Introduction
Impression materials are used to copy the teeth and surrounding oral structures by creating a dental impression poured with dental plaster to fabricate a dental cast. This procedure provides a tridimensional and accurate mouth replica, allowing dental work even in the absence of the patient.
Dental models enable dentists to perform a better diagnosis and treatment planning since the teeth can be meticulously visualized and studied from angles that are difficult to see in the patient's mouth. Particular treatment, such as removable and fixed prostheses, can be executed thanks to dental casts. The final restoration or prosthesis fit depends on how accurately the impression material has recorded the tissue details.
Wax was the only impression material used in dentistry until the mid-19th century when gutta-percha first appeared. Then in 1857, Charles Stent created a thermoplastic modeling compound similar to today's impression compound. Still, the problem with this material was that it was rigid and could not reproduce undercut areas. All the impression materials used until that date became rigid after setting and could not copy the oral tissues accurately. Thus, there was always a need for an impression material that could remain elastic even after setting. That is when agar, a reversible hydrocolloid manufactured from algae, was introduced in dentistry. Although this jelly-like material was elastic, it required a complicated procedure to be used as an impression material.
When the algae used to manufacture agar was unavailable during the second world war, Americans used local algae to manufacture another elastic impression material known as alginate, which has gained popularity since then.
Alginate and agar have disadvantages, like dimensional instability and low tear strength, which led to the manufacture of elastomeric (also known as rubber-based) impression materials. First came polysulfide, then condensation silicone followed by polyether, and then addition silicones.[1][2]
With the advancement in technology, digital dentistry is also making its way into the field.[3] However, there is always a scope for new impression materials, as no impression material is 100% accurate until the date.
Issues of Concern
The wettability of the impression material determines its ability to record fine details, which depends on its viscosity. The more the impression material wets the tissues, the more it will come in close contact with them and capture fine details. The more viscous materials will have limited flow and very few wetting features.[4] In fixed dental prostheses, an impression is expected to reproduce 20 to 70 microns and 100 to 150 microns in removable prosthodontics.
According to international standards, the impression material should record a line of 0.02 mm width or less, which is less than the width of a human hair.[5]
Classification
Impression materials can be classified as follow:
For primary impressions, e.g., alginate, impression compound, elastomeric putty.
For secondary impressions, e.g., light body elastomers and zinc oxide eugenol.
- Based on Setting Reaction
Reversible (physical): impression compound, impression waxes, agar.
Irreversible (chemical): alginate, impression plaster, elastomeric impression materials.
- Based on the State of the Impression Material After Setting in the Oral Cavity
Rigid: impression compound, zinc oxide eugenol, impression plaster, impression waxes.
Elastic: alginate, agar, polysulfides, addition and condensation silicones, polyether.
- Based on Compression of Underlying Tissues
Mucostatic: impression plaster, light body elastomers.
Mucocompressive: impression compound, putty elastomers.
- Based on Consistencies
- Light body
- Medium body
- Heavy body
- Putty
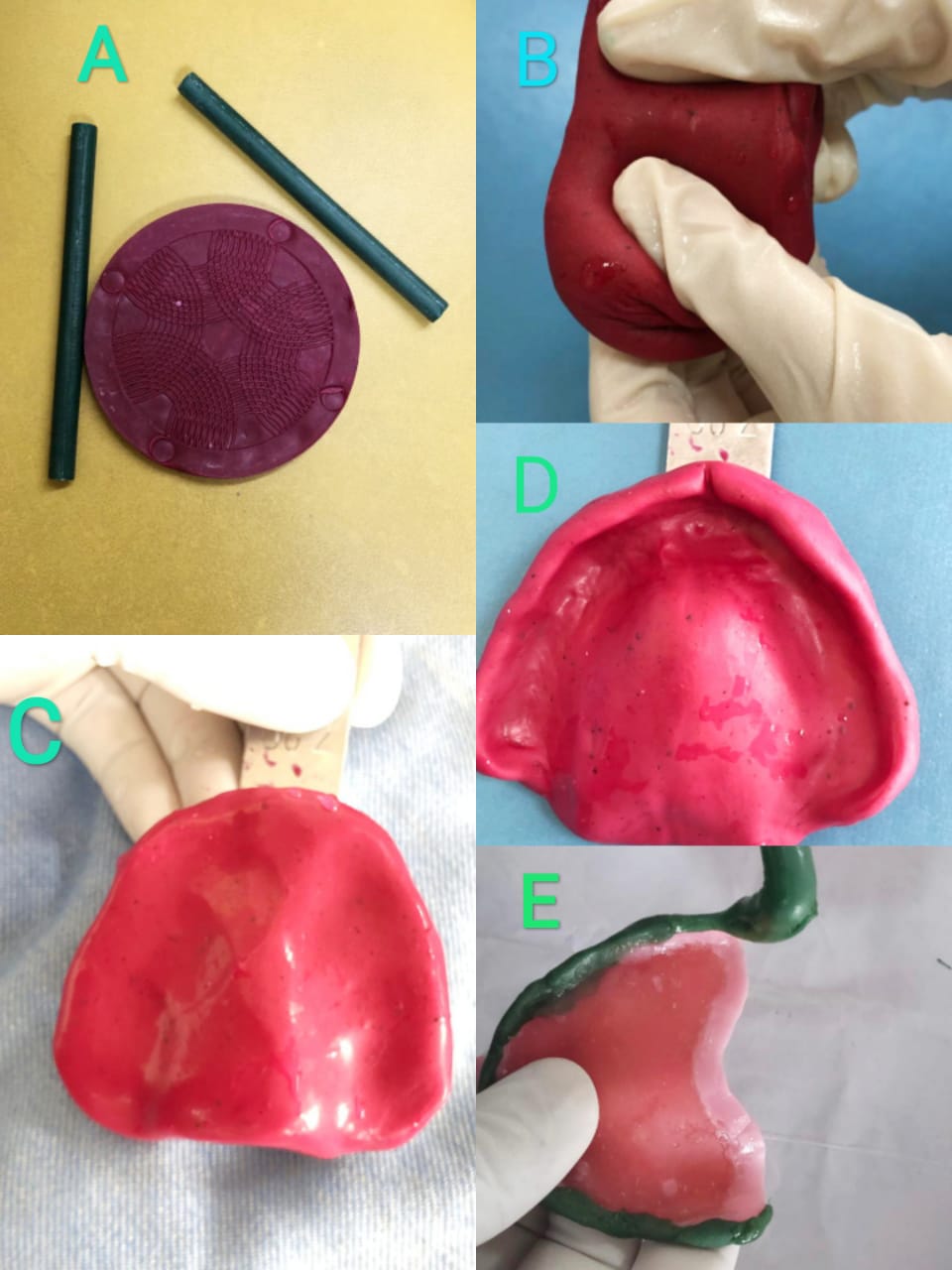
Impression Compound (Fig1)
It is a thermoplastic, rigid and reversible impression material (meaning it can be reused in the same patient if an impression needs to be repeated). It is also known as a modeling compound.
Types
- Type 1: Low fusing impression compound. Available as sheet, rope, and stick. The sheet material impresses edentulous arches, and the stick form is used for border molding.
- Type 2: High fusing impression compound, also known as tray compound. It is used for making impression trays.
Composition
- Rosin 30 parts
- Resin 30 parts
- Carnauba wax 10 parts
- Stearic acid 5parts (gives plasticity)
- Talc 75parts (provides hardness)
- Coloring agents
Mechanism of Action (mode of setting)
It is a thermoplastic material that sets by physical reaction only.
Instruments and armamentarium: water bath, gauge piece, burner, scalpel handle, and blade to modify the impression.
Manipulation
Type 1 sheet impression compound is softened in a water bath with warm water and is placed in a stock tray to copy edentulous ridges. The water bath temperature is kept at around 55-60 degrees Celsius, above the impression compound's fusion temperature.[6] The impression compound is a mucocompressive material, meaning that it impresses the mucosa when subjected to compression. These impressions must be corrected with a second impression made in a custom impression tray fabricated on the primary cast of the patient.
The type 1 stick impression compound is softened over a flame and placed on the borders of the custom impression tray.[7]
The type 2 impression compound is used to make an impression tray to make a wash impression.
Properties
- The impression compound has low thermal conductivity. Therefore one should check the softening of material during manipulation and complete material setting before removing it from the oral cavity.
- Glass transition temperature: This is when amorphous substances start to lose their hardness - for the impression compound is 39 degrees Celsius.
- Fusion temperature: The impression compound reaches the fusion temperature at 43.5 degrees Celcius. Above this temperature, the impression compound remains plastic and can be utilized.
- Viscosity: The impression compound is highly viscous; therefore, impressions are mucocompressive in nature. It gives an extended impression but lacks detail.
Advantages
- It can be reused in the same patient until a good impression is made.
- It can compensate for a short impression tray because it does not sag under its weight.
- It can be electroplated to form dies.
- It can be added or removed until a good impression is made.
Disadvantages
- Due to high viscosity, it does not record fine details.[8]
- Its dimensional stability is poor due to the release of internal stresses incorporated into the material during kneading.
Indications
- Edentulous arch impressions for complete denture fabrication.
- Border molding procedure.
- A single prepared tooth impression (copper tube impression).
Contraindications
- It should not be used in undercuts areas.
The impression should be washed off saliva and disinfected using 2% glutaraldehyde and poured within half an hour to prevent dimensional deformation.
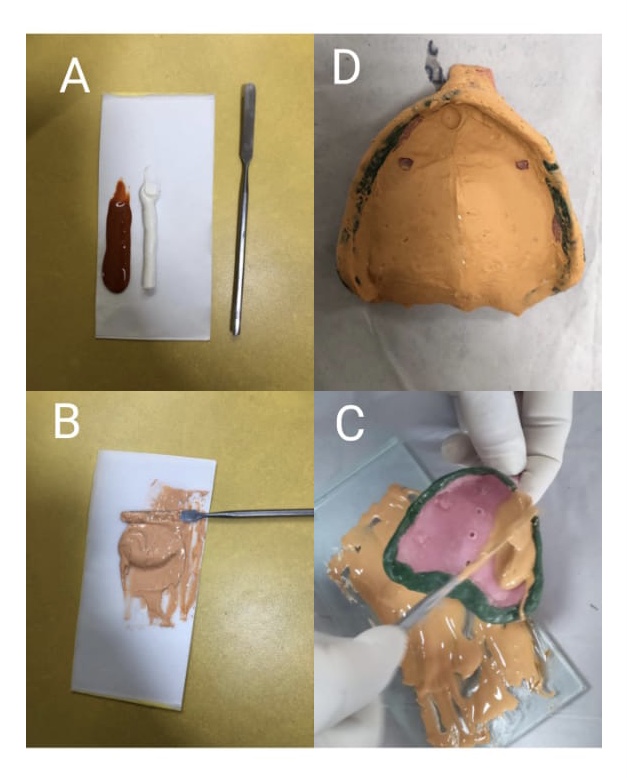
Zinc Oxide Eugenol Impression Material (impression paste)(Fig2)
It is an irreversible nonelastic material used as a final impression (wash impression) in complete denture fabrication. It records the tissues in the undistorted state.[9][10]
Composition: ZOE impression material is available in two collapsible tubes; one contains the base and the other the catalyst.
The base contains:
- ZnO 87%
- Vegetable or mineral oils 13%
The catalyst contains:
- Eugenol 12-15%
- Rosin 50%,
- Fillers 20%, resinous balsam 10%, accelerator, color pigments 5%
*Noneugenol pastes (for patients who are allergic to eugenol) contain carboxylic acids.
Instruments and armamentarium: paper pad or glass slab and broad end spatula.
Manipulation: equal lengths are squeezed out from both tubes on a paper pad or a glass slab and mixed with a broad end spatula until mixed to an even color.
Setting reaction:
It sets in two steps: first, by the hydrolysis of ZnO to form zinc hydroxide (water is required to initiate the reaction). The second stage is a typical acid-base reaction in which zinc hydroxide reacts with eugenolic acid to form zinc eugenolate, forming a chelate and water as a byproduct. The final set structure consists of ZnO particles embedded in the matrix of zinc eugenolate.
The impression paste's setting time can be altered in clinical set up according to need, either decreased by adding a drop of water during mixing or increased by adding vaseline during mixing. The material has a good flow, which records fine details.
ZOE impression has excellent dimensional stability for 24 hrs; therefore, it can be poured within this time. But the special impression tray underneath should not get deformed.[11]
Indications:
- Wash impressions (secondary impression) in complete denture fabrication and dual impression in distal extensions partial dentures.
- Bite registration and interocclusal records.[12]
Contraindications:
- It is a brittle material; it cannot impress dentulous mouths or severe undercuts areas.
- It should not be used in patients who are allergic to eugenol.
Advantages:
- Economical and easy to use
- Good flow helps in recording fine details
- Dimensionally stable
Disadvantages:
- It cannot be used in stock trays; custom trays are mandatory
- Fragile
- Can produce burning sensation of the mucosa
- Setting time varies with temperature and humidity
Properties:
- Rigid
- Low viscosity
- Good surface details in thin section (0.5mm)
- Dimensionally stable (0.1% contraction)
- Compatible with gypsum products
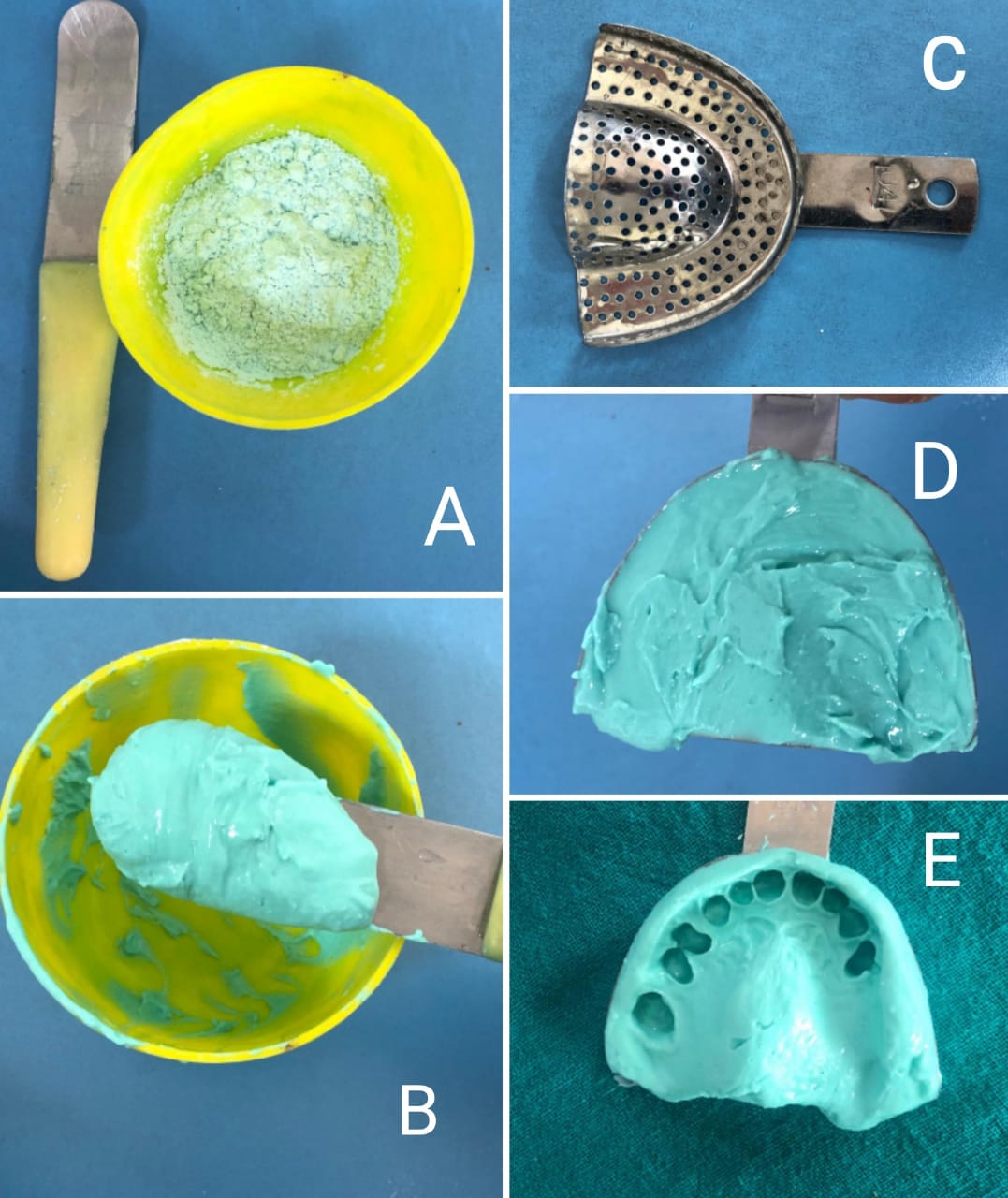
Alginate (Fig3): Alginate is a hydrocolloid widely used as an impression material in dentistry. It is derived from alginic acid, present in brown algae. It is an irreversible and elastic impression material.[13]
Composition:
- Sodium or potassium alginate (15%) - dissolves in water and forms a viscous sol.
- Calcium sulfate (16%) - reactor
- Diatomaceous earth (60%) - filler
- Zinc oxide (4%) - filler
- Potassium titanium fluoride (3%) - accelerator
- Sodium phosphate (2%) - retarder
- Glycol (in dustfree alginates)
- Pigments and flavoring agents
Indications:
- Diagnostic casts for treatment planning
- Orthodontic study models
- Impressions to fabricate partial and complete dentures, and temporomandibular disorders appliances
- For duplicating models
Instruments and armamentarium: flexible rubber bowl, curved spatula, measuring scoop, perforated impression tray, alginate powder, and water.
Manipulation:
The water is added first to the rubber bowl and then the powder; the manufacturer gives the proportions. The mixture is mixed vigorously against the walls of the bowl in a figure of eight motion. The mixing time is 45-60 seconds according to the type of alginate. Then the mixture is loaded into the selected impression tray (tray border should be a maximum of 3 mm short of vestibular depth) and placed into the patient's dental arch. After the alginate attains sufficient elasticity, the impression is removed. There should be a minimum of 3 mm thick material between the tray and tissues not to get torn. The impression should be removed swiftly, simultaneously breaking the seal by inserting fingers in the buccal vestibular region. The impression must be cast within half an hour as hydrocolloids tend to deform because of imbibition and syneresis.[14] The impression could be kept in 100% humidity and cast within 24 hours instead. But for optimum dimensional stability, an alginate impression should be poured immediately.[15]
Setting reaction:
It is a sol to gel transformation divided into two steps: 1) retardation reaction 2) gelation reaction.
First, calcium sulfate reacts with trisodium phosphate to form calcium sulfate and sodium sulfate; the second stage starts after all the trisodium phosphate gets consumed, which provides optimum working time in the manipulation of alginate. In the gelation reaction, potassium alginate reacts with calcium sulfate to form calcium alginate gel.
Advantages:
- Affordable
- Short manipulation time
- Simple technique
- Few armamentaria required
- Good impression (even in the presence of undercuts) all in a single step [16][17]
Disadvantages:
- Low tear strength
- Dimensional instability
Modified alginates:
- Dustless alginates: manufactured to prevent inhalation of alginate particles, which may cause respiratory problems. The alginate particles are coated with glycol or glycerine to make them denser.
- Chromatic alginates: change colors during manipulation to guide mixing time and setting time.
- In the form of sol or paste (containing water) and reactor (plaster of pairs) separately.
Agar: Agar is another hydrophilic colloid impression material like alginate but reversible. It is the first elastic impression material to be used in dentistry.
Composition: Chemically, agar is a sulfuric ester of the galactan complex, and agar is available as a tray or syringe material.
- Agar (gelling agent)
- Borax (strengthener)
- Potassium sulfate (gypsum hardener)
- Alkyl benzoate (preservatives)
- Water (reaction medium > 80%)
- Fillers, flavoring, and coloring agents
Manipulation:
It requires hydrocolloid conditioner equipment with three compartments to heat, store and temper the material and special impression trays that can circulate water.
First, the material is boiled in the first compartment and changed to sol from gel state. In the second compartment, the material is stored at 65 degrees Celsius and used when needed. The agar is brought to 45 degrees Celsius in the tempering section to impress oral tissues comfortably. The water circulates through the tubing and converts the sol into a gel state.
Indications:
The agar has been used in dentistry for cast duplication and impression making. Its use is now limited as it requires a complicated setup.[18]
Properties:
- Hydrophilic, meaning better impressions in the presence of saliva. Agar has been used for making subgingival crown preparation impressions when it is not easy to keep the area dry.
- Dimensional stability: As this is a hydrocolloid (water-based), it may lead to deformation due to imbibition (absorption of water ) or syneresis (exudation of fluids) if the impression is not poured immediately.
- It has an optimum flow to record fine details of hard and soft tissues.
- Compatibility issues with gypsum because borax interferes with gypsum setting, a gypsum hardener is added.
Advantages:
- Reversible
- Affordable
- Nontoxic, odorless, and nonstaining
Disadvantages
- Requires purchasing a water bath
- Low tear strength
- Dimensional instability
- Infection control unfriendly
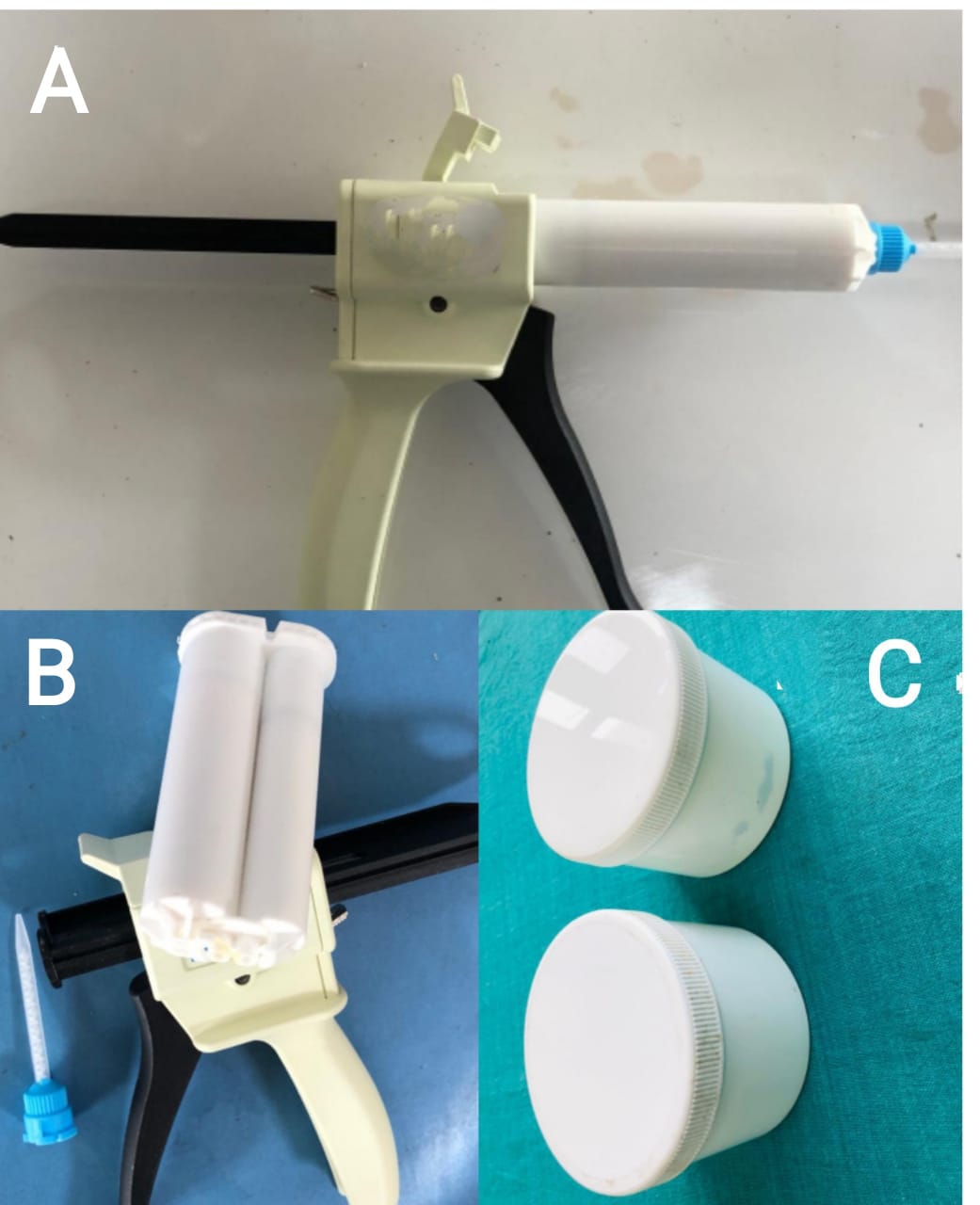
Elastomeric Impression Materials (Fig4)
Elastomers are required when precision is of utmost importance, like crown and bridge preparation and implants.
Four types of elastomeric impression materials are available in the market: addition silicone, also known as polyvinyl siloxanes (PVS), condensation silicone, polyether, and polysulfide.
Elastomers can present in different consistencies, including putty, heavy body, medium body, and light body. The putty type is available in two jars containing base and catalyst; the medium body is dispensed in two collapsible tubes as base and catalyst; and the light body in syringes.
Addition Silicone: they are the most widely used impression materials in fixed prosthodontics.
Mode of supply: Available in all consistencies( extra-low, low, medium, heavy, and putty)
Composition: All the consistencies are supplied as base and accelerator
The base contains:
- Hydroxy terminated polysiloxane polymer -undergoes crosslinking.
- Fillers - control viscosity
The accelerator contains:
- Divinylpolysiloxane prepolymers - crosslinking agents.
- Chloroplatinic acid - catalyst
- Palladium - hydrogen absorber
- Fillers
Setting reaction:
The base paste containing hydrosilane-terminated molecules reacts with an accelerator paste containing siloxane oligomers with vinyl end groups and a platinum catalyst. Although no by-product is formed, a secondary reaction leads to hydrogen gas production. That is why it is recommended to wait at least 30 minutes rather than have a pitted cast.[19]
Advantages:
- Excellent dimensional stability - impressions can be stored or posted before casting.
- Elastic recovery
- Great accuracy
- Short setting time
- Good tear resistance
- Automix available
- Hydrophilized addition silicone has good compatibility with gypsum
- The impression can be cast multiple times without jeopardizing the details[20]
Disadvantages:
- Hydrophobic - the impression area must be dry to prevent inaccuracies in the impression[21]
- The sulfur present in the latex gloves and rubber dam may interfere with the polymerization of the base and catalyst.
- Hydrogen gas may lead to pitting in the cast.
Indications:
- Fixed prosthesis: crown, bridges, implant
- Maxillofacial prosthodontics
- Registering occlusion
Polyether: it has become popular because it only requires a stock tray and a single mix.
Mode of supply:
Available as light, medium, and heavy body consistencies.
Composition:
The base contains:
- Polyether
- Fillers
- Plasticizers
The accelerator contains:
- Alkyl aromatic sulfonates
- Inert oils
- Plasticizers
Setting reaction:
When base and accelerator are mixed in equal proportions, polyether rubber is formed.
Indications
- Fixed prosthodontics (crown and bridgework, particularly for multiple preparations)
- Implants
- Border molding in complete denture fabrication
- Indirect inlay and onlay impressions
- It can be used for corrective impressions as it can be added to previously set material.
Advantages:
- Hydrophilic
- Accurate and high dimensional stability - makes it possible to delay casting and allow multiple pouring.
- Good elastic recovery
- Good compatibility with gypsum
- Good shelf life
- It can be used as a single-phase material or with a syringe tray technique
Disadvantage:
- Most rigid of all the elastomers makes it hard to remove (newer polyethers are slightly more flexible)
- May cause allergy due to sulfonate acid esters
The impression should not be immersed in disinfectant for more than 10 minutes since it's hydrophilic.[22][23] Since it absorbs water, it should not be kept with alginate impressions.
Polysulfide: these are the first elastomers to be introduced. Although messy to manipulate, it is useful when a long working time is needed. Polysulfides are not recommended except for complete dentures.
Consistencies:
Mode of supply:
It is available in a two-paste system: base and accelerator.
Composition:
The base contains:
- Polysulfide prepolymer
- Filler for strength
- Plasticizer for optimum consistency
- Sulfur as an accelerator
The catalyst contains:
- Lead oxide (gives characteristic brown color)
- Filler, plasticizers, and retarders
- Setting reaction:
The polysulfide prepolymer reacts with lead oxide, forming polysulfide rubber and water. The reaction byproduct significantly affects the dimensional stability of the impression; therefore, the impression should be cast immediately. Polysulfide is the most flexible of elastomeric materials, and it can be easily removed from undercut areas.[24]
Advantages:
- Least rigid (most flexible of all the elastomers)
- Good tear strength
- Most biocompatible
- Excellent flow so good reproduction of details
- Hydrophilic
Disadvantages:
- Requires a custom tray
- Long setting time
- Must be poured within half an hour
- Hydrophobic
- Bad odor
- Unpleasant taste
- Stains the clothes
- Messy to work
Indications
Only recommended in complete denture cases.
Condensation silicone: they are more affordable than other elastomeric materials but have the disadvantage of being prone to shrinkage, requiring immediate pouring.
Consistencies: extra-low, Low, medium, and putty
Mode of supply:
- In collapsible tubes as base and catalyst (medium body)
- In jars as base and catalyst (putty)
- Syringes (ultralow and low)
Composition:
The base contains:
- Hydroxy terminated polydimethylsiloxane - forms polymer.
- Fillers - controls viscosity.
The accelerator contains:
- Tetraethyl silicate
- Tin octoate (catalyst)[25]
Setting reaction:
Condensation polymerization reaction occurs with the release of alcohol as a byproduct that evaporates as formed.
Advantages:
- Good elastic recovery
- Pleasant odor and taste
- Accurate reproduction
Disadvantages:
- Dimensional deformation over the time
- Hydrophobic
- Dimensional stability is affected due to reaction byproducts[25]
Delivery systems of elastomers:
Elastomers are typically constituted by a base and a catalyst. The light body comes in a syringe, the regular body is available in collapsible tubes, and the putty is dispensed in two jars. The mixing can be done manually or by automix systems, e.g., disposable intraoral syringes, automatic mixing machines, and dispensers with attached cartridges.
Steps in elastomeric impression making:
First, the impression tray is selected and prepared with tray adhesive. The impression material is mixed, manually, or by mechanical means.
The impression technique may vary according to the case, including multiple mix, monophase, or putty wash techniques.[25]
Digital Impressions
The advantages of intraoral scanning are too many: the material and armamentarium used in analog impressions are avoided (e.g., impression trays, impression material, gypsum); the communication between the clinician and laboratory technician is improved since the image can be modified, recaptured, a soft copy can be stored; and the cross infections can be minimized due to absence of physically stored casts.
However, digital impressions require an expensive setup, images of completely edentulous arches are less accurate, the presence of blood and saliva obscures subgingival finish lines, and they do not record complete occlusal information for comprehensive prosthodontic treatments.[26][27] But, for single units and segmental dentistry, the intraoral scanners are highly accurate.[28]