Introduction
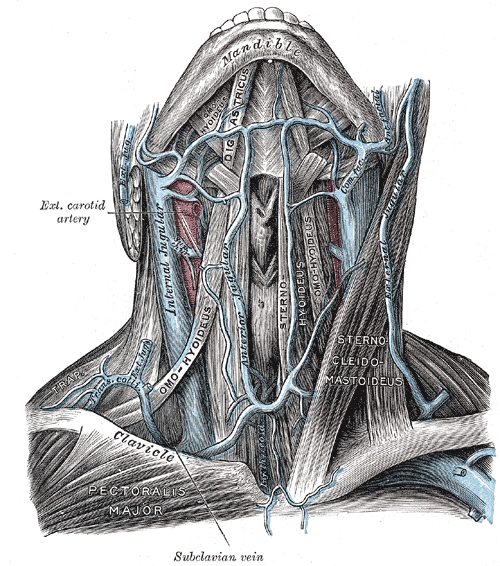
The external jugular vein, located in the anterior and lateral neck, receives blood from the deeper parts of the face as well as the scalp — the external jugular vein forms from the combination of the posterior auricular and retromandibular vein. The external jugular vein starts in the parotid at the level of the angle of the mandible and runs vertically down the neck along the posterior border of the sternocleidomastoid muscle. At its distal end, the external jugular vein perforates the deep neck fascia and terminates in the subclavian vein. Throughout its course in the neck, the vein is immediately deep to the platysma muscle. During its course from the mandible, it runs parallel with the greater auricular nerve. Like most veins, the external jugular vein also has valves at the terminal end before it enters the subclavian vein. In patients with obstruction or occlusion of the subclavian vein, the external jugular may appear dilated. The vein is not always easily visible on external examination, particularly in obese patients. The size of the external jugular vein does vary with body habitus and size of the neck. In rare cases, there may be two small external jugular veins. The is some variation in course as it descends into the neck, but its path is more consistent than the anterior jugular. Awareness of its location is essential during head and neck surgery, where injury should be avoided (it can also be harvested as a vein graft). The vein can be cannulated to provide fluids and medications during resuscitation when more peripheral access cannot be easily established.[1]