Introduction
The pons is the portion of the brainstem between the midbrain above and the medulla oblongata below. The transverse section of pons subdivides into two areas: the ventral and the dorsal. The ventral portion of pons contains pontine nuclei, vertically traversing corticopontine and corticospinal tracts, and transversely crossing fibers arising from pontine nuclei that project to the opposite cerebellum through the middle cerebellar peduncle. The ventral segment of the pons is bulky due to pontine nuclei and their connection, corticopontocerebellar.
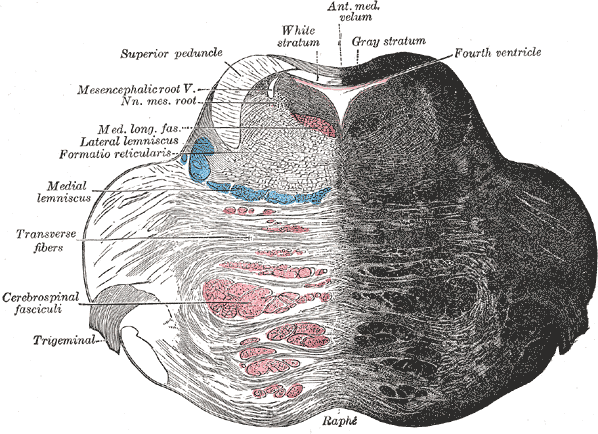
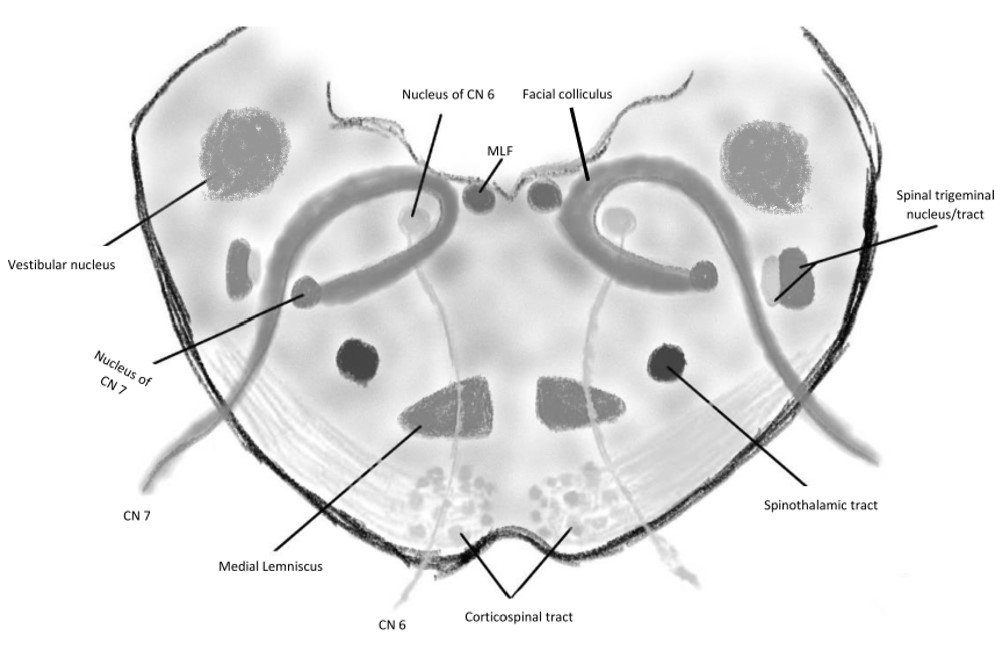
The dorsal part of the pons, also known as the tegmentum, is occupied mainly by the reticular formation. The tegmentum is bounded laterally and superiorly by the inferior cerebellar peduncle in the superior cerebellar peduncle. Internal structures of the pons are usually described along with anatomical landmarks; structures at upper pons are mainly superior cerebellar peduncles, medial longitudinal fasciculus, locus coeruleus, pedunculopontine tegmental nucleus, and parabrachial nucleus. The transverse section at the middle cerebellar peduncle shows the trapezoid body, medial lemniscus, lateral lemniscus, and trigeminal nucleus (both sensory and main motor). Pontine structures at the level of the facial nucleus are the abducens nerve nucleus, facial nerve nucleus, and vestibular nuclei.
Structure and Function
External features
The pons has an approximate height of about 27 mm, transverse and anteroposterior width of 38 mm and 25 mm, respectively. Anteriorly it is limited by pontomesencephalic sulcus and pontomedullary sulcus below. Whereas its posterior surface is limited superiorly by an imaginary line running immediately below the inferior colliculi and inferiorly by an imaginary line crossing the lateral angles of the fourth ventricle.[1][2]
Surfaces
The anterior surface rests on the anterior part of the clivus and is mostly convex that continues with the middle cerebellar peduncle bilaterally. The basilar groove for the basilar artery runs along its midline of the anterior pons, and the pyramidal tracts course through either side of the basilar groove. Trigeminal nerve roots emerge from the ventral pons by a larger sensory root and smaller motor root. The posterior surface forms the cranial portion of the rhomboid fossa and is covered posteriorly by the cerebellum. Critical anatomical landmarks in the dorsal pons include medial eminence, facial colliculus, and stria medullaris.
The medial eminence denotes the midline of the floor. The facial colliculus is an elevated area formed by the axons from the facial motor nucleus (cranial nerve VII) looping around the abducens nucleus (cranial nerve VI). The stria medullaris is transversely crossing a bundle of nerve fibers that distinct pons from medulla oblongata posteriorly. It is a part of the epithalamus that contains afferent fibers projecting to the habenula from septal nuclei, anterior thalamic nuclei, and lateral preoptic-hypothalamic region.[3]
Internal Morphology
Morphologically and physiologically, the pons subdivides into two segments: the anterior basilar pons and the posterior tegmentum. A bundle of transverse myelinated fibers, also known as the trapezoid body, is situated between these two segments. The base or crus of the pons is the extension of the middle cerebral peduncles and continues caudally as the pyramid of the medulla oblongata. Internal structures of the base of pons include longitudinal bundles of corticospinal tracts, transverse fibers of pontocerebellar tracts and acoustic pathway, and by the pontine nuclei, adjacent to the other fibers. Among the two transverse fibers, axons of acoustic pathways arise from the cochlear nuclei and cross contralateral side constituting the trapezoid body.
Pontocerebellar fibers arise from the pontine nuclei and project into the cerebellum through the middle cerebellar peduncles. They divide into three layers 1) the superficial layer that rests anteriorly to the pyramidal tract and pontine nuclei; 2) the intermediate layer separating the bundles of the pyramidal tract and the deep layer 3) the deep layer that courses ventral to the medial lemniscus.
The longitudinal fibers within the pons are mainly corticospinal, corticonuclear, and cortico-pontine tracts. The corticospinal tract courses through the base of the pons, as several separated bundles and not as a compact structure observed in the pyramids of the medulla. The corticonuclear tract represents cortical axons projecting to the facial, trigeminal, and abducens nerve nuclei. Finally, the corticopontine fibers connect the cerebral cortex and the pontine nuclei. The dorsal portion of the pons is called the tegmentum, a similar structure in the medulla oblongata and midbrain. The reticular formation, descending and transverse fibers, cranial nerve nuclei are the main constituents of the tegmentum of pons.[4][5]
Gray Matter
The gray matter of pons can be homologous to the spinal cord, such as cranial nerve nuclei, or the gray matter of its own. Pontine gray matter includes pontine nuclei, the gray matter of reticular formation, the superior olivary nucleus, trapezoid body nucleus, and nucleus of the lateral lemniscus. The superior salivary nucleus is a part of the parasympathetic nervous system that provides parasympathetic innervation to sublingual and submandibular glands. The lacrimal nucleus, also located within the pons and considered as a part of the superior olivary nucleus, provides parasympathetic supply to the nasal, lacrimal, and palatine glands.
The nuclei of cranial nerves are homologous to the gray matter of the spinal cord. Motor nuclei represent the anterior horn, while sensory nuclei represent the posterior horn. The facial and trigeminal nuclei are mixed, having both sensory and motor components. The motor nucleus of the facial nerve is located almost at the pontomedullary junction, dorsal the trapezoid body, and approximately 4 mm away from the fourth ventricular floor. It innervates the muscles of the facial expression, and injury to this nucleus manifests as a lower motor neuron type of facial paralysis.
The fibers of the motor nucleus form the inner genu and facial colliculus on the rhomboid fossa while encircling the abducens nucleus. Whereas the sensory root of the facial nerve is also called the intermediate nerve, carries the taste sensation from the ventral two-thirds of the tongue and terminates at the solitary tract nucleus. The abducens nerve nucleus is purely motor located deep to the facial colliculus. It provides motor innervation to the lateral rectus of the eyeball, and the lesson to it manifests as ipsilateral paralysis of eye abduction.[6]
Trigeminal nerve nuclei located in the pons include the sensory nucleus, mesencephalic nucleus, and main motor nucleus. The sensory nucleus, mesencephalic tract nucleus, and motor nucleus of the trigeminal nerve are situated at the pons. The main sensory nucleus is the cranial continuation of the trigeminal nerve's spinal nucleus and is located lateral to the main motor nucleus. It receives afferent axons conveying tactile and pressure sensations from the scalp, dura, face, oral cavity, and nasal cavity. Cranial extension of the main sensory nucleus toward the midbrain is called the mesencephalic nucleus. It receives proprioception from extraocular muscles, muscles of mastication, joints, teeth, and the periodontium and is responsible for monosynaptic jaw jerk reflex.
The spinal nucleus of the trigeminal nerve corresponds to the dorsal horn of the spinal cord. Afferents of trigeminal ganglion carrying pain and temperature sensations from the face enter in the rostral pons, then synapse on the spinal nucleus after descending along the spinal tract of the trigeminal nerve. This spinal tract of the trigeminal nerve is lateral to the spinal nucleus, extending from the fifth cranial nerve's entry to the upper cervical cord (C2). The main motor nucleus of the trigeminal nerve is located medially to the main sensory nucleus and adjacent to the point of trigeminal nerve fibers attachment. It provides motor supply to the muscles of mastication.
The tegmentum of the pons harbors the ventral and dorsal cochlear nuclei. The dorsal nucleus forms an elevation called the acoustic tubercle at the lateral angle of the rhomboid fossa, and its axons are recognizable as acoustic striae. The axons of the ventral nucleus undergo a horizontal course and decussate to form the trapezoid body, then ascend as the lateral lemniscus around the superior olivary nucleus. These cochlear nuclei and their corresponding axons aid the hearing process by receiving afferents from the organ of Corti. Four vestibular nuclei named superior, inferior, medial, and lateral are located in the vestibular area of the rhomboid fossa and receive afferent vestibular nerve fibers from semicircular ducts, utricle, and saccule of the inner ear. A lesson to these nuclei causes postural instability, vertigo, and nystagmus.
White Matter
For description purposes, nerve fibers within the pons group together as transverse and longitudinal fibers. The transverse fibers comprise the fibers of the cochlear nucleus and pontocerebellar tracts. Whereas longitudinal fibers subgrouped as ascending, descending, and associative fibers. The ascending fibers include the medial, lateral, spinal, and trigeminal lemnisci and the superior cerebellar peduncle. The medial lemniscus is located posterior to the pyramidal tract and near to the raphe. It forms by sensory fibers from the gracile and cuneate nuclei projecting to the thalamus. It carries the spinal cord's dorsal column sensation (conscious proprioception, discriminative touch, vibratory sensation). The lateral lemniscus forms from fibers of the trapezoid body that ascend toward the inferior colliculus. This lateral lemniscus is part of the acoustic pathway and is located lateral to the spinothalamic tract in the ventral portion of the tegmentum.
The spinal lemniscus is a combined form of anterior and lateral spinothalamic tracts. It ascends along the ventral tegmentum, in between the lateral and medial lemniscus, and carries pain and temperature sensation from the contralateral side of the body. The trigeminal lemniscus carries the fibers from the spinal and main sensory trigeminal nucleus and relays on the ventral posteromedial nucleus (VPM) of the thalamus. The superior cerebellar peduncle principally carries efferents of the cerebellum, including the dentatorubral tract, projecting from the dentate nucleus to the contralateral red nucleus at the midbrain.
Embryology
During the third week of gestation, the formation of the nervous system begins with the development of the neural plate from a thickening of the ectoderm. The formation of two neural folds gives rise to a longitudinal neural groove along the midline of the neural plate. Subsequent midline fusion of the neural folds converts the grooved neural plate into the neural tube having two openings, anterior and posterior neuropores. This process is called neurulation that proceeds in both directions, cranial and caudal.
Neurulation occurs simultaneously with the dissociation of the neuroectoderm from the overlying surface ectoderm, a process termed as disjunction. Anterior and posterior neuropores close between gestational days 23 to 25 and 25 to 27, respectively. The brain and spinal cord are derived from the wall of the neural tube, whereas the lumen forms the ventricular system and central canal.
During the fourth week, three primary brain vesicles form in the rostral neural tube named, the forebrain vesicle or prosencephalon, the midbrain vesicle or mesencephalon, and the hindbrain vesicle or rhombencephalon. During the fifth week, the forebrain splits into the telencephalon and diencephalon, the hindbrain into the metencephalon and the myelencephalon, and the midbrain becomes the mesencephalon. Thus, five secondary brain vesicles form. As the three primary vesicles develop, the brain bends forward to form the cephalic and the cervical flexure in the midbrain region and at the hindbrain spinal cord junction, respectively.
Later, a compensatory pontine flexure forms between the cervical and cephalic flexure. The pontine flexure divides the hindbrain into the metencephalon (future pons and cerebellum) and the myelencephalon (future medulla). The dorsal portion of the metencephalon gives rise to the cerebellum, whereas the ventral part becomes the pons. The pontine nuclei, those project axons to the contralateral cerebellar cortex, lie in the ventral pons, whereas the cranial nerve nuclei are located in the dorsal pons. Motor nuclei of cranial nerves derive from the basal plate, and sensory nuclei are from the alar plate.
The central hindbrain cavity becomes the fourth ventricle. Consequently, the fourth ventricle expands and spreads its lateral walls like the pages of a book. As a result, the dorsal wall or roof plate of the fourth ventricle, covered by pia mater, is stretched and thinned. The roof plate with its vascular pia mater forms the tela choroidea that invaginates into the fourth ventricular cavity to form choroid plexus. Another result of the spreading of lateral walls of the fourth ventricle is the alar plates granted the lateral position in relation to basal plates.[7][8]
Blood Supply and Lymphatics
Three groups of arteries from posterior circulation provide blood supply to the pons: anteromedial, lateral, and dorsal. The anteromedial group of arteries originates from the terminal branches of the vertebral artery and the basilar artery that nourish the paramedian ventral pons (including the corticospinal tract fibers), bilateral medial longitudinal fasciculus (MLF), medial lemniscus, and abducens nucleus.
The lateral group of arteries derives mainly from the superior cerebellar artery, anterior inferior cerebellar artery, and long pontine arteries. Perforating branches of lateral group arteries nourish the superior cerebellar peduncle, motor and main sensory trigeminal nuclei, central tegmental tract, superior olivary nucleus, pontine reticular nucleus, abducens nerve nucleus, facial nerve nucleus, and locus ceruleus. Terminal superior cerebellar arteries provide the arterial supply of the dorsal pons that perfuse the superior cerebellar peduncle, the mesencephalic nucleus of the CN V, and the locus ceruleus.[7][9]
Surgical Considerations
Most pontine tumors are diffuse; as such, chemotherapy/radiotherapy frequently preferred over resection surgery. However, patients with focal, low-grade tumors are the best candidate for surgery. The pons is identified superiorly by pontomesencephalic and inferiorly by a pontomedullary sulcus, and divided into ventral and dorsal, or anterior and posterior at the level of the medial lemniscus. The pyramidal tract within the pons is more medial and ventral compared in the midbrain, as well as the CN V, CN VI, CN VII, and CN III nerves and their nuclei.
The facial nerve courses around the abducens nerve nucleus within the pons, and must be very well established anatomical relation when lessons are approached through the rhomboid fossa. The choice of route for neurosurgical access to the pons is primarily determined by the specific location of the pontine lesson. Anterior and upper pontine lessons are accessible through an orbito-fronto-zygomatic route, which a modified form of the supraorbital craniotomy.
For the orbito-fronto-zygomatic route, the oculomotor nerve (CN III) is considered a key reference point. Dissection of interpeduncular and prepontine cisterns with the durotomy of the tentorium is necessary to expose the upper pons, and this entry point is also known as supra-trigeminal. In the anterior approach, the region around the emergence of the trigeminal nerve is a safe area to be accessed 1 cm wide at 1 cm from the midline, but should not extend too anterior to avoid the corticospinal tract.
The sigmoid approach can be useful for lesions in the anterior, inferior, or ventrolateral portions of the pons reached via paramedian occipital or petrosal route. However, due to the very narrow corridor, this approach is only suitable for biopsy or resecting cavernomas therein. To access a longitudinal incision is made between the points of emergence of the CN V and CN VII. Lesions in the dorsal pons are accessed through the rhomboid fossa.
A telovelar route, in other words, the cerebellomedullary fissure approach, is used to access superior and posterior dorsal pontine lesions. The suprafacial triangle is a safe entry triangle, defined caudally by the facial nerve (facial colliculus is the reference), medially by the median sulcus (medial longitudinal fasciculus), and laterally by the superior cerebellar peduncles.
However, bipolar stimulation on the surface to localize facial nerve course is recommended, to avoid injury, and entry must always be 2 mm away from the midline to preserve the MLF (medial longitudinal fasciculus). The infracollicular route accesses posterior and inferior lesions via the infrafacial triangle, that bordered medially by the MLF (medial longitudinal fasciculus), laterally by the facial nerve, and caudally by the medullary striae. Intraoperative monitoring is mandatory for this route.[9][10][11]
Clinical Significance
Pons is a potential anatomical site for tumor, infarction, and demyelinating disorders and commonly manifested and cranial nerves and tract dysfunction. A stroke affecting the pons results from a large-vessel stroke small-vessel disease within the posterior circulation, composed of the paired vertebral arteries, basilar artery, and paired posterior cerebral arteries (PCAs). At the level pontomedullary junction, vertebral arteries unite to the basilar artery, split into two PCAs in the interpeduncular fossa. In 75% of instances, PCAs arise from the basilar artery; in 20%, one PCA originates ipsilaterally from the internal carotid artery (ICA) via the posterior communicating artery; and in 5%, both arise from the respective internal carotid arteries.[12]
The common causes of posterior circulation ischemia affecting pons, as well as brainstem infarctions, are following:[13][14]
- In situ thrombosis from atherosclerosis plaque rupture (most common cause)
- Embolism: thromboembolism from the cardiac chambers or large arteries proximal to the posterior circulation of the brain
- Vasculitis: Takayasu arteritis, giant cell arteritis
- Hypercoagulability: Inherited or acquired form of hypercoagulability including factor V Leiden, protein C, S, and anti-thrombin-III deficiency, polycythemia, cryoglobulinemia, Waldenstrom macroglobulinemia
- Vertebral artery dissection. Extracranial and intracranial either segments of vertebral arteries are frequently affected by dissection, thus resulting in the posterior circulation, including brainstem ischemia
Several syndromes describe the specific anatomical lesson of the pons that can result from tumors or infarction.[15][16]
1. Medial superior pontine syndrome: occurs secondary to compressing tumor to the upper and medial portion of the pons or stoke affecting paramedian branches of the upper basilar artery. Clinical findings are the following:
- Ipsilateral to the lesion: ataxia (probably) due to superior and/or middle cerebellar peduncle involvement, internuclear ophthalmoplegia due to the lesson of medial longitudinal fasciculus
- Contralateral to the lesion: Paralysis of face, arm, and leg from corticobulbar and corticospinal tract lesson Rarely touch, vibration, and position are affected due to loss of medial lemniscus function
2. Lateral superior pontine syndrome or syndrome of the superior cerebellar artery:
- Ipsilaterally: ataxia of limbs and gait. Dizziness, nausea, vomiting, horizontal nystagmus due to vestibular nucleus dysfunction, paresis of conjugate gaze or pontine contralateral gaze, Horner syndrome) due to the descending sympathetic tract lessons
- Contralaterally: impaired pain and thermal sensation on the face, limbs, trunk from spinothalamic tract lesson. Touch, vibration, and position sense may also be impaired more prominently in the leg than the arm. There is a tendency to the incongruity of pain and touch due to the lesson to the lateral portion of the medial lemniscus.
3. Medial mid-pontine syndrome due to the paramedian branch of the mid-basilar artery stroke:
- Ipsilaterally: ataxia due to pontine nuclei lesson
- Contralaterally: face, arm, leg paralysis, and variable loss of touch and proprioception in the cases where the lesion extends posteriorly
4. Lateral mid-pontine syndrome (short circumferential artery):
- Ipsilateral to the lesion, ataxia of limbs due to the middle cerebellar peduncle involvement. Paralysis of muscles of mastication resulting from the lesson to the Motor fibers or nucleus of the trigeminal nerve. Diminished sensation over the side of the face due to the lesion of sensory fibers or the nucleus of the trigeminal nerve.
- Contralateral to the lesion: Impaired pain and temperature sensation on limbs and trunk due to the spinothalamic tract lesson.
5. Medial inferior pontine syndrome, secondary to occlusion of a paramedian branch of the basilar artery:
- Ipsilaterally: paralysis of conjugate gaze to the affecting side (preservation of convergence), nystagmus: ataxia of limbs and gait, diplopia due to abducens nerve lesson.
- Contralaterally: presents with face, arm, and leg paralysis, impaired tactile and proprioceptive sensation over one-half of the body due to lesson to the medial lemniscus.
6. Lateral inferior pontine syndrome from occlusion of the anterior inferior cerebellar artery:
- Ipsilaterally: vertigo, nausea, vomiting, horizontal and vertical nystagmus, oscillopsia, facial paralysis (seventh nerve), paralysis of conjugate gaze to the affecting side (preservation of convergence), deafness, tinnitus (cochlear nucleus), ataxia, impaired sensation over face (descending tract and nucleus of the trigeminal nerve.
- Contralateral to the lesion: impaired pain, thermal sensation over one-half the body (spinothalamic tract).