[1]
Zimmer L,Luxen A, PET radiotracers for molecular imaging in the brain: past, present and future. NeuroImage. 2012 Jun
[PubMed PMID: 22222719]
[2]
Lameka K, Farwell MD, Ichise M. Positron Emission Tomography. Handbook of clinical neurology. 2016:135():209-227. doi: 10.1016/B978-0-444-53485-9.00011-8. Epub
[PubMed PMID: 27432667]
[3]
Zhang Y, Wang J. Targeting uptake transporters for cancer imaging and treatment. Acta pharmaceutica Sinica. B. 2020 Jan:10(1):79-90. doi: 10.1016/j.apsb.2019.12.005. Epub 2019 Dec 16
[PubMed PMID: 31993308]
[4]
Barollo S, Bertazza L, Watutantrige-Fernando S, Censi S, Cavedon E, Galuppini F, Pennelli G, Fassina A, Citton M, Rubin B, Pezzani R, Benna C, Opocher G, Iacobone M, Mian C. Overexpression of L-Type Amino Acid Transporter 1 (LAT1) and 2 (LAT2): Novel Markers of Neuroendocrine Tumors. PloS one. 2016:11(5):e0156044. doi: 10.1371/journal.pone.0156044. Epub 2016 May 25
[PubMed PMID: 27224648]
[5]
The MICAD Research Team, 4-[{sup}18{/sup}F]Fluoro-l-{i}m{/i}-tyrosine Molecular Imaging and Contrast Agent Database (MICAD). 2004
[PubMed PMID: 20641732]
[6]
Ossenkoppele R, Rabinovici GD, Smith R, Cho H, Schöll M, Strandberg O, Palmqvist S, Mattsson N, Janelidze S, Santillo A, Ohlsson T, Jögi J, Tsai R, La Joie R, Kramer J, Boxer AL, Gorno-Tempini ML, Miller BL, Choi JY, Ryu YH, Lyoo CH, Hansson O. Discriminative Accuracy of [18F]flortaucipir Positron Emission Tomography for Alzheimer Disease vs Other Neurodegenerative Disorders. JAMA. 2018 Sep 18:320(11):1151-1162. doi: 10.1001/jama.2018.12917. Epub
[PubMed PMID: 30326496]
[7]
Foster NL,Heidebrink JL,Clark CM,Jagust WJ,Arnold SE,Barbas NR,DeCarli CS,Turner RS,Koeppe RA,Higdon R,Minoshima S, FDG-PET improves accuracy in distinguishing frontotemporal dementia and Alzheimer's disease. Brain : a journal of neurology. 2007 Oct;
[PubMed PMID: 17704526]
[8]
Rinne JO. Positron emission tomography in the differential diagnosis of parkinsonism. Journal of movement disorders. 2009 Oct:2(2):53-7. doi: 10.14802/jmd.09015. Epub 2009 Oct 30
[PubMed PMID: 24868357]
[9]
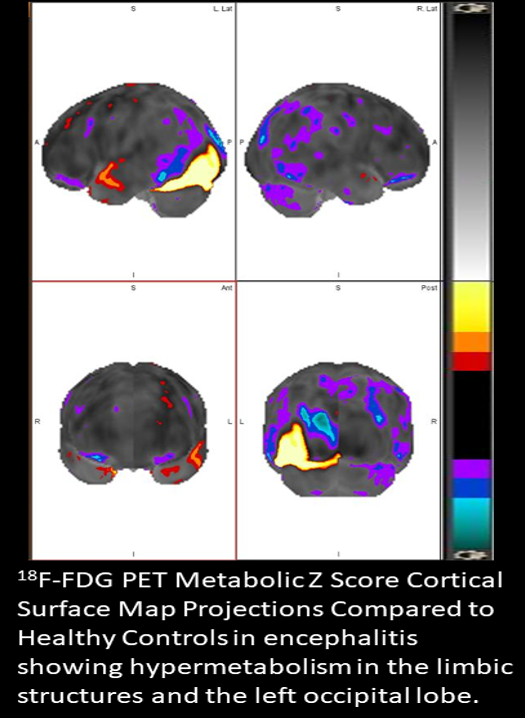
Moreno-Ajona D, Prieto E, Grisanti F, Esparragosa I, Sánchez Orduz L, Gállego Pérez-Larraya J, Arbizu J, Riverol M. (18)F-FDG-PET Imaging Patterns in Autoimmune Encephalitis: Impact of Image Analysis on the Results. Diagnostics (Basel, Switzerland). 2020 May 29:10(6):. doi: 10.3390/diagnostics10060356. Epub 2020 May 29
[PubMed PMID: 32486044]
[10]
Holzgreve A,Albert NL,Galldiks N,Suchorska B, Use of PET Imaging in Neuro-Oncological Surgery. Cancers. 2021 Apr 26
[PubMed PMID: 33926002]
[11]
Shukla AK, Kumar U. Positron emission tomography: An overview. Journal of medical physics. 2006 Jan:31(1):13-21. doi: 10.4103/0971-6203.25665. Epub
[PubMed PMID: 21206635]
Level 3 (low-level) evidence
[12]
Vaquero JJ, Kinahan P. Positron Emission Tomography: Current Challenges and Opportunities for Technological Advances in Clinical and Preclinical Imaging Systems. Annual review of biomedical engineering. 2015:17():385-414. doi: 10.1146/annurev-bioeng-071114-040723. Epub
[PubMed PMID: 26643024]
Level 3 (low-level) evidence
[13]
GBD 2016 Dementia Collaborators. Global, regional, and national burden of Alzheimer's disease and other dementias, 1990-2016: a systematic analysis for the Global Burden of Disease Study 2016. The Lancet. Neurology. 2019 Jan:18(1):88-106. doi: 10.1016/S1474-4422(18)30403-4. Epub 2018 Nov 26
[PubMed PMID: 30497964]
Level 1 (high-level) evidence
[14]
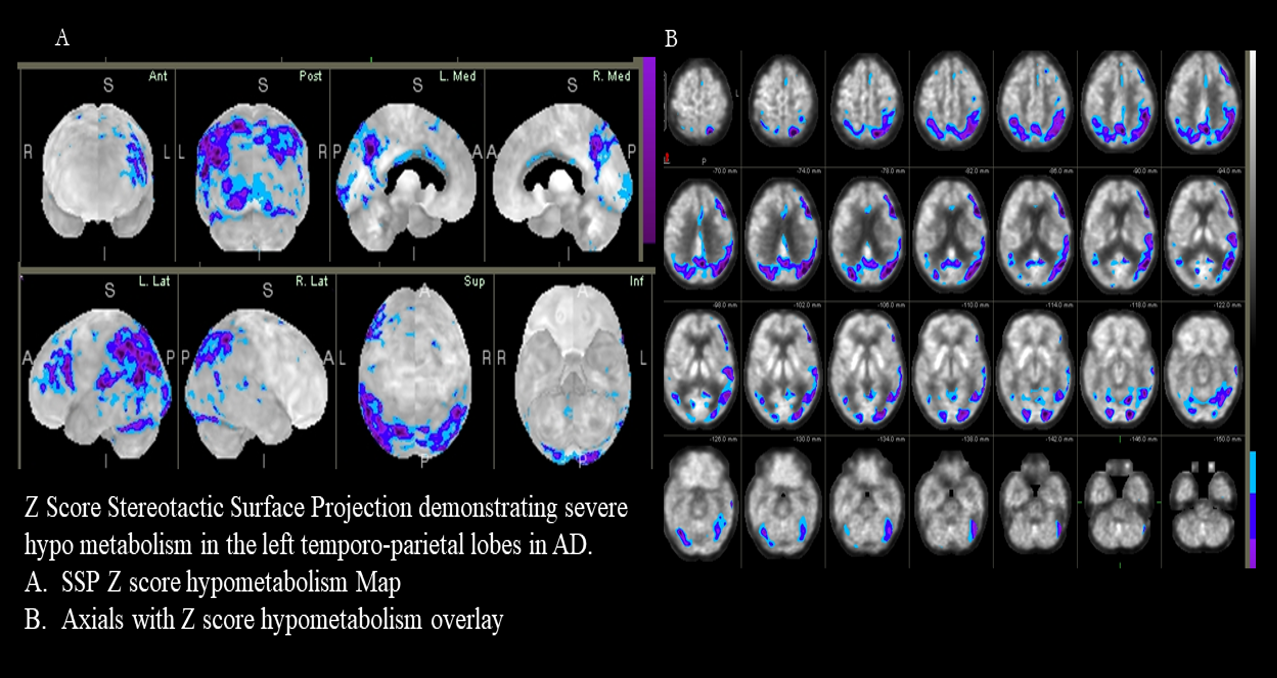
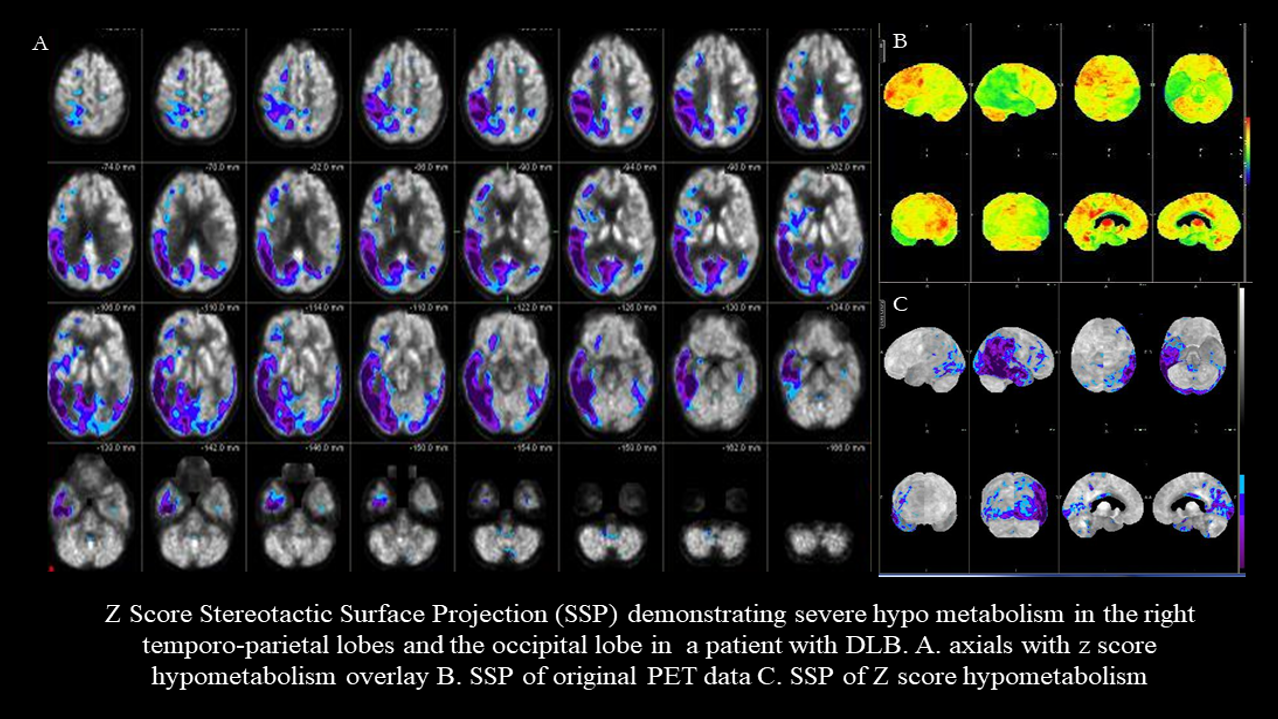
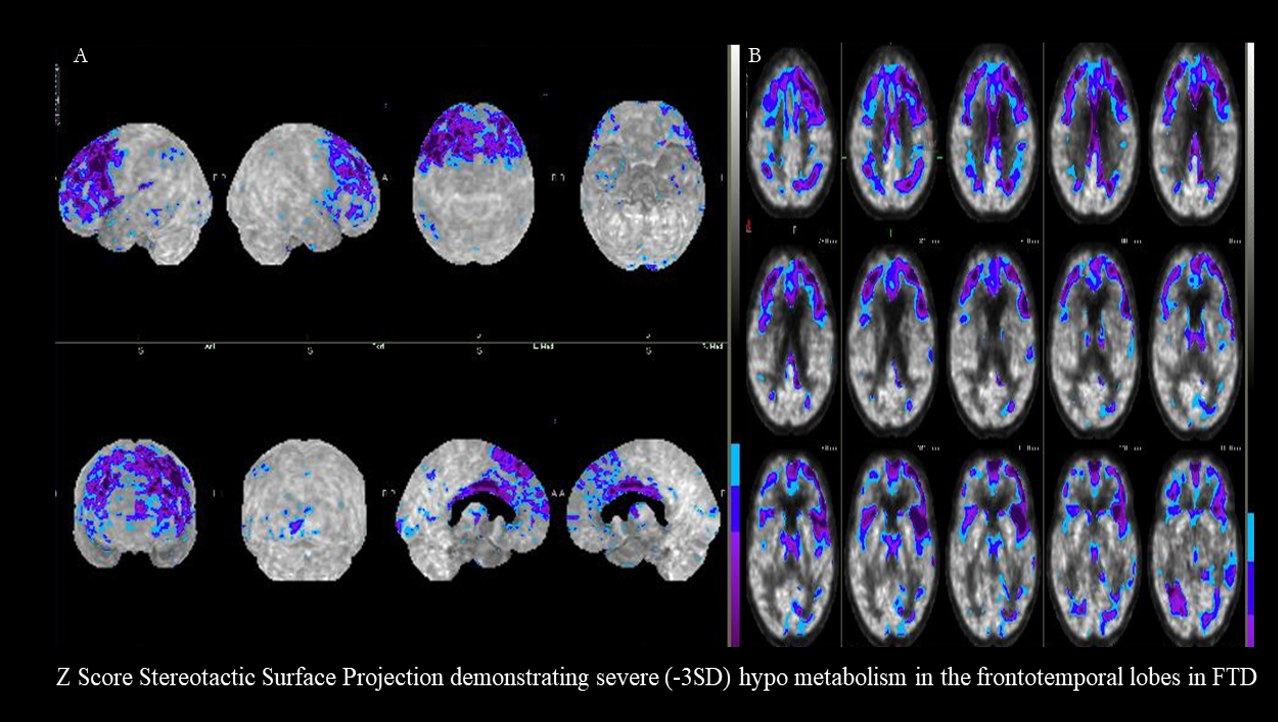
Minoshima S,Mosci K,Cross D,Thientunyakit T, Brain [F-18]FDG PET for Clinical Dementia Workup: Differential Diagnosis of Alzheimer's Disease and Other Types of Dementing Disorders. Seminars in nuclear medicine. 2021 May
[PubMed PMID: 33546814]
[15]
Chételat G,Arbizu J,Barthel H,Garibotto V,Law I,Morbelli S,van de Giessen E,Agosta F,Barkhof F,Brooks DJ,Carrillo MC,Dubois B,Fjell AM,Frisoni GB,Hansson O,Herholz K,Hutton BF,Jack CR Jr,Lammertsma AA,Landau SM,Minoshima S,Nobili F,Nordberg A,Ossenkoppele R,Oyen WJG,Perani D,Rabinovici GD,Scheltens P,Villemagne VL,Zetterberg H,Drzezga A, Amyloid-PET and {sup}18{/sup}F-FDG-PET in the diagnostic investigation of Alzheimer's disease and other dementias. The Lancet. Neurology. 2020 Nov;
[PubMed PMID: 33098804]
[16]
Librizzi D, Cabanel N, Zavorotnyy M, Riehl E, Kircher T, Luster M, Hooshyar Yousefi B. Clinical Relevance of [(18)F]Florbetaben and [(18)F]FDG PET/CT Imaging on the Management of Patients with Dementia. Molecules (Basel, Switzerland). 2021 Feb 26:26(5):. doi: 10.3390/molecules26051282. Epub 2021 Feb 26
[PubMed PMID: 33652938]
[17]
Blazhenets G, Frings L, Ma Y, Sörensen A, Eidelberg D, Wiltfang J, Meyer PT, Alzheimer's Disease Neuroimaging Initiative. Validation of the Alzheimer Disease Dementia Conversion-Related Pattern as an ATN Biomarker of Neurodegeneration. Neurology. 2021 Mar 2:96(9):e1358-e1368. doi: 10.1212/WNL.0000000000011521. Epub 2021 Jan 6
[PubMed PMID: 33408150]
Level 1 (high-level) evidence
[18]
Scheltens P, De Strooper B, Kivipelto M, Holstege H, Chételat G, Teunissen CE, Cummings J, van der Flier WM. Alzheimer's disease. Lancet (London, England). 2021 Apr 24:397(10284):1577-1590. doi: 10.1016/S0140-6736(20)32205-4. Epub 2021 Mar 2
[PubMed PMID: 33667416]
[19]
Minoshima S,Drzezga AE,Barthel H,Bohnen N,Djekidel M,Lewis DH,Mathis CA,McConathy J,Nordberg A,Sabri O,Seibyl JP,Stokes MK,Van Laere K, SNMMI Procedure Standard/EANM Practice Guideline for Amyloid PET Imaging of the Brain 1.0. Journal of nuclear medicine : official publication, Society of Nuclear Medicine. 2016 Aug
[PubMed PMID: 27481605]
Level 1 (high-level) evidence
[20]
Cecchin D, Garibotto V, Law I, Goffin K. PET Imaging in Neurodegeneration and Neuro-oncology: Variants and Pitfalls. Seminars in nuclear medicine. 2021 Sep:51(5):408-418. doi: 10.1053/j.semnuclmed.2021.03.003. Epub 2021 Apr 3
[PubMed PMID: 33820651]
[21]
Yap SY, Frias B, Wren MC, Schöll M, Fox NC, Årstad E, Lashley T, Sander K. Discriminatory ability of next-generation tau PET tracers for Alzheimer's disease. Brain : a journal of neurology. 2021 Sep 4:144(8):2284-2290. doi: 10.1093/brain/awab120. Epub
[PubMed PMID: 33742656]
[22]
Ashton NJ,Leuzy A,Karikari TK,Mattsson-Carlgren N,Dodich A,Boccardi M,Corre J,Drzezga A,Nordberg A,Ossenkoppele R,Zetterberg H,Blennow K,Frisoni GB,Garibotto V,Hansson O, The validation status of blood biomarkers of amyloid and phospho-tau assessed with the 5-phase development framework for AD biomarkers. European journal of nuclear medicine and molecular imaging. 2021 Jul
[PubMed PMID: 33677733]
Level 1 (high-level) evidence
[23]
Leuzy A, Chiotis K, Lemoine L, Gillberg PG, Almkvist O, Rodriguez-Vieitez E, Nordberg A. Tau PET imaging in neurodegenerative tauopathies-still a challenge. Molecular psychiatry. 2019 Aug:24(8):1112-1134. doi: 10.1038/s41380-018-0342-8. Epub 2019 Jan 11
[PubMed PMID: 30635637]
[24]
Bastin C, Bahri MA, Bernard C, Hustinx R, Salmon E. Frontal hypometabolism in neurocognitive disorder with behavioral disturbance. Journal of nuclear medicine : official publication, Society of Nuclear Medicine. 2021 Mar 31:62(12):1783-8. doi: 10.2967/jnumed.120.260497. Epub 2021 Mar 31
[PubMed PMID: 33789936]
[25]
Dev SI, Dickerson BC, Touroutoglou A. Neuroimaging in Frontotemporal Lobar Degeneration: Research and Clinical Utility. Advances in experimental medicine and biology. 2021:1281():93-112. doi: 10.1007/978-3-030-51140-1_7. Epub
[PubMed PMID: 33433871]
Level 3 (low-level) evidence
[26]
Rabinovici GD, Gatsonis C, Apgar C, Chaudhary K, Gareen I, Hanna L, Hendrix J, Hillner BE, Olson C, Lesman-Segev OH, Romanoff J, Siegel BA, Whitmer RA, Carrillo MC. Association of Amyloid Positron Emission Tomography With Subsequent Change in Clinical Management Among Medicare Beneficiaries With Mild Cognitive Impairment or Dementia. JAMA. 2019 Apr 2:321(13):1286-1294. doi: 10.1001/jama.2019.2000. Epub
[PubMed PMID: 30938796]
[27]
Sood A, Shukla J, Shree R, Vatsa R, Modi M, Mittal BR. Comparative Performance of 99mTc-TRODAT-1 SPECT/CT and 18F-FDOPA PET/CT Imaging in Patients With Parkinson's Disease, Parkinson-Plus Syndrome, and Essential Tremor. Clinical nuclear medicine. 2021 Feb 1:46(2):95-102. doi: 10.1097/RLU.0000000000003409. Epub
[PubMed PMID: 33234920]
Level 2 (mid-level) evidence
[28]
Boertien JM, van der Zee S, Chrysou A, Gerritsen MJJ, Jansonius NM, Spikman JM, van Laar T, PPNN Study Group. Study protocol of the DUtch PARkinson Cohort (DUPARC): a prospective, observational study of de novo Parkinson's disease patients for the identification and validation of biomarkers for Parkinson's disease subtypes, progression and pathophysiology. BMC neurology. 2020 Jun 13:20(1):245. doi: 10.1186/s12883-020-01811-3. Epub 2020 Jun 13
[PubMed PMID: 32534583]
Level 2 (mid-level) evidence
[29]
Stormezand GN,Chaves LT,Vállez García D,Doorduin J,De Jong BM,Leenders KL,Kremer BPH,Dierckx RAJO, Intrastriatal gradient analyses of 18F-FDOPA PET scans for differentiation of Parkinsonian disorders. NeuroImage. Clinical. 2020
[PubMed PMID: 31981888]
[30]
Darcourt J, Schiazza A, Sapin N, Dufour M, Ouvrier MJ, Benisvy D, Fontana X, Koulibaly PM. 18F-FDOPA PET for the diagnosis of parkinsonian syndromes. The quarterly journal of nuclear medicine and molecular imaging : official publication of the Italian Association of Nuclear Medicine (AIMN) [and] the International Association of Radiopharmacology (IAR), [and] Section of the Society of.... 2014 Dec:58(4):355-65
[PubMed PMID: 25366711]
[31]
Louarn N, Kauv P, Capelle L, Mokhtari K, Itti E. Illustration of the Added Value of 18F-DOPA PET to Multimodal MRI to Distinguish Low- and High-Grade Gliomas. Clinical nuclear medicine. 2021 Jul 1:46(7):e353-e354. doi: 10.1097/RLU.0000000000003507. Epub
[PubMed PMID: 33577196]
[32]
Law I, Albert NL, Arbizu J, Boellaard R, Drzezga A, Galldiks N, la Fougère C, Langen KJ, Lopci E, Lowe V, McConathy J, Quick HH, Sattler B, Schuster DM, Tonn JC, Weller M. Joint EANM/EANO/RANO practice guidelines/SNMMI procedure standards for imaging of gliomas using PET with radiolabelled amino acids and [(18)F]FDG: version 1.0. European journal of nuclear medicine and molecular imaging. 2019 Mar:46(3):540-557. doi: 10.1007/s00259-018-4207-9. Epub 2018 Dec 5
[PubMed PMID: 30519867]
Level 1 (high-level) evidence
[33]
Marcus C, Feizi P, Hogg J, Summerfield H, Castellani R, Sriwastava S, Marano GD. Imaging in Differentiating Cerebral Toxoplasmosis and Primary CNS Lymphoma With Special Focus on FDG PET/CT. AJR. American journal of roentgenology. 2021 Jan:216(1):157-164. doi: 10.2214/AJR.19.22629. Epub 2020 Oct 28
[PubMed PMID: 33112669]
[34]
Zhang Y, Cai J, Lin Z, Yao S, Miao W. Primary Central Nervous System Lymphoma Revealed by 68Ga-FAPI and 18F-FDG PET/CT. Clinical nuclear medicine. 2021 Aug 1:46(8):e421-e423. doi: 10.1097/RLU.0000000000003517. Epub
[PubMed PMID: 33512949]
[35]
Djekidel M. (18)F-FDG PET Imaging Predicts the Epileptogenic Zone Prospectively in Recurrent Cryptogenic Meningoencephalitis with Subsequent Simple Partial Visual Seizures. Journal of nuclear medicine technology. 2021 Mar:49(1):92-94. doi: 10.2967/jnmt.120.252866. Epub 2020 Nov 20
[PubMed PMID: 33219155]
[36]
Avendaño-Estrada A, Velasco F, Velasco AL, Cuellar-Herrera M, Saucedo-Alvarado PE, Marquez-Franco R, Rivera-Bravo B, Ávila-Rodríguez MA. Quantitative Analysis of [18F]FFMZ and [18F]FDG PET Studies in the Localization of Seizure Onset Zone in Drug-Resistant Temporal Lobe Epilepsy. Stereotactic and functional neurosurgery. 2019:97(4):232-240. doi: 10.1159/000503692. Epub 2019 Nov 13
[PubMed PMID: 31722358]
[37]
Tomás J, Pittau F, Hammers A, Bouvard S, Picard F, Vargas MI, Sales F, Seeck M, Garibotto V. The predictive value of hypometabolism in focal epilepsy: a prospective study in surgical candidates. European journal of nuclear medicine and molecular imaging. 2019 Aug:46(9):1806-1816. doi: 10.1007/s00259-019-04356-x. Epub 2019 May 29
[PubMed PMID: 31144060]
[38]
Solnes LB, Jones KM, Rowe SP, Pattanayak P, Nalluri A, Venkatesan A, Probasco JC, Javadi MS. Diagnostic Value of (18)F-FDG PET/CT Versus MRI in the Setting of Antibody-Specific Autoimmune Encephalitis. Journal of nuclear medicine : official publication, Society of Nuclear Medicine. 2017 Aug:58(8):1307-1313. doi: 10.2967/jnumed.116.184333. Epub 2017 Feb 16
[PubMed PMID: 28209905]
[39]
Bordonne M, Chawki MB, Doyen M, Kas A, Guedj E, Tyvaert L, Verger A. Brain (18)F-FDG PET for the diagnosis of autoimmune encephalitis: a systematic review and a meta-analysis. European journal of nuclear medicine and molecular imaging. 2021 Nov:48(12):3847-3858. doi: 10.1007/s00259-021-05299-y. Epub 2021 Mar 7
[PubMed PMID: 33677643]
Level 1 (high-level) evidence
[40]
Ge J, Deng B, Guan Y, Bao W, Wu P, Chen X, Zuo C. Distinct cerebral (18)F-FDG PET metabolic patterns in anti-N-methyl-D-aspartate receptor encephalitis patients with different trigger factors. Therapeutic advances in neurological disorders. 2021:14():1756286421995635. doi: 10.1177/1756286421995635. Epub 2021 Feb 24
[PubMed PMID: 33717212]
Level 3 (low-level) evidence
[41]
Liu X, Shan W, Zhao X, Ren J, Ren G, Chen C, Shi W, Lv R, Li Z, Liu Y, Ai L, Wang Q. The Clinical Value of (18) F-FDG-PET in Autoimmune Encephalitis Associated With LGI1 Antibody. Frontiers in neurology. 2020:11():418. doi: 10.3389/fneur.2020.00418. Epub 2020 Jun 5
[PubMed PMID: 32581996]
[42]
Seniaray N, Verma R, Ranjan R, Belho E, Mahajan H. 18F-FDG PET/CT in Initial Diagnosis and Treatment Response Evaluation of Anti-NMDAr and Anti-GAD Dual Antibody Autoimmune Encephalitis. Clinical nuclear medicine. 2021 Jan:46(1):e63-e64. doi: 10.1097/RLU.0000000000003379. Epub
[PubMed PMID: 33181746]
[43]
Seniaray N, Verma R, Ranjan R, Belho E, Mahajan H. Metabolic Imaging Patterns on 18F-FDG PET in Acute and Subacute LGI1 Autoimmune Limbic Encephalitis. Clinical nuclear medicine. 2021 Jan:46(1):e27-e28. doi: 10.1097/RLU.0000000000003258. Epub
[PubMed PMID: 32910055]
[44]
Wei YC, Tseng JR, Wu CL, Su FC, Weng WC, Hsu CC, Chang KH, Wu CF, Hsiao IT, Lin CP. Different FDG-PET metabolic patterns of anti-AMPAR and anti-NMDAR encephalitis: Case report and literature review. Brain and behavior. 2020 Mar:10(3):e01540. doi: 10.1002/brb3.1540. Epub 2020 Jan 27
[PubMed PMID: 31985135]
Level 3 (low-level) evidence