Introduction
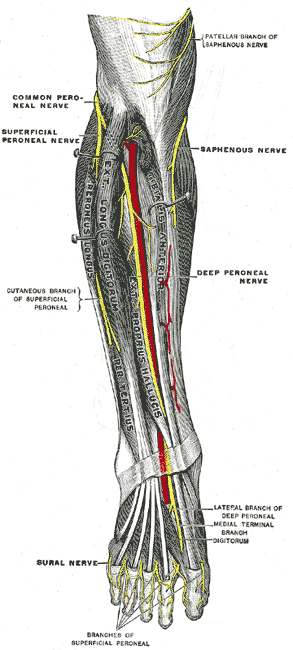
The deep peroneal nerve is also known as the deep fibular nerve. It originates after the bifurcation of the common peroneal nerve between the upper segment of the peroneus longus and the head of the fibula.[1] The common peroneal nerve (spinal nerves L4 through S1) itself originates from the bifurcation of the sciatic nerve (spinal nerves L4 through S3) which terminates at the apex of the popliteal fossa into the common peroneal and the tibial nerve after wrapping around the neck of the fibula.[2],[3] After bifurcation from the common peroneal nerve, the deep peroneal nerve then traverses deep to the extensor digitorum longus and runs on the anterior surface of the interosseous membrane.[1] In the middle of the leg, it is in close association with the anterior tibial artery and then descends with the artery to lie in front of the ankle joint. Here, it gives off the lateral and medial terminal branches. The medial terminal branch accompanies the dorsalis pedis and runs on the dorsum of the foot reaching the first interosseous space where it divides into digital nerves that supply the side of the great and second toes. The lateral terminal branch runs beneath the extensor digitorum brevis and gives off interosseous branches that supply the tarsal and metatarsophalangeal joints.[1]