Continuing Education Activity
Bullous myringitis (BM) is a relatively common infectious condition characterized by bullae or vesicles on the tympanic membrane without affecting the contents of the external or middle ear. This activity reviews the evaluation and management of bullous myringitis, highlights the need for early recognition and prompt treatment by the interprofessional team to prevent complications and facilitate early resolution.
Objectives:
- Identify the etiology and epidemiology of bullous myringitis.
- Review the appropriate history, physical, and evaluation of bullous myringitis.
- Outline the treatment and management options available for bullous myringitis.
- Describe some interprofessional team strategies for improving care coordination and communication for bullous myringitis and improve outcomes.
Introduction
Bullous myringitis (BM) is a relatively common infectious condition characterized by bullae or vesicles on the tympanic membrane (TM), without affecting the contents of the external or middle ear.[1] If the middle ear becomes involved, this would be consistent with acute otitis media (AOM) and not merely bullous myringitis. As the tympanic membrane is well innervated, moderate to severe pain is a common expected manifestation. Physical findings may be similar to those of acute otitis media, including erythema and thickening of the tympanic membrane, attenuated or absent light reflex, and decrease membrane mobility. Bloody otorrhea can occur when a bulla ruptures and is referred to as bullous hemorrhagic myringitis. The rupturing of bulla often results in a concomitant reduction of pain.
The current thinking is that bullous myringitis is caused predominantly by viruses, although one study insinuated mycoplasma pneumoniae, which was not substantiated by subsequent studies.[2][3][4]
Etiology
Bullous myringitis is thought to be caused predominantly by viruses, although Streptococcus pneumoniae is the most commonly identified bacteria.[2] Other bacterial pathogens include Haemophilus influenzae, Moraxella catarrhalis, Group A Streptococcus, Staphylococcus aureus.[5][1] Viral etiologies include Respiratory Syncytial Virus (RSV) or influenza viruses predominately. In cases of recurrent otitis media, there can be involvement of multiple bacterial pathogens or coinfection with both a bacterial and viral pathogen. Other, rarer, organisms identified include varicella, Epstein-Barr virus, measles, mycoplasma, and fungi.[6] Bullous myringitis may also occur after chemical irritation of the middle ear space in an otherwise intact tympanic membrane can produce BM with acute otitis media.[7] Streptococcus pneumoniae has a relatively higher prevalence in cases with bullous myringitis compared to AOM.
Epidemiology
The peak incidence of bullous myringitis is found to be in the winter months and is thought to be the result of poor Eustachian tube function in cold climate.[4][5] In older children and the adolescent population, bullous myringitis appears to be more common among women.[8] However, AOM and bullous myringitis are more common in male young children. Most cases of bullous myringitis occur in males between the ages of 2 to 8 years old, whereas AOM is most commonly seen in children less than two years of age.[4][5][9] One study found the rate of bullous myringitis among those less than 2-year-old to be 5.7% of patients with AOM, accounting for one bullous myringitis case for every 20 AOM cases.[4][5] In 2017, the estimate was that 5 million US children are affected by AOM annually, which in turn correlates with approximately 400,000 annual bullous myringitis cases nationally each year.[10] Up to 16% percent of patients can present with bilateral bullous myringitis. The risk of recurrent AOM in patients with bullous myringitis is up to three times greater than in AOM without bullous myringitis.[4][5]
Pathophysiology
Bullous myringitis shares similar pathophysiology with AOM and although some aspects remain unclear. Inflammation of the tympanic membrane can occur as a direct result of trauma such as a foreign body, accidental trauma while cleaning the ear canal, sudden loud noises, changes in airline cabin pressure, and even an inflicted blow to the ear. Bullous myringitis can also occur as a result of viral or bacterial infections affecting the tympanic membrane as part of a respiratory infection or through the spread of fungal infection from the adjacent epidermis. Once inflamed, the enlarging bullae and inflamed tympanic membrane can cause severe pain until the blister ruptures, which can result in bloody ear discharge.
History and Physical
The most common symptom of bullous myringitis is acute ear pain.[11] This pain is often sudden in onset, sharp or throbbing, with or without radiation, and is often more severe than described in children with AOM.[4][5] If radiation is present, it will most often be to the mastoid process, occiput, temporomandibular joint, and rarely to the face.[4][5] Young children of less than two years that cannot articulate pain may manifest other symptoms such as rubbing of the ear(s), restless sleeping, excessive crying, and poor feeding. These manifestations often accompany upper respiratory tract symptoms, notably rhinitis (93%), and cough (73%). The specific bacterial pathogen type does not appear to alter symptom presentation.[4][5]
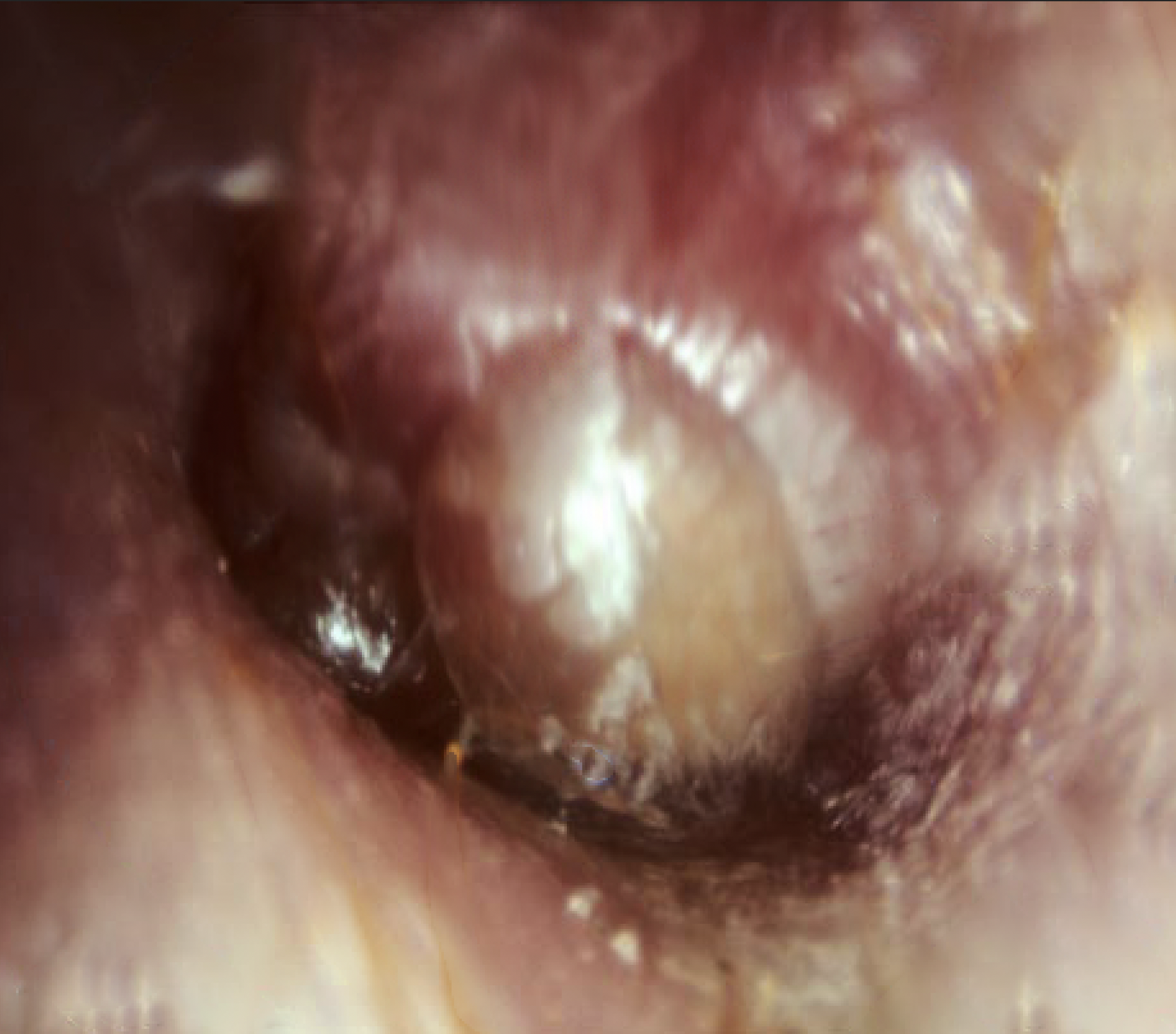
The classic sign of bullous myringitis is the presence of blisters (bullae) on the tympanic membrane, often accompanied by fever, thickening, and erythematous appearance of the tympanic membrane, decreased or absent light reflex, and decreased mobility. In true bullous myringitis, the bullae are confined to the tympanic membrane. If bullae or vesicles are seen in the ear canal or external ear, other diagnoses should be considered such as Ramsay-Hunt syndromw or any of the bullous dermatidities. Conductive hearing loss may occur in the presence of effusion. Over half of the patients with bullous myringitis demonstrate sensorineural hearing changes. However, the mechanism of this is poorly understood.[11] Overall, earache and fever are more common in bullous myringitis than in AOM.[4][5]
Diagnosis is clinical, with its basis on the presence of one or more blisters on the tympanic membrane, irrespective of other findings such as AOM.[4][5] No lab tests or imaging are necessary for the diagnosis of bullous myringitis. Tympanocentesis can be used in selected cases to confirm middle ear effusion and to culture for the offending pathogen. Aspiration of teh bulla may also provide pain relief. Otoscopic visualization forms the basis of the diagnosis, but other studies are available for the practitioner, such as a pneumatic otoscope, tympanometry, and acoustic reflectometry, though these are rarely indicated in isolated bullous myringitis.
Evaluation
The basis for the diagnosis of bullous myringitis is on physical examination via an otoscope
Laboratory Studies
Laboratory evaluation is rarely necessary for the diagnosis of bullous myringitis. The occasions that would lead to further laboratory evaluations would consist of infants less than 28 days of age with a fever and acute bullous myringitis. This scenario will involve full sepsis work up per the American Academy of Pediatrics guidelines to confirm or exclude other systemic or congenital diseases.
Imaging Studies
Imaging studies are not a routine recommendation unless there are concerns for intertemporal or intracranial complications such as mastoiditis, epidural or brain abscess, meningitis, or cholesteatoma. CT or MRI may be of assistance.
Tympanocentesis
Tympanocentesis is rarely indicated but can be of assistance in neonates or toxic appearing children who require culturing due to a higher risk of adverse outcomes, and to provide pain relief.
Treatment / Management
The treatment and prognosis of bullous myringitis are similar to AOM without bullae, with the exception being that pain management may require more aggressive treatment. Also, the more common “watch and wait” method of AOM may not be appropriate in BM cases, as these have a higher reoccurrence rate, and the majority of patients have a positive bacterial culture of their middle ear effusion.[12] As a result, systemic antibiotics and close outpatient follow-up are considered first-line treatment in BM. The American Academy of Pediatrics' (AAP) AOM guideline recommends amoxicillin (80 to 90 mg/kg/day) as the first-line drug provided there was no use of amoxicillin in the previous 30 days.[13] High dose amoxicillin is the recommended antimicrobial treatment as it reaches a high concentration in the middle ear. Among patients that had a recent course of amoxicillin (previous 30 days), amoxicillin-clavulanic acid is the therapy of choice. In penicillin-allergic patients, the AAP recommends a macrolide (azithromycin or clarithromycin) or, depending on the severity of the patient’s allergy, cefdinir, cefpodoxime, or cefuroxime. A case report using topical steroids, topical antibiotics, and systemic antibiotics showed good recovery with no hearing loss.[14] Ciorba speculated that adding systemic steroids to antibiotic therapy ould reduce the prevalence of hearing loss among bullous myringitis patients.[15] However, systemic steroids are not indicated in the management of bullous myringitis at present.
A recent review evaluating therapeutic options for myringitis found no well-designed randomized studies, although surgery showed better treatment results than topical agents and laser-assisted treatments.[16]
Due to the high occurrence of hearing loss in a patient diagnosed with bullous myringitis, recommendations include a pure tone audiogram in all patients diagnosed with bullous myringitis. This evaluation is key in identifying the specific type and quantity of hearing loss.[4][11][17] There is no strong evidence supporting the use of systemic steroids in the recovery of hearing loss.[11]
Myringotomy may be necessary in refractory cases or cases with impending complications.[11]
Differential Diagnosis
The differential diagnosis of bullous myringitis relies heavily on the clinician’s physical exam. Bullous myringitis, like AOM, needs to be distinguished from otitis media with effusion (OME) as well as from other bullous dermatologic conditions such as bullous pemphigoid and pemphigus vulgaris. Bullae must also be distinguished from vesicles, which would suggest a viral origin sich as Ramsay-Hunt syndrome. Other differential diagnoses include acute suppurative otitis media, otitis externa, granuloma, and acute mastoiditis.[18][19]
Prognosis
Bullous myringitis, like AOM without bullae, has a relatively good prognosis. Hearing loss and vestibular dysfunction are usually transient, and most recover after the infection has resolved.[11] The majority of patients (95%) experienced pain resolution by day three and otorrhea resolution by day 5. The resolution of middle ear effusion, however, can take up to 5 weeks.[4][5][11]
Complications
Complications arising from bullous myringitis are similar to AOM without bullae. The most common sequelae being hearing loss. More rare, but life-threatening, complications include subperiosteal abscess, labyrinthitis, facial paresis, mastoiditis, post-auricular cellulitis, epidural abscess, meningitis, and sigmoid sinus thrombosis. Among patient populations with adverse sequelae, multidrug-resistant Streptococcus pneumoniae has been isolated.[20][21]
Deterrence and Patient Education
Patients require education regarding the completion of their full course of antibiotics and the need to follow up with their primary care provider. Return precautions for worsening of their symptoms, despite appropriate pain management and antibiotic administration, are recommended.
Pearls and Other Issues
The biggest challenge is the timely recognition of this condition. Failure to do so results in great patient dissatisfaction as it is very painful.
Enhancing Healthcare Team Outcomes
Diagnosis and management of patients diagnosed with bullous myringitis require an interprofessional team of healthcare professionals that include a nurse, a pharmacist, and several physicians in different specialties. This approach is necessary to reduce both morbidity and mortality of bullous myringitis sequela. The moment there is a diagnosis of bullous myringitis, the provider needs to provide proper analgesia orders for the nurse to administer, as well as systemic antibiotics. There also may be a need for referral to otolaryngology for further evaluation and management, which includes auditory testing for the assessment of hearing loss.[11] [Level 1] Pharmacists can evaluate the appropriateness of antibiotic selection, verify dosing, and check for drug interactions, informing the clinician of any issues. Pharmacists should also counsel patients and their families about the importance of the completion of antibiotics and potential side effects. Nursing can also emphasize the importance of compliance, track treatment progress, answer patient questions, and keep the clinician staff up to date on progress or concerns. This interprofessional approach will yield the best patient results. [Level 5]