Introduction
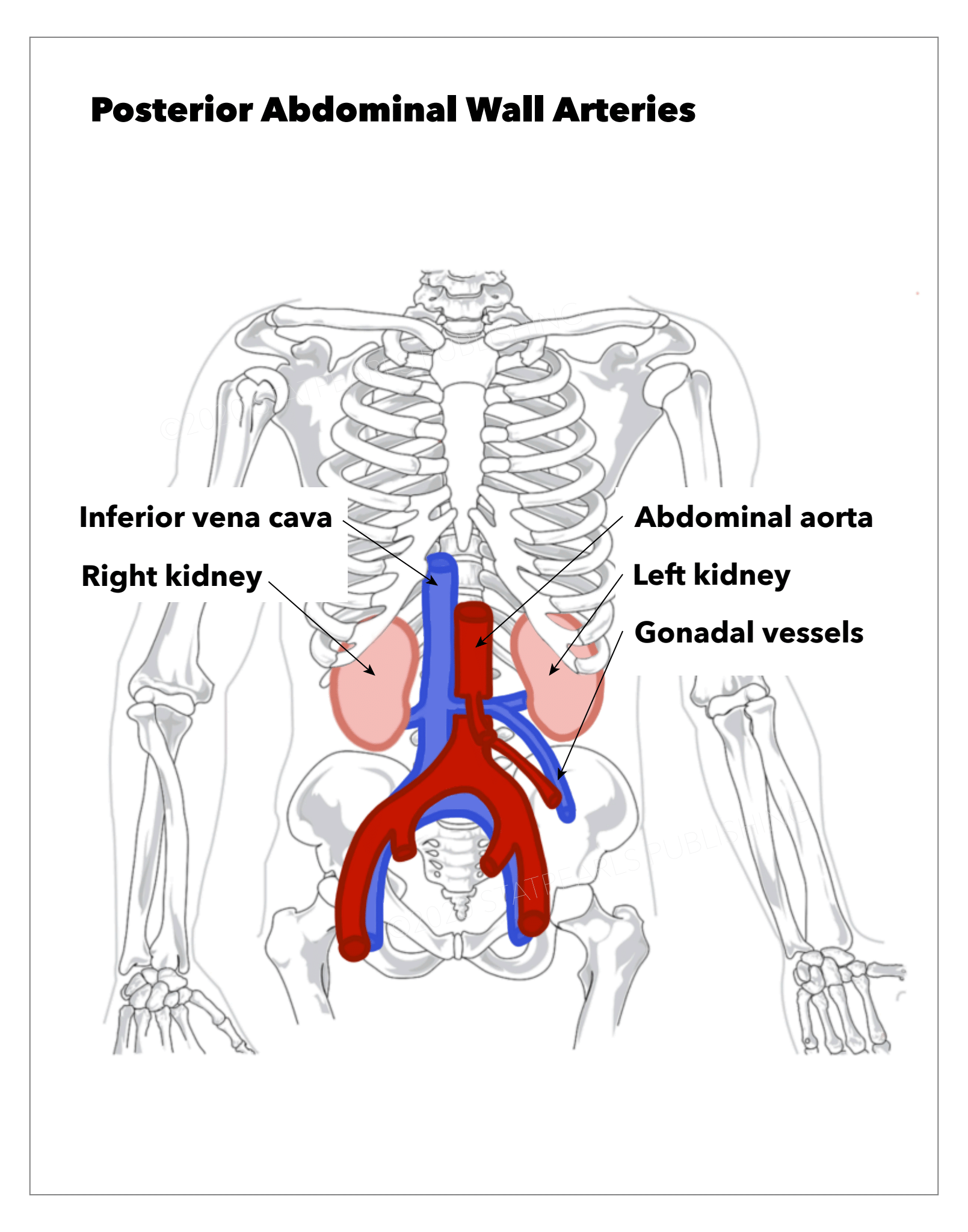
Several arteries course through the posterior abdominal wall (see Image. Posterior Abdominal Wall Arteries).
- The aorta passes the aortic hiatus at the T12 level through the diaphragm and descends anterior to the vertebral column. The aorta branches into the right and left common iliac arteries at L4. The aorta gives rise to the inferior phrenic arteries just below the aortic hiatus. These vessels supply the diaphragm and also give rise to the suprarenal vessels.
- The renal arteries arise from the aorta just inferior to the origin of the superior mesenteric artery. The right renal artery is longer and a little inferior to the left renal artery and traverses behind the inferior vena cava (IVC). The left renal artery passes posterior to the left renal vein.
- Testicular or ovarian arteries descend into the retroperitoneum and run laterally on the psoas major muscle and across the ureter. The testicular artery accompanies the ductus deferens into the scrotum. Here it provides blood to the epididymis, testis, and spermatic cord. The ovarian artery traverses through the suspensory ligament of the ovary, supplies the ovary, and anastomosis with the ovarian branch of the uterine artery.
- Lumbar arteries consist of 4 or 5 pairs that originate from the back of the aorta. These vessels require ligation when performing aortic aneurysm surgery. They run posterior to the sympathetic trunk, the IVC (on the right side), the quadratus lumborum, and psoas major muscles. The lumbar vessels give off numerous small anterior branches and accompany the dorsal primary rami of the corresponding spinal nerves and divide into spinal and muscular branches.
- The middle sacral artery comes off the posterior of the aorta, just above the bifurcation; the vessel then runs down the anterior of the sacrum and ends at the coccygeal body. It supplies the anal canal and rectum and joins the superior and inferior rectal arteries.
In the posterior abdominal wall, other important vessels that are not arteries include:
- IVC is formed by the union of the two common iliac veins just to the right of L5. The bifurcation of the IVC is almost always lower than the bifurcation of the aorta in the pelvis. As it ascends, the IVC remains to the right of the aorta. At the diaphragm, it ascends through the IVC hiatus at T8 and enters the right atrium. Through its course, it receives venous blood from the adrenals, renal veins, right gonads, hepatic veins, and inferior phrenic veins.
- The cisterna chyli, formed by the lumbar and intestinal lymphatics, lies just posterior and to the right of the aorta. It is usually located between the two crura of the diaphragm and ascends through the aortic hiatus in the diaphragm. The cisterna chyli is the inferior collecting sac of the thoracic duct, which returns chyle to the venous system at the left brachiocephalic vein, where the left subclavian and left internal jugular veins converge.
- The para-aortic lymph nodes can divide into subgroups, which include the preaortic, retroaortic, and lateral aortic groups. The preaortic nodes are located next to the origin of the celiac trunk, superior and inferior mesenteric arteries.
Surgeons, radiologists, and other health professionals need to be familiar with these vessels as multiple pathologic conditions may develop, resulting in untoward consequences from vessel injury (see Image. Bolus Tracking).