Introduction
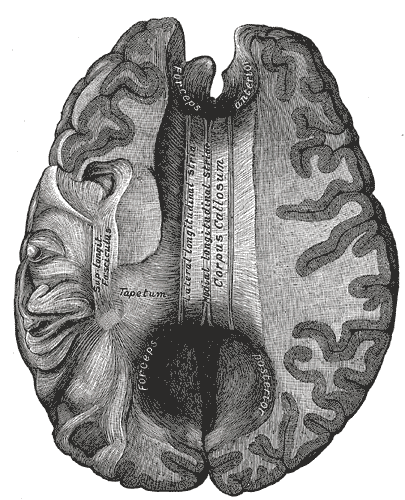
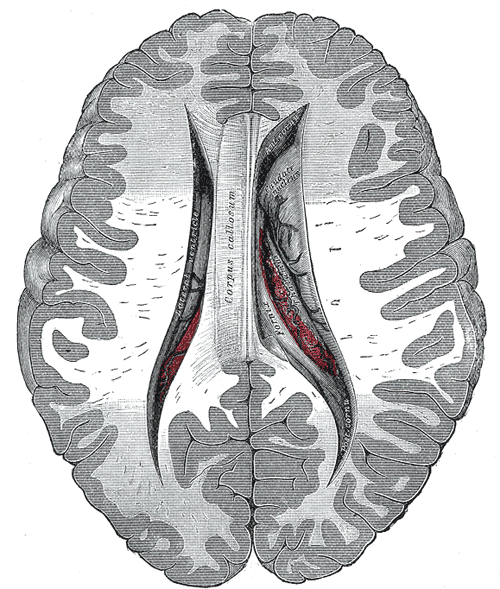
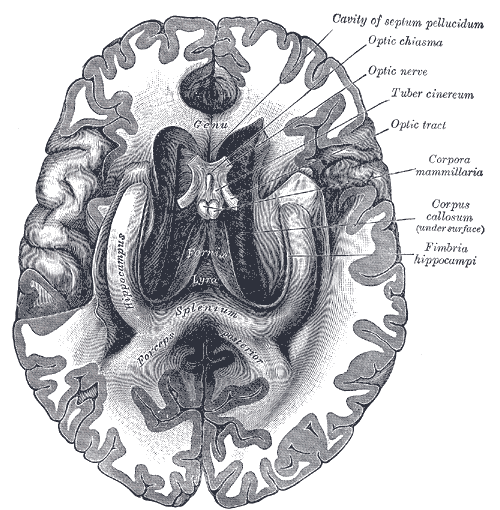
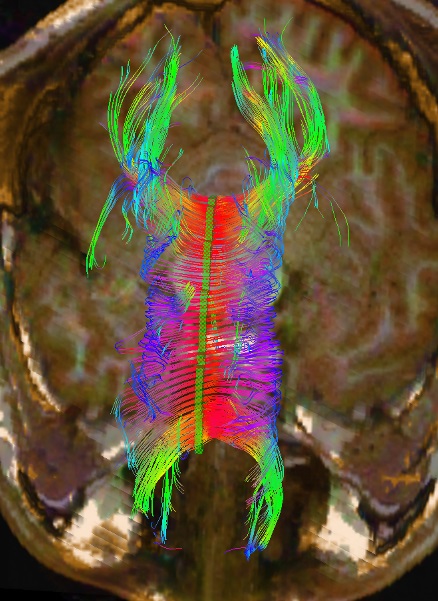
The corpus callosum is the primary commissural region of the brain consisting of white matter tracts that connect the left and right cerebral hemispheres. It is composed of approximately 200 million heavily myelinated nerve fibers that form homotopic or heterotopic projections to contralateral neurons in the same anatomical layer.[1] During infancy, the corpus callosum expands rapidly due to an increase in the number of axons, axon diameter, and myelin. Although the development of the corpus callosum is complete by age four, growth continues until the third decade of life at a much slower rate.[1] Anatomically from anterior to posterior, the corpus callosum is composed of four parts based on previous histological findings: the rostrum, genu, body, and splenium, each responsible for connecting distinct areas of the cortex. The isthmus refers to the narrow region between the body and splenium in the posterior aspect of the corpus callosum.[2] Fibers of the genu cross over and give rise to the forceps minor, a connection between regions of the frontal cortices.[2] The fibers of the splenium move posteriorly and contribute to the forceps major, providing a connection between the occipital lobes.[3] The body fibers form the corona radiata as well as other large white matter pathways as they move transversely through the cerebral cortex. Finally, the orbital regions of the frontal lobes connect via the rostral fibers.[3] Due to its anatomical location, the corpus callosum is strongly related to the fornix and lateral ventricles. In conjunction with the fornix, the corpus callosum forms a physical barrier to separate the two lateral ventricles.[3]