Definition/Introduction
Prism glasses are lenses which deflect light and therefore, can correct some ophthalmic conditions most notably ocular misalignment.

Prism glasses are lenses which deflect light and therefore, can correct some ophthalmic conditions most notably ocular misalignment.
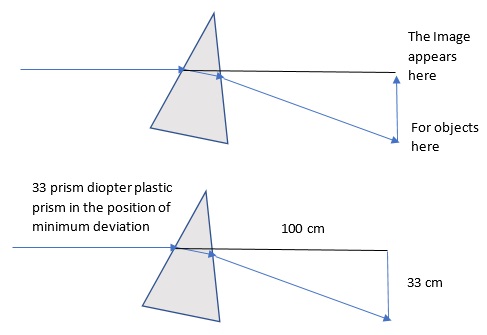
In optics, a prism is a device that uses refraction to change the direction of light. In nearly all applications, the refractive index of a prism (e.g. 1.49 for plastic) is higher than that of the medium it exists in (e.g. 1.00 for air). Therefore Snell’s law of refraction dictates that the light is bent toward the base of the prism. This light deflection is the sum of the deflection at both interfaces, or sides, of the prism. The more light is bent, the more power a prism is said to have. Prism power is measured in prism diopter which is defined as the amount of light deflection in cm at a distance of 100 cm. For example, since a 45-degree angle is formed when light is deflected 100 cm away over a distance of 100 cm, 100 prism diopters correspond to 45 degrees.[1]
The amount of deflection depends on both the refractive index of the material and the position the prism is held in. With a higher refractive index, glass prisms deflect light more than plastic prisms and are more prone to error.[2] The position of minimum deviation is such that the angle of light incident on the prism equals the angle of light exiting the prism. Rotating a prism in either direction from this position increases its effective power.[3]
Since prism power is due to refraction, the frequency of the light influences the amount of deflection from a prism. Higher frequency blue light gets refracted more than lower frequency red light; therefore, a prism will bend blue light more than red light. This fact can be exploited to allow for white light to be separated into its constituent colors by a prism.
In ophthalmology, prisms are used to measure the misalignment of the eyes, to induce misalignment to facilitate various tests and to treat misalignment. To treat misalignment, one must first measure the misalignment. This is done by holding prisms in front of one or both eyes until the eyes are aligned.
Complicating the discussion of prism power is the fact that glass and plastic prisms are calibrated for use in different positions. Plastic prisms are calibrated to be used in the position of minimum deviation. Glass prisms are calibrated such that the posterior surface is held perpendicular to the visual axis; this is known as the Prentice position. Finally, plastic prism bars are calibrated to be held perpendicular to the face; this is known as frontal plane position. In practice, the difference between the frontal plane and the position of minimum deviation is minimal. Because the position of the prism is crucial, one should not hold two prisms over the same eye in the same direction as the second prism will be out of position. Instead, the prisms can be split over each eye.
The position of least deviation is the most forgiving position. Since a prism mistakenly held outside the position of minimum deviation will have more effective power, any errors in holding a plastic prism results in falsely low measurements. Meanwhile, an error in holding a glass prism in Prentice Position could result in falsely high or falsely lower readings depending on which way the prism was out of position. Glass prisms are less frequently used.
Spherocylindrical lenses such as glasses and bifocals have prismatic power when looking outside the optical center. When observing a high myope, the side of their face can often appear shifted and directly behind their lens to an observer. This is an important consideration in diplopia induced by bifocals, especially in cases of anisometropia. In such cases of anisometropia, the prism can be added or removed from a portion of the lens to cancel out the prismatic power of looking outside the optical center. This is referred to as slab off or reverse slab off.
Glasses with prism power are often used to treat misalignment, convergence insufficiency, nystagmus, and (with the use of a prism in only the periphery) hemianopia[4]. A practitioner can measure the misalignment and treat it with a prism. Given the cost of glasses, often a trial with a series of parallel press-on prisms known as Fresnel prisms is advised. These prisms allow a patient to determine if symptoms are improved. Given the optical imperfections of the Fresnel press on prisms, there tends to be reduced image quality, and patients should receive a warning regarding this fact.
Prismatic power can be ground into a new pair of glasses for superior image quality. Prism should be written in prism diopters along an axis with the direction of the base specified. For example, to correct a five prism diopter hypertropia, one would write for five prism diopters of the base down prism over the hyperopic eye. Since alignment is a binocular issue, the prism can also be split and placed in front of each eye. Once the required prism is over ten diopters, referral to a strabismus surgeon should be a consideration.
Prisms can make convergence more or less difficult. Given that a myope with spectacle correction has inherent base-in prism when converging, myopic spectacles lessen the demands of convergence. In contrast, a hyperope would experience more difficulty with convergence due to spectacle use. In the case of convergence insufficiency, base in prisms can make convergence easier or base out prisms can be used to strengthen the muscles of convergence. Although theoretically sound, the practical use of the base in prisms for convergence insufficiency is no more effective than placebo.[5] Optical decentration can also be used to obtain a prism effect.
Finally, in nystagmus, there often exists a point of minimization of the nystagmus called the null point, which often results in patients adopting a head turn. If the null point is in eccentric gaze, prisms can be used to shift the null point to a primary gaze to allow for a lessened head turn. However, the amount of prism necessary is often too high for this to be practically useful. This same limitation is also a problem is using prisms to shift the visual field in homonymous hemianopia or hemispatial neglect.
While there exist many other uses of the prism in non-ophthalmic applications, the relevance to ophthalmology is our focus here. In summary, the proper use of prisms in ophthalmology can facilitate diagnosis and treatment.
Irsch K. Optical Issues in Measuring Strabismus. Middle East African journal of ophthalmology. 2015 Jul-Sep:22(3):265-70. doi: 10.4103/0974-9233.159691. Epub [PubMed PMID: 26180462]
Freedman K, Ray C, Kirk D. Reevaluation of Current Prism Standards With Recommendations to Increase Accuracy in the Measurement of Strabismus. American journal of ophthalmology. 2019 Feb:198():130-135. doi: 10.1016/j.ajo.2018.09.009. Epub 2018 Sep 19 [PubMed PMID: 30240722]
Thompson JT, Guyton DL. Ophthalmic prisms. Measurement errors and how to minimize them. Ophthalmology. 1983 Mar:90(3):204-10 [PubMed PMID: 6866442]
Bowers AR, Keeney K, Peli E. Randomized crossover clinical trial of real and sham peripheral prism glasses for hemianopia. JAMA ophthalmology. 2014 Feb:132(2):214-22. doi: 10.1001/jamaophthalmol.2013.5636. Epub [PubMed PMID: 24201760]
Level 1 (high-level) evidenceScheiman M, Cotter S, Rouse M, Mitchell GL, Kulp M, Cooper J, Borsting E, Convergence Insufficiency Treatment Trial Study Group. Randomised clinical trial of the effectiveness of base-in prism reading glasses versus placebo reading glasses for symptomatic convergence insufficiency in children. The British journal of ophthalmology. 2005 Oct:89(10):1318-23 [PubMed PMID: 16170124]
Level 1 (high-level) evidence