Introduction
The scapula is a flat, triangular-shaped bone (colloquially as the "shoulder blade"). It is located in the upper thoracic region on the dorsal surface of the rib cage. It connects with the humerus at the glenohumeral joint as well as the clavicle at the acromioclavicular joint to form the shoulder joint. In total, 17 different muscles attach to the scapula, which makes it difficult to fracture.
Structure and Function
The scapula is a site of attachment for many muscles and has several processes, projections, and surfaces for attachment. The scapula has three angles (superior/medial, lateral, inferior), three borders (medial, lateral/axillary, and superior), and two surfaces (ventral and dorsal). The scapula has three processes: the acromion, the spine, and the coracoid process. Muscle attachments to these landmarks are covered in the "Muscles" section.
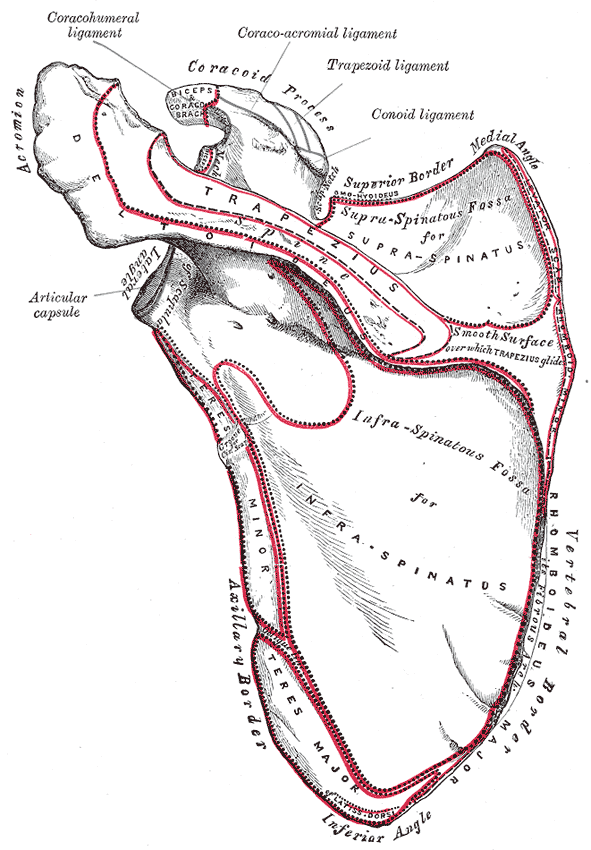
The ventral surface of the scapula abuts the thoracic rib cage and has a large concavity called the subscapular fossa where the subscapularis attaches. Three ridges within this fossa allow for tendinous attachment. The dorsal surface divides into two unequal parts via the scapular spine which runs across from the posterior scapula before forming the acromion. Above the spine is the supraspinous fossa and below it is the infraspinous fossa. A ridge runs down the infraspinous fossa near the lateral border from the glenoid cavity to just above the inferior angle. This ridge separates the teres major and minor muscles from the infraspinatus muscle. The spinoglenoid notch connects the two fossae, which is situated under the acromion and is where the suprascapular nerve and artery run on the way to supplying the infraspinatus muscle. The acromion is an oblong continuation of the spine that runs laterally then anteriorly above the supraspinous fossa and is the summit of the shoulder on palpation. The superior border of the scapula extends from the superior angle to the coracoid process. The coracoid process is a hook-like structure that comes off anteriorly from the lateral superior aspect of the ventral side of the scapula. Like the acromion, it is an attachment point for muscles and ligaments.
At the base of the coracoid, there is a notch that is closed off by the superior transverse scapular ligament superiorly, forming a foramen. The suprascapular nerve runs through this foramen while the suprascapular artery runs just above the ligament. The lateral angle of the scapula is the location of the glenoid cavity; this is where the humeral head articulates with the scapula. At the margins of this cavity, a fibrocartilagenous structure called the glenoid labrum acts to deepen the cavity as to accommodate more of the humeral head. Just below the cavity is an impression called the infraglenoid tuberosity where the long head of the triceps brachii originates. The ligaments of the scapula are predominantly named based on the two points they attach. They are the transverse scapular ligament (discussed earlier), coracoacromial ligament, coracoclavicular ligament, coracohumeral ligament, glenohumeral ligaments, and acromioclavicular ligament.
The muscles that attach to the scapula allow it to perform six movements:
- Elevation: The upper trapezius and levator scapulae raise the scapula
- Depression: The lower trapezius brings down the scapula
- Upward rotation: The upper and middle trapezius rotate the scapula during upper extremity abduction
- Downward rotation: The rhomboids rotate the scapula when reaching behind the back and downward
- Retraction (adduction): The rhomboids and middle trapezius separate the scapula from the thoracic wall, active when performing rowing motions
- Protraction (abduction): The serratus anterior brings the scapula against the thoracic wall, active when reaching forward
Embryology
As with other bones, the scapula is derived from the embryologic mesoderm. Its osteogenic development beings in week 11 of human embryogenesis. [1]
Blood Supply and Lymphatics
The blood supply of the posterior surface of the scapula is composed of an anastomosis of several arteries derived from the thyrocervical trunk (a branch of the subclavian artery) and axilla artery (continuation of the subclavian artery beyond the lateral margin of the first rib):
- Thryocervical trunk branches:
- Transverse cervical artery - runs along the medial border of the scapula. May provide a deep (or descending) branch that is also known as the dorsal scapular artery. However, this artery more often branches off the subclavian artery.
- Suprascapular artery - Mostly supplies supraspinatus and infraspinatus muscles.
- Subclavian artery branches:
- Subscapular artery - Provides blood supply for subscapularis muscle as far as the inferior angle of the scapula
- Circumflex scapular artery - branch of the subscapular artery. Forms an anastomosis with the suprascapular artery and the deep branch of the transverse cervical artery.
Venous drainage of the scapula: Primarily via the axillary vein and suprascapular veins
Lymphatic drainage:
- Right scapula - Right lymphatic duct
- Left scapula - Thoracic duct
- The lymph nodes associated with the scapula include the axillary and the supraclavicular lymph nodes.
Nerves
See "Muscles" section for innervations of muscles attached to the scapula.
Muscles
The intrinsic muscles of the scapula attach directly to the surface of the bone. These muscles are the four members of the rotator cuff and act to stabilize the glenohumeral joint. These include:
Supraspinatus
- Function: Initiation of arm abduction (first 15 degrees), stabilize glenohumeral joint
- Origin: Supraspinous fossa
- Insertion: Top of the greater tubercle
- Innervation: Suprascapular nerve (C5, C6)
Infraspinatus
- Function: Lateral rotation of the arm, stabilize glenohumeral joint
- Origin: Infraspinous fossa
- Insertion: Greater tubercle of humerus, between the supraspinatus and teres minor insertion
- Innervation: Suprascapular nerve (C5, C6)
Teres minor
- Function: Lateral rotation of the arm, stabilize glenohumeral joint
- Origin: Lateral/axillary border and adjacent posterior aspect of the scapula
- Insertion: Inferior aspect of the greater tubercle on the humerus
- Innervation: Axillary nerve (C5, C6)
Subscapularis
- Function: Adduction and medial rotation of the arm, stabilize glenohumeral joint
- Origin: Subscapular fossa
- Insertion: Lesser tubercle of humerus
- Innervation: Subscapular nerves (C5, C6, C7)
The extrinsic muscles of the scapula attach to the processes of the scapula and affect motion at the glenohumeral joint: These include:
Biceps brachii
- Function: Resists dislocation of the shoulder, major flexor of the forearm, supination of the forearm
- Origin:
- Short head: coracoid process
- Long head: supraglenoid tubercle
- Insertion: Radial tuberosity and forearm fascia (as bicipital aponeurosis)
- Innervation: Musculocutaneous nerve (C5, C6)
Triceps brachii
- Function: Resists dislocation of the shoulder, major extensor of the forearm
- Origin:
- Lateral head: above the radial groove,
- Medial head: below the radial groove
- Long head: infraglenoid tubercle of scapula
- Insertion: Olecranon process of ulna and fascia of the forearm
- Innervation: Radial nerve (C6, C7, C8)
Deltoid
- Function:
- Anterior aspect is responsible for flexion and medial rotation of the arm
- Middle aspect is responsible for abduction of the arm (up to 90 degrees)
- The posterior aspect is responsible for extension and lateral rotation of the arm
- Origin: Lateral clavicle, acromion and scapular spine
- Insertion: Deltoid tuberosity
- Innervation: Axillary nerve (C5, C6)
Stabilizing muscles of the scapula include:
Trapezius
- Function:
- Upper fibers elevate the scapula and rotate it during abduction of the arm (90 to 180 degrees)
- Middle fibers retract the scapula
- Lower fibers pull the scapula inferiorly.
- Origin: Skull, nuchal ligament and the spinous processes of C7 to T12
- Insertion: clavicle, acromion and the scapular spine
- Innervation: Accessory nerve (Cranial nerve XI)
Levator scapulae
- Function: Elevates the scapula
- Origin: Transverse processes of the C1 to C4 vertebrae
- Insertion: Medial border of the scapula
- Innervation: C3, C4, and the Dorsal scapular nerve (C5)
Serratus anterior
- Function: fixes the scapula into the thoracic wall, and aids in rotation and abduction of the arm (90 to 180 degrees)
- Origin: Surface of the upper eight ribs at the side of the chest
- Insertion: Along the entire anterior length of the medial border of the scapula
- Innervation: Long thoracic nerve (C5, C6, C7)
Rhomboid major
- Function: Retracts and rotates the scapula
- Origin: Spinous processes of T2 to T5 vertebrae
- Insertion: Inferomedial border of the scapula
- Innervation: Dorsal scapular nerve (C5)
Rhomboid minor
- Function: Retracts and rotates the scapula
- Origin: Spinous processes of C7 to T1 vertebrae
- Insertion: Medial border of the scapula
- Innervation: Dorsal scapular nerve (C5)
Other muscles attached to the scapula include:
Latissmus dorsi
- Function: Extends, adducts and medially rotates the upper limb
- Origin: Spinous processes of T6 to T12, iliac crest, thoracolumbar fascia, the inferior three ribs, and the inferior angle of the scapula
- Insertion: Intertubercular sulcus of the humerus
- Innervation: Thoracodorsal nerve (C6, C7, C8)
Teres major
- Function: Adduction and medial rotation of the arm
- Origin: Posterior surface of the scapula at its inferior angle
- Insertion: Intertubercular groove on its medial aspect
- Innervation: Lower scapular nerve (C5, C6)
Pectoralis minor
- Function: Depression of the shoulder, protraction of the scapula
- Origin: Third, fourth, fifth ribs close to their respective costal cartilages
- Insertion: Coracoid process
- Innervation: Medial pectoral nerve (C8, T1)
Coracobrachialis
- Function: Flexion and adduction of the arm
- Origin: Coracoid process
- Insertion: Middle of the humerus, on its medial aspect
- Innervation: Musculocutaneous nerve (C5, C6, C7)
Omohyoid
- Function: Pulls hyoid bone down, active while talking and swallowing
- Origin: Superior border of scapula
- Insertion: Inferior edge of the hyoid
- Innervation: Ansa cervicalis (C1, C2, C3)
Physiologic Variants
Os acromiale - Unfused center of secondary ossification in the acromion that may cause pain and tenderness. It is thought to increase the risk of impingement and rotator cuff tears. Initial treatment can be conservative, but surgical excision of the unfused fragment is an option in refractory cases.[2]
Sprengel deformity - Congenital elevation of the scapula that leads to decreased functionality of the scapula and upper limb. Surgical reconstruction is the usual approach to correct the cosmetics and functionality of the scapula. This is a rare condition, but it is the most common variant of the scapula.[3]
Surgical Considerations
Surgical interventions involving the scapula occurs most commonly in shoulder arthroplasty, as the glenoid fossa and labrum compose the scapular portion of the shoulder joint. Indications for shoulder arthroplasty include shoulder osteoarthritis or inflammatory arthritis refractory to conservative management and other proximal humeral or rotator cuff pathologies refractory to conservative management. During shoulder arthroplasty, particular caution should be taken to avoid axillary nerve injury.
Clinical Significance
Scapular Winging[4][5]
Injury causing denervation of the long thoracic nerve leads to paralysis of the serratus anterior, the primary muscle involved in protracting and pulling the scapula toward the rib cage. This weakened protraction allows the rhomboid muscles and the trapezius to work unopposed, leading to retraction of the medial scapula and elevation of the entire scapula. The result is medial winging of the scapula and limitation functionality of the upper extremity. Less commonly, palsy of the trapezius or rhomboids may cause lateral winging. The diagnosis of serratus anterior palsy is easy to make via visualization of the scapula, and the winging can be accentuated by asking the patient is to push against a wall. Treatment is generally conservative, with pain reduction, activity modification, and physical therapy being the mainstays. Twenty-five percent of patients fail conservative treatment and are candidates for surgical reconstruction.
Snapping Scapula Syndrome (Scapulothoracic Crepitus)[6]
In this syndrome, disruption of the gliding motion of the anterior scapula along the posterior thoracic cage (the scapulothoracic joint) leads to audible and painful crepitus with motion of the scapula. Repetitive use, trauma, osteophyte formation, and bursitis have been suggested as possible etiologies of this syndrome. Conservative treatment is the first option in the majority of cases with successful results. This treatment includes the use of physical therapy to increase the space between the chest wall and scapula, as well as corticosteroid injection or NSAIDs for pain management. Surgical treatment is reserved for refractory cases and involves resecting any lesions in the scapulothoracic joint.
Scapulothoracic Dissociation[7]
The scapulothoracic joint is disrupted by traumatic injury, leading to lateral displacement of the scapula and damage to nerves and blood vessels. Loss of limb and life are potential outcomes of this injury depending on the extent of neurologic and arterial damage. On exam, swelling of the shoulder, numbness, weakness, and pulselessness in the upper extremity may be present. Radiographs should be taken to determine if there is a fracture of the clavicle or scapula, or if there is detachment in the acromioclavicular or sternoclavicular joints. Surgery is indicated when there is active arterial bleeding, or the limb is at risk of becoming ischemic. Surgery is also required to repair fractures and joint detachments.
Facioscapulohumeral Muscular Dystrophy[8][9]
This condition is an autosomal dominant muscular dystrophy that affects muscles of the face, humerus, and scapula before moving to the muscles of the trunk and lower extremities. Slowly progressive physical therapy is used to strengthen the muscles while attempting to avoid causing more damage to them. Surgery to stabilize the scapula against the thoracic cage has been shown to improve shoulder function in these patients.
Impingement[10]
Rotator cuff tendonitis/impingement presents with pain during overhead activities and results from the tendon of the supraspinatus muscle being pinched down by the acromion in most cases. This condition can cause inflammation around the tendon and in the fluid-filled bursae surrounding it.