Introduction
The submandibular triangle is an important anatomic landmark located underneath the body of the mandible. The majority of the anatomic space bounded by the submandibular triangle consists of the submandibular gland. The submandibular gland is the second largest salivary gland in the body (the parotid gland is the largest). In addition to housing the submandibular gland, a vast array of nerves, arteries, veins, and lymphatics course within the boundaries of the submandibular triangle. The complexity of the anatomy within the submandibular triangle makes for important clinical implications when performing surgery in this region. This article will focus on the anatomy contained within the borders of the submandibular triangle as well as the clinical significance and implications of surgery in this area.[1][2]
Structure and Function
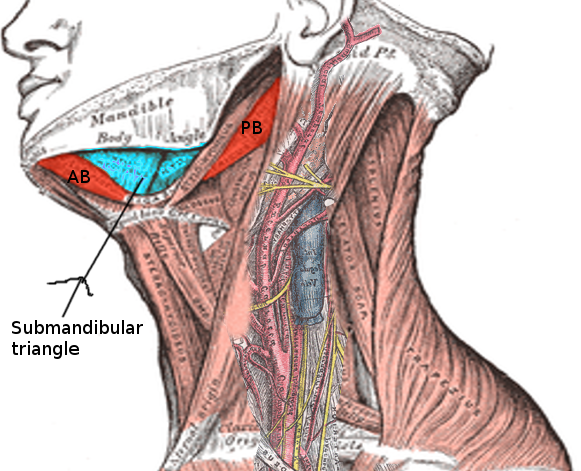
The submandibular triangle is bounded anteriorly by the anterior belly of the digastric muscle and posteriorly by the posterior belly of the digastric muscle.[3] The superior border of the triangle is the inferior border of the mandible. The triangle's floor is formed by the mylohyoid muscle.[3] Odontogenic infections, particularly from wisdom teeth, can spread below the mylohyoid muscle into the submandibular triangle.[3] The hyoid bone borders the triangle inferiorly.
Superficial to deep dissection of the submandibular triangle involves passing through the skin, subcutaneous fat, superficial cervical fascia, platysma muscle, and deep cervical fascia before reaching the submandibular gland. The majority of the space within the triangle is taken up by the submandibular gland that helps produce salivary fluid secreted into the oral cavity. Additionally, the gland helps to facilitate lymph drainage from the lower gums, tongue, the floor of the mouth, and tonsils into the 3-6 lymph nodes contained within the triangle which lie adjacent to the submandibular gland. Unlike the parotid gland, the submandibular gland contains no intraglandular lymph nodes.[1][2]
Embryology
The first, second, and third pharyngeal arches play a role in the development of the submandibular triangle. The first pharyngeal arch is the progenitor to the mandible while the second and third give rise to the hyoid. The majority of the contents of the submandibular triangle are contained between these structures and primarily arise from mesoderm and neural crest derivatives. The submandibular gland arises from an outpouching of endodermal tissue.[4][5]
Blood Supply and Lymphatics
The blood vessels and lymphatics that course through the submandibular triangle are significant landmarks to note for surgical incision into the triangle. The facial artery, being the fourth branch of the external carotid artery, courses underneath the posterior belly of the digastric and sits behind the submandibular gland in the triangle. After the artery passes posterior to the submandibular gland, it courses superiorly across the inferior border of the mandible. The submental artery and mylohyoid artery also course deep to the submandibular gland within the triangle. The submandibular lymph nodes follow the veins in the triangle and drain many of the inferior portions of the oral cavity. The facial vein runs superficially to the submandibular gland and eventually joins the anterior branch of the retromandibular vein, forming the common facial vein that drains into the internal jugular vein.[1][2]
Nerves
Nerves that course through and around the submandibular triangle are essential surgical landmarks to recognize as resection can lead to numerous adverse outcomes. The most superficial of these nerves include the marginal mandibular branch of the facial nerve superiorly and the cervical branch of the facial nerve inferiorly. Nerves that course deeper in the triangle include the lingual nerve; a division of the mandibular branch of the trigeminal nerve (V3), and the hypoglossal nerve; cranial nerve XII. The mylohyoid muscle is supplied by the mylohyoid nerve from the alveolar branch of V3, which lies on the inferior portion of the muscle.[1][2]
Muscles
The submandibular triangle is bordered by muscles that delineate its borders along with the inferior border of the body of the mandible. These include the anterior and posterior bellies of the digastric muscle, and the mylohyoid muscle deep. Superficially, the platysma courses across the triangle.[1]
Surgical Considerations
Surgical considerations within the submandibular triangle involve detailed knowledge of the anatomy of the area to avoid post-operative complications. This anatomical understanding should include both the structures contained in, as well as those surrounding structures of the triangle. The most common post-operative complications from excision of both benign and malignant submandibular triangle masses include temporary or permanent marginal mandibular nerve weakness, and hematoma. Resection of other nerves present within the triangle may be necessary depending on the depth of invasion of the neoplasm. This may involve damage to the lingual or hypoglossal nerves.[6][7][8]
Clinical Significance
The clinical significance of the submandibular triangle is vast due to the complex anatomy present in and around this region. Pathology arising in the submandibular triangle includes infectious, immunologic, and neoplastic processes.
The most common pathology arising in the submandibular triangle is sialadenitis or inflammation of the submandibular salivary gland. Sialadenitis in the submandibular gland is typically caused by sialolithiasis, consisting of a precipitated stone that blocks salivary flow through the submandibular gland duct or Wharton’s duct. This usually results in postprandial unilateral painful swelling in the submandibular triangle with resulting edema and reddening of the skin. Sialadenitis caused by sialolithiasis is diagnosed clinically and confirmed with imaging such as ultrasound, computerized tomography, and magnetic resonance imaging. Treatment of acute sialadenitis includes antibiotic therapy, hydration, NSAIDs, and gentle massage. Antibiotic coverage for the treatment of sialadenitis is aimed at the coverage of both aerobic and anaerobic pathogens. Treatment of sialadenitis secondary to sialolithiasis may necessitate surgical removal of the obstructing stone by either open surgery or sialendoscopy. Other infectious etiologies of sialadenitis include pathogens related to insufficient oral hygiene, HIV, and mumps. Mumps infection is most commonly seen in the parotid gland manifesting as parotitis. However, cases of sialadenitis isolated to one or both submandibular glands have been reported.
Non-infectious, immunologic pathology arising within the submandibular gland include chemical sensitivities and autoimmune disorders. One such chemical sensitivity includes sialadenitis caused by iodide contrast dye. The pathophysiology of iodide-associated sialadenitis is thought to be due to an elevated concentration of salivary iodine, resulting in swelling of the duct mucosa and impairment of salivary excretion. Another cause of non-infectious sialadenitis includes autoimmune immunoglobulin G4-related sialadenitis (IgG4-RS). IgG4-RS typically presents as bilateral inflammation of the submandibular and/or parotid glands with associated xerostomia from a reduced salivary flow. Unlike Sjogren’s syndrome, IgG4-RS occurs more commonly in males that are typically middle-aged and presents serologically with elevated IgG4 and IgE levels. IgG4-RS is progressive and causes fibrosis of the submandibular gland. Diagnostic workup usually consists of imaging with ultrasound or positron emission tomography (PET) and is confirmed with biopsy. The first line of treatment for IgG4-RS involves glucocorticoid therapy. Studies suggest that early intervention with glucocorticoids results in reduced fibrosis and improved clinical outcomes.
Neoplasms that arise in the submandibular triangle can be divided into benign and malignant masses. Evaluation of these masses involves imaging studies with ultrasound, computerized tomography (CT), or magnetic resonance imaging (MRI), followed by fine-needle aspiration biopsy for confirmation. Treatment of all neoplasms requires surgical resection. The degree of surrounding tissue and lymph nodes surgically removed in addition to the mass is case-dependent and is a function of the etiology and aggressiveness of the neoplasm. The most common benign neoplasm seen in the submandibular triangle is a pleomorphic adenoma, followed by adenolymphoma, also known as Warthin’s tumor. The most common malignant neoplasm is adenoid cystic carcinoma, followed by mucoepidermoid carcinoma. Mucoepidermoid carcinoma is statistically the most common overall malignancy of the salivary gland, but the second most common malignancy of the submandibular gland. Both malignant neoplasms are aggressive in nature, and rapid diagnosis followed by surgical excision improves morbidity and mortality. Other benign and malignant neoplasms arising from within the submandibular triangle have been reported but are exceedingly rare in incidence.[1][9][10][11][8]