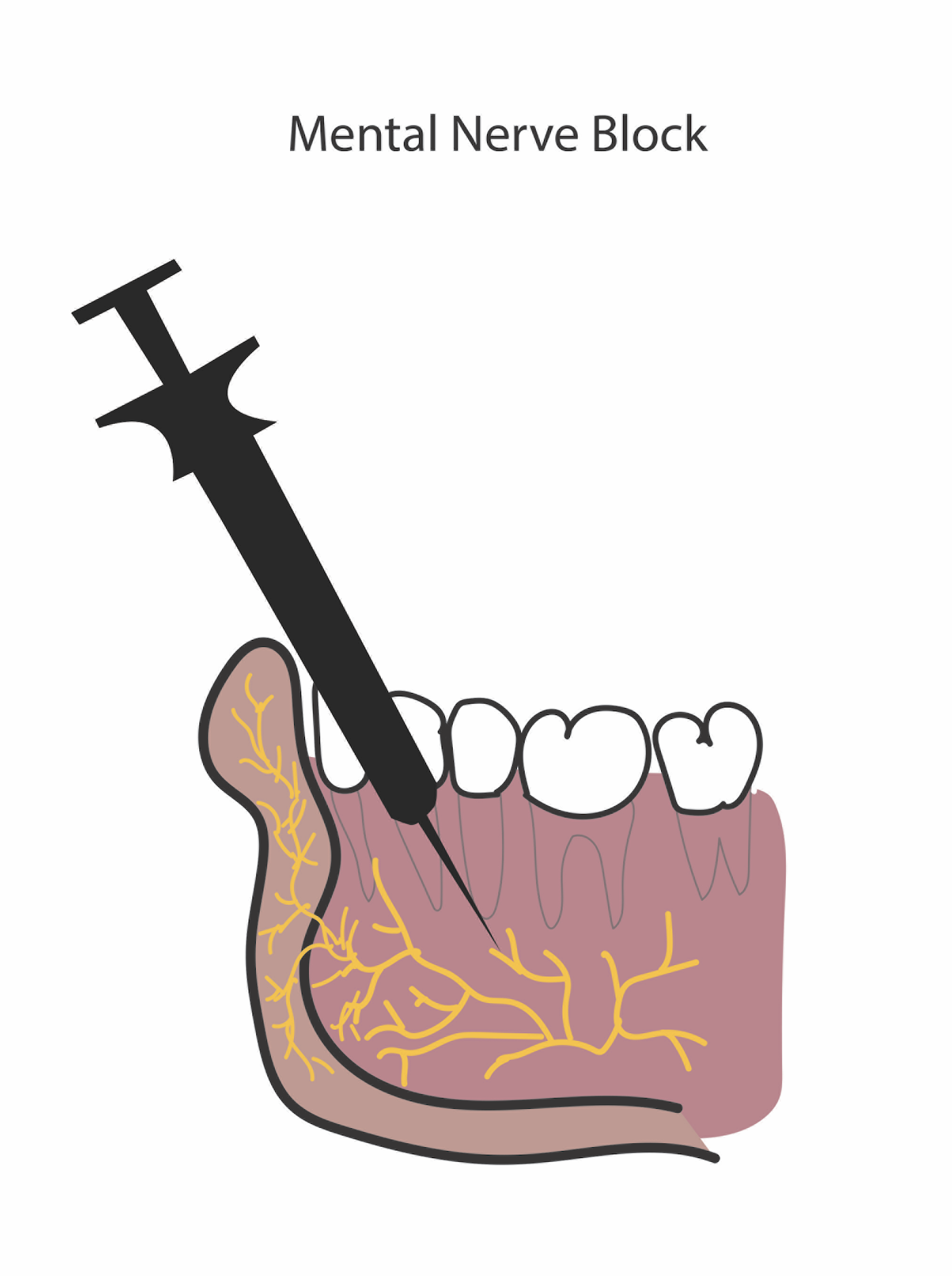
A comparative study of the percutaneous versus intraoral technique for mental nerve block., Syverud SA,Jenkins JM,Schwab RA,Lynch MT,Knoop K,Trott A,, Academic emergency medicine : official journal of the Society for Academic Emergency Medicine, 1994 Nov-Dec
[PubMed PMID: 7600396]
Level 2 (mid-level) evidence
[4]
Khalil H, A basic review on the inferior alveolar nerve block techniques. Anesthesia, essays and researches. 2014 Jan-Apr;
[PubMed PMID: 25886095]
[5]
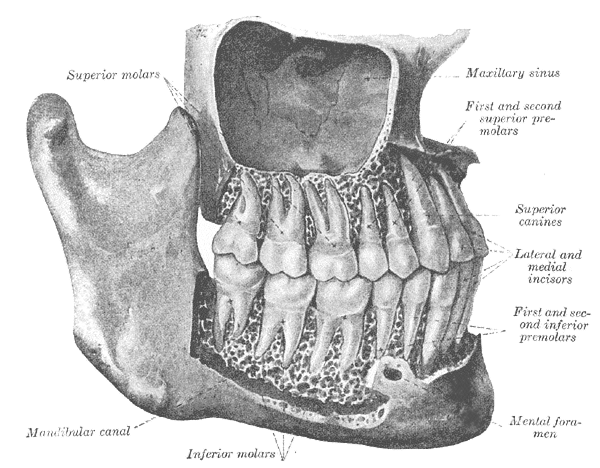
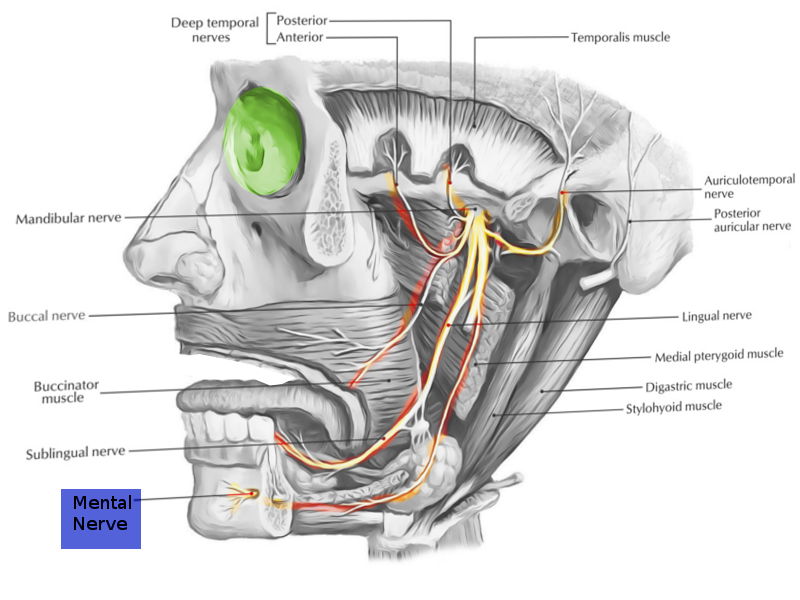
Greenstein G,Tarnow D, The mental foramen and nerve: clinical and anatomical factors related to dental implant placement: a literature review. Journal of periodontology. 2006 Dec
[PubMed PMID: 17209776]
[6]
The position of the mental foramen in dentate and edentulous mandibles: clinical and surgical relevance., Charalampakis A,Kourkoumelis G,Psari C,Antoniou V,Piagkou M,Demesticha T,Kotsiomitis E,Troupis T,, Folia morphologica, 2017 May 29
[PubMed PMID: 28553857]
[7]
Tan FF,Schiere S,Reidinga AC,Wit F,Veldman PH, Blockade of the mental nerve for lower lip surgery as a safe alternative to general anesthesia in two very old patients. Local and regional anesthesia. 2015;
[PubMed PMID: 25999760]
[8]
An evaluation of the incisive nerve block and combination inferior alveolar and incisive nerve blocks in mandibular anesthesia., Nist RA,Reader A,Beck M,Meyers WJ,, Journal of endodontics, 1992 Sep
[PubMed PMID: 9796516]
[9]
Influence of injection speed on the effectiveness of incisive/mental nerve block: a randomized, controlled, double-blind study in adult volunteers., Whitworth JM,Kanaa MD,Corbett IP,Meechan JG,, Journal of endodontics, 2007 Oct
[PubMed PMID: 17889680]
Level 1 (high-level) evidence
[10]
Evaluation of the effectiveness and comfort of incisive nerve anesthesia given inside or outside the mental foramen., Joyce AP,Donnelly JC,, Journal of endodontics, 1993 Aug
[PubMed PMID: 8263444]