Introduction
The mandible, which holds the lower teeth, comprises the majority of the lower third of the maxillofacial skeleton and is of utmost functional importance. Complex mandibular movements are afforded by the masseter, temporalis, medial pterygoid, lateral pterygoid muscles, and temporomandibular joints.[1] Given that the maxilla is stationary, mastication is dependent on mandibular movement. In certain populations, masticatory function related to dental status is a significant determinant of nutritional status. Being an edentulous geriatric patient without complete dentures was shown to be an independent risk factor for malnutrition.[2] This suggests the importance of functional occlusion.
Occlusion is the articulation between the mandibular and maxillary dental arch. Static and dynamic occlusal relationships can be described in many ways.[3][4] Understanding the occlusal contact relationship impacts the providers' ability to design and place dental implants, implement orthodontic braces, fit dentures, re-establish masticatory function, and restore a patient’s native bite after maxillofacial trauma.
Structure and Function
Mandible
The mandible consists of a body, rami, coronoid processes, and condylar processes. The mandible can be further subdivided into the angle where the ramus transitions to the body, the body, the parasymphysis located anterior to the mental foramen, and the midline symphysis. Mobility in the mandible allows for its participation in mastication and occlusion.[5] The muscles of mastication contribute to the mandible's complex movements and include the temporalis, masseter, medial pterygoid, and lateral pterygoid.[6] There are primarily 6 types of mandibular movement, including opening, closing, rightward jaw translation, leftward jaw translation, protrusion, and retrusion. Variability in jaw movement allows for mastication of different textures and consistencies.
Temporomandibular Joint (TMJ)
The temporomandibular joint is the junction of the mandible and the temporal bone. These are synovial joints, each with an upper and lower compartment divided by an intra-capsular disc. The mandibular condyle articulates with the intra-capsular disc and remains in the mandibular fossa at rest when the jaw is closed. The condyle follows the articular eminence forward during jaw opening.
Condylar movements during mastication are complex. In total, condylar actions within the temporomandibular joints have 3 basic movements: spin, roll, and slide. Spin describes the condylar head twisting about a vertical axis within the capsule. Roll is the condylar head rocking back and forth with the central portion maintaining contact with the intra-capsular disc. Slide refers to the translation of the condylar head relative to the intra-capsular disc.
Intricate movements within the temporomandibular joint translate to mandibular movements needed for mastication. To allow maximal mouth opening, the condyles move downward and forward over the articular eminence. The closing force begins with the condyle ipsilateral to the food bolus moving back into the mandibular fossa upwards and posteriorly to a position lateral from resting. Through closing, the ipsilateral condyle shifts medially while the contralateral condyle moves upward, posteriorly, and laterally.
Maxillary and Mandibular Dental Arch
The permanent, succedaneous teeth in adults consist of 16 teeth in the maxilla and 16 teeth in the mandible. The universal numbering system for permanent teeth assigns numbers to each tooth from 1 to 32. Tooth #1 is the right maxillary third molar followed sequentially by numbers 2-15 across the maxilla until reaching the left maxillary third molar, tooth #16. Numbering continues down to the mandible, with tooth #17 being the left mandibular third molar followed by 18-31 proceeding sequentially across the mandible until reaching the right mandibular third molar, which is tooth #32.[7][8] There are alternative numbering systems.
Adult dentition consists of 2 central incisors, 2 lateral incisors, 2 canines, 2 first premolars, 2-second premolars, 2 first molars, 2-second molars, and 2 third molars, both in the maxilla and mandible. The teeth are secured within the alveolar ridges of the maxilla and mandible. Dentition, whether native or restored, is integral to masticatory function.[9]
Dental Occlusal Anatomy
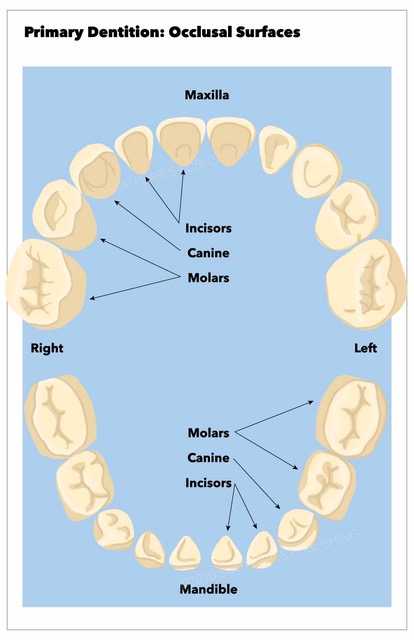
The following 5 surfaces of the crown of a tooth allow for discussion of occlusal contacts:[8]
- Facial: oriented toward the lips or teeth and referred to as labial for incisors/canines or buccal for premolars/molars
- Palatal/Lingual: oriented towards the palate for the maxilla and the tongue for the mandible
- Mesial: oriented toward the midline
- Distal: oriented away from the midline
- Occlusal: oriented toward the upper or lower jaw depending on the mandible versus the maxilla
Tooth cusps function to guide erupting teeth into appropriate occlusion with periodontal stimulation informing neural reflexes for jaw closure and mastication [1]. The maxillary palatal cusps and the mandibular facial cusps comprise the centric cusps involved in centric occlusion (discussed below). In contrast, the maxillary buccal cusp and the mandibular lingual cusps guide the mandible during the lateral excursion.
When in occlusion, a lateral view shows a convexity in the maxillary occlusal surface interdigitating with a concavity in the mandibular occlusal surface. The occlusal curve is called the Curve of Spee. Extending the curve while maintaining its arc into a circle centered at the glabella creates the Curve of Monson. In a coronal plane, the mandibular posterior dentition is characterized by a lingual incline, and a buccal incline characterizes the maxillary posterior dentition. The coronal occlusal curve in the posterior dentition is called the Curve of Wilson.[10] Maintaining these characteristic occlusal curves is imperative to the practice of dental implants and denture design/fitting.
Mandibular Movements and Dynamic Occlusal Contacts
The sophisticated movements of the mandible impacting dynamic occlusal contacts are a combination of the 6 primary mandibular movements as well as the condylar movements discussed above. Posselt published his seminal work in the mandibular movement in 1952, including Posselt’s envelope of motion. This depicts the movement of the mandible in a sagittal plane. When the condyle is superior and anterior within the glenoid fossa, the mandible is maximally retruded. In this condyle position, the mandibular opening is referred to as centric relation, and this depends on the rolling (hinge) movement facilitated by the lower synovial cavity in the TMJ. Opening beyond this is dependent on the sliding (translational) movement of the upper synovial TMJ cavity. The first occlusal contact upon mandibular closing, when in centric relation, is referred to as centric occlusion. This is followed by the teeth sliding into the intercuspal position, where maximal intercuspal contacts are made in the occlusion. The Envelope of Motion's anterior arc illustrates mandibular movement into occlusion and opening when the mandible is maximally protruded.
For lateral movement, the mandible is designated into working and non-working sides. The side that the mandible is moving toward is the working side, and that condyle moves laterally. The amount of movement laterally in the condyle is referred to as the Bennett movement. On the non-working side, the lateral movement necessitates downward, inward, and forward positioning of the condyle. The difference between a sagittal plane established through the condyle at rest and a line through the lateral movement's non-working condyle is the Bennett angle, the average being 7.5 degrees.[1][4]
Embryology
The first branchial arch gives rise to Meckel's cartilage. On the lateral aspect of Meckel’s cartilage, the mandible starts as two halves, with each half developing an ossification center in the sixth to seventh week of intrauterine development. The ossification centers develop into what will eventually be the symphysis, body, angle, and ramus of the mandible. Separately, cartilage clusters form within the connective tissue, eventually ossify into coronoid and condylar processes.
The two ossified right and left halves of the mandible remain separated by connective tissue until closer to birth when small mental bone(s) (1 or 2) ossify. These mental bones ultimately fuse with the mandible creating a mental protuberance and the unified mandibular bone.[11]
Mesenchymal cells from the first branchial arch give rise to the muscles of mastication.[8]
Odontogenesis is the formation of teeth. The deciduous or baby teeth develop at 6 to 8 weeks gestation, whereas succedaneous teeth develop at 20 weeks. The ectoderm forms the dental enamel, while the ectomesenchyme (neural crest-derived) forms the dentin, cementum, periodontal ligament, and pulp. Placodes represent invaginations of primary dental lamina within the mandibular and maxillary arches beginning the process of tooth formation. Tooth buds form from the placodes, and the tooth buds develop into teeth.[11]
Blood Supply and Lymphatics
The endosteal blood supply of the mandible is derived from the external carotid artery. The mandibular ramus, condyle, and coronoid have a blood supply from the intramedullary ascending artery (from the inferior alveolar artery), a direct branch of the maxillary artery pterygoid osteomuscular branches. The inferior alveolar artery supplies the mandibular angle and body. Finally, the mandibular symphysis has a rich blood supply consisting of contributions of the submental artery from the facial artery, the sublingual artery from the lingual artery, and the incisive artery from the inferior alveolar artery.[12]
The maxillary artery, a branch of the external carotid artery, branches into the anterior, middle, and posterior superior alveolar arteries providing a blood supply to the maxillary dentition.[8]
The oral cavity primarily has lymphatic drainage to cervical lymph nodes in levels I (submental and submandibular), II (upper internal jugular chain), and III (middle internal jugular chain).[13]
Nerves
The trigeminal nerve is the 5 and largest cranial nerve. There are three branches of the trigeminal nerve including: ophthalmic (V1), maxillary (V2), and mandibular (V3).[14] The V2 and V3 divisions are the most relevant for occlusal contact relationships and mandibular movements.
The trigeminal nerve's maxillary division exits the skull base via the foramen rotundum, traverses the pterygopalatine fossa, enters the inferior orbital fissure, and ultimately gives rise to the inferior orbital nerve. This nerve is the origin of the anterior branch of the superior alveolar nerve providing sensation to the anterior hard palate, incisors, and canines. For the molars and posterior two-thirds of the palate, sensation comes from the greater palatine nerves arising from the maxillary nerve.[8]
The mandibular division of the trigeminal nerve exits the skull base via the foramen ovale. The anterior branch provides motor innervation to the muscles of mastication. The posterior branch provides sensory innervation via the long buccal nerve, inferior alveolar nerve (IAN), and the lingual nerve. The IAN provides sensory innervation for mandibular molars and premolars. A small branch of the IAN, the incisive nerve, branches just before the IAN exits the mental foramen becoming the mental nerve. The incisive nerve provides sensation to the mandibular canines and incisors.[8][11]
Muscles
The muscles of mastication are also responsible for occlusion, given that they are the predominant mobilizers of the mandible.
Muscles of Mastication[6][15]
|
Muscle
|
Origin
|
Insertion
|
Action
|
|
Temporalis
|
Temporal fossa
|
Coronoid process of the mandible
|
Elevate the mandible closing the jaw, mandibular retraction, and with unilateral action deviate the mandible to the ipsilateral side
|
|
Masseter
|
Zygomatic arch
|
Lateral aspect of the mandibular ramus
|
Elevate the mandible closing the jaw, mandibular retraction, some degree of protrusion of the mandible, and approximation of dentition (occlusion)
|
|
Medial pterygoid
|
Medial surface of the lateral pterygoid plate (sphenoid bone)
|
Medial aspect of the mandibular ramus and angle
|
Assists with mandible elevation (jaw closure), protrusion of mandible, and side-to-side mandibular movement for grinding in coordination with the lateral pterygoid
|
|
Lateral pterygoid
|
The lateral surface of the lateral pterygoid plate (sphenoid bone)
|
Condylar process of the mandible
|
Upper head: jaw-closing
Lower head: mandible depression (jaw opening), protrusion of the mandible, and side-to-side mandibular movement for grinding in coordination with the medial pterygoid
|
Suprahyoid Muscles
The suprahyoid muscles contribute to mandible depression (jaw opening). These include the digastric, stylohyoid, mylohyoid, and geniohyoid muscles.[16]
Physiologic Variants
Variation in static occlusion seen in the general population can be further described using various classifications. In 1899, Edward Angle introduced his classification of occlusion.[17] This system is based on normal occlusion being determined by the relationship between the maxillary and mandibular first molar as below.
Angle’s Classifications[3]
|
Class
|
Description
|
|
I
|
the mesiobuccal cusp of the first maxillary molar sits in the buccal groove of the first mandibular molar
|
|
II
|
the mesiobuccal cusp of the first maxillary molar is mesial to the buccal groove of the first mandibular molar
|
|
III
|
the mesiobuccal cusp of the first maxillary molar is distal to the buccal groove of the first mandibular molar
|
There are variations in native occlusion in the population. 52% of the population is Angle’s class I. While 26.2% are classified as Angle class II and 2.6% being Angle’s class III. This classification system is imperfect, leaving 21% of the population not clearly falling into any Angle classes.[17]
Transverse and vertical relationships between maxillary and mandibular dentition can be described as well.
Lingual-labial/buccal Relationship[3]
|
Designation
|
Description
|
|
Normal
|
Maxillary dentition is labial/buccal to mandibular dentition
|
|
Anterior crossbite
|
Anterior maxillary dentition is lingual to mandibular dentition
|
|
Posterior crossbite
|
Posterior maxillary dentition is lingual to mandibular dentition
|
Vertical Relationship[3]
|
Designation
|
Description
|
|
Normal
|
Anterior maxillary dentition extends 2-3 mm inferior to the occlusal surface of mandibular dentition.
|
|
Open bite
|
Lack of occlusal contact
|
|
Overbite
|
Anterior maxillary dentition extends beyond 3 mm inferior to the occlusal surface of mandibular dentition.
|
Overjet differs from overbite as overjet is the measure of how far anterior the maxillary dentition is in front of the mandibular dentition.[18]
Surgical Considerations
Orthognathic surgery repositions the maxilla, the mandible, or both. There are numerous indications for orthognathic surgery, including obstructive sleep apnea, Angle’s class II occlusion, Angle class III occlusion, canting of the occlusal plane, aesthetic considerations, and an open bite, among others. A LeFort I osteotomy for the maxilla and bilateral sagittal split osteotomies for the mandible are the mainstays for modern orthognathic surgery. With both the maxilla and mandible manipulated, there is an opportunity to dramatically change a patient’s occlusion. For this reason, dental modeling is imperative to the process, whether done with traditional stone model surgery or virtual surgical planning.[19][20]
Maxillofacial trauma treatment, including mandibular and LeFort midface fractures, is founded upon pre-traumatic occlusion restoration. Some fracture patterns, particularly in the mandible, resulting in predictable malocclusions. For example, a condylar or subcondylar fracture reduces the vertical height of the mandible, causing premature contact of the ipsilateral posterior dental arch. An anterior open bite characterizes a bilateral condylar fracture because of these dimensional changes.[3]
Mobility of the mandible and/or the maxilla can create complex clinical situations in which occlusion can be altered adversely. Maxillomandibular fixation (MMF) is used intraoperatively to re-establish a patient’s occlusion. This can be achieved using Erich arch bars, inter-maxillary fixation screws, or rapid maxillomandibular fixation systems, among other techniques. With native occlusion secured using MMF, the midfacial fractures and/or mandibular fractures can be reduced and internally fixated.[16][21] In this way, the occlusion is the foundation of the repair.
Mandibular movement can influence forces surrounding mandibular fractures. The suprahyoid musculature and bite force puts downward anterior pressure on the mandible. The masseter, temporalis, and pterygoid muscles pull the posterior mandible upward. These opposing forces can reduce some (favorable) fractures and displace other (unfavorable) fractures.[16]
Clinical Significance
Occlusal contact relations are between the maxillary and mandibular dental arches. The quality of these contacts allows for efficient mastication. Nutritional status is dependent on the dental status of a patient, as prior literature has shown.[2] Mastication is reliant on mandibular movements that can be complex, requiring coordination between temporomandibular joints and the muscles of mastication.
There are many ways to examine the quality of occlusion, and this is exemplified when considering dental implants or denture design. In maxillofacial trauma, occlusion can be altered from the trauma itself or suboptimal management of fractures. Keeping the dental occlusion as the foundation for these repairs prevents long-term malocclusion.[3] In other cases, malocclusion can be developmental and adversely impact cosmesis, which is the case for some patients seeking orthognathic surgery.[20]