Learning Outcome
- Describe the cause of hypothermia
- List the complications of hypothermia
- Recall the general management of hypothermia
- Summarize the nurse's role in managing hypothermic patients

Hypothermia is defined as an involuntary drop in body temperature below 35C. Symptoms will vary based on the severity of hypothermia. Hypothermia can be further defined based on core temperature as mild (32-35C), moderate (28-32C), severe (<28C), with some experts also categorizing certain individuals with profound (<24C) hypothermia. More severe symptoms and morbidity/mortality are associated with worsening degrees of hypothermia. Primary hypothermia occurs when a person is unable to maintain adequate heat production due to overwhelimg cold stress. Death from exposure and accidental hypothermia is not limited to regions/times of severe cold and can occur in milder climates/temperatures even occurring during summer months.
Hypothermia occurs as a results of the body dissipating more heat than it absorbs/creates leaving the body unable to generate sufficient heat to maintain an adequate temperature to maintain proper function. Many factors play a role in the development of hypothermia. While the underlying cause of accidental hypothermia is excessive cold stress and inadequate heat generation from the body (thermogenesis) there are other factors that increase one’s risk of developing hypothermia. Risk factors include extremes of age, mental disability/disease, malnutrition, dehydration, alcohol abuse, excessive exertion, certain medications, co-morbid medical conditions (ie: hypothyroidism, CV disease, Parkinson’s). Prolonged or intense exposure and co-existing weather conditions can also increase the risk of developing hypothermia.
Each year there are approximately 1500 patients in the United States who have hypothermia noted on their death certificates. The true incidence of hypothermia and associated morbidity and mortality is unknown but even with supportive in-hospital care the mortality of those with moderate to severe hypothermia still approaches 40 percent.
Those suffering from accidental hypothermia will normally have a history of cold exposure. Obtaining a temperature is important to effectively diagnosis and manage hypothermia. Oral temperature is only useful to rule out hypothermia as most commercially available thermometers cannot read under 35C. Tympanic thermometers are also unreliable and not recommended. Epitympanic thermometers when used properly reflect the carotid artery temperature and when done properly with the soft probe near tympanic membrane and ear canal insulated from environment can be fairly reliable. Both rectal and bladder temperature measurement are reasonable in conscious individuals with mild to moderate hypothermia but should not be used in critical patients during rewarming as they lag behind true core temperature. Neither should be performed in the pre-hospital setting as doing so may further expose the patient and cause further drops in temperature. Esophageal temperature measurement is the most accurate when done properly with the probe in the lower 1/3 of the esophagus, but should only be performed in patients with an advanced airway in place. Given the difficulty to get an immediate reliable temperature in a pre-hospital setting, it is important to know the clinical findings associated with the stages of hypothermia so that appropriate treatment can be started immediately.
Mild Hypothermia 32-35C: Presentation can often be subtle with vague symptoms such as hunger, nausea, fatigue, shivering, and pale/cold/dry skin. Often will have increased muscle tone, increased blood pressure, tachycardia, and tachypnea from body’s attempts to promote thermogenesis. Patients are often shivering, but if energy stores have been depleted they may not be shivering meaning you cannot rely on this finding. Will often have decline in cognitive abilities, memory, and judgment with some experiencing ataxia and dysarthria. May experience “cold diuresis” due to peripheral vasoconstriction leading to increased central fluid volume resulting in increased diuresis despite that they may be volume depleted.
Moderate Hypothermia 28-32C: Patient will continue to have a cognitive decline and may be stuporous. Increased CNS depression may lead to hypo-reflexia with pupils less responsive and dilated. Will have a reduction in heart rate and respiratory rate with possible bradycardia and bradypnea. May be hypotensive. Shivering typically ceases between 30-32C and paradoxical undressing may be observed. Susceptibility to dysrhythmias increases with atrial fibrillation being the most common.
Severe Hypothermia <28C: Cognition continues to decline, usually unconscious and may have areflexia. Increasing hypotension and bradypnea. Usually bradycardic but have an increased risk for ventricular arrhythmias and asystole. Due to the difficulty a provider may have palpating a pulse due to decreaed tactile sensation from ambient cold temperature and due to bradycardia and vasocontriction of a hypohermic individual it is reccomended to check for a pulse for a full minute, and preferably a central pulse using continuous wave Doppler, prior to declaring the patient pulseless and initating CPR.
All patients with suspected hypothermia should have a complete physical exam to exclude local cold-induced injuries and to assess for signs of trauma or other illness that may have caused their exposure to the cold. Also be aware of vital signs inconsistent with the degree of hypothermia as this may be the only clue to an alternate diagnosis such as hypothyroidism, adrenal insufficiency, sepsis, hypoglycemia, carbon monoxide poisoning, alcohol abuse, malnutrition, overdose.
After diagnosis of hypothermia is made, laboratory and possible imaging evaluation should take place to help identify potential comorbidities or medical events that may have led to the patient becoming hypothermic. Standard laboratory evaluation should include finger-stick glucose, complete blood count, metabolic panel with basic serum electrolytes and BUN/Cr. One may expect the hemoglobin/hematocrit to be increased in hypothermic patients due to cold diuresis. No significant electrolyte abnormalities are consistent in hypothermia but rewarming can result in rapid changes in concentrations and it is recommended to reassess electrolytes approximately every 4 hours when resuscitating the moderate to severely hypothermic patient. Glucose also does not follow a specific pattern but may be the earliest clue for a patient in DKA.
In moderate to severe hypothermic patients in whom invasive procedures may be performed reasonable to get a coagulation panel. Despite the fact that the patient may have an obvious bleeding diathesis this test may return as normal as it is always performed at 37C. If patient is in respiratory distress or intubated an ABG uncorrected for temperature to help guide resuscitation. Under the right clinical settings may also consider serum lactate, creatinine kinase, troponin, TSH, cortisol, toxicology screen, fibrinogen, lipase, magnesium, and any other labs deemed necessary per the clinical scenario.
Imaging should be dictated by clinical scenario as some patients may have experienced trauma, cerebrovascular accident, or other events that led to prolonged cold exposure. If CXR is obtained it is not uncommon for severely hypothermic patients to show signs of pulmonary edema.
Due to the different dysthymias often exhibited by hypothermic patients and ECG should be obtained. Hypothermia can cause slowed impulses conduction through potassium channels resulting in prolonged ECG intervals. There may also be an elevated J point which can produce an Osborne or J wave. The height of this wave is proportional to the degree of hypothermia and is most common in the precordial leads. Any dysrhythmia is possible with atrial fibrillation being the most common. Those with more moderate to severe hypothermia will likely exhibit bradycardia and are at increased risk for ventricular arrhythmias and care should be taken to not jostle the patient due to the increased irritability of the myocardium.
The management and treatment of accidental hypothermia revolves around prevention of further heat loss and initiation or rewarming but also requires evaluation and support/intervention of airway, breathing, and circulation. This may involve patent rescue with the first priority being rescuer safety. Wet clothing should be removed and replaced with dry clothing or insulation as soon as possible to prevent further heat loss.
Once able one should then attempt to determine the degree of hypothermia based on history, mental status, exam, and temperature if able/appropriate to help guide treatment. If there is suspicion for moderate or severe hypothermia, especially in those with decreased level of consciousness or in those have an irregular or faint pulse, extra care should be taken to not move or jostle to patient too much as his may precipitate cardiac collapse into a fatal arrhythmia due to increased cardiac irritability. Considerations and appropriate treatment must also be given to comorbid medical conditions and trauma that may have occurred.
Rewarming of hypothermic patients involve passive external rewarming, active external rewarming, active internal rewarming, or a combination of these techniques. The treatment of choice for mild hypothermia is passive external rewarming. After wet clothing is removed, additional layers of insulation are placed on/over the patient with the goal to prevent heat loss and promote retention of heat produced by patient. Success of this method requires adequate glucose/glycogen stores so that a patient can produce heat, given that at this point many will have depleted energy reserves (more so in elderly, young, and malnournished) it is appropriate to supply glucose to these individuals, orally when possible. In individuals with mild hypothermia it is recommended to warm them at 0.5-2C per hour. If the patient fails to respond to passive techniques it is appropriate to progress to active external rewarming techniques.
Active external rewarming is indicated for moderate to severe hypothermia and in some cases of mild hypothermia not responding to standard measures or when there is worry patient is at risk for decompensation.
involving addition of more insulating layers, application of heat to the axillae, chest, back (in that order) using heat pads/blankets, Bair hugger (forced warm air), blankets and garments with circulating warm fluids. Wet clothing should be removed prior to this. Warm water bottles and heat packs may also be used but one should avoid placing heat source directly on skin due to decreased peripheral sensation raising the risk of iatrogenic burns. Heated humidified oxygen may also be used. Immersion of extremities in warm water (44-45C) may be undertaken with great care and attention as efforts to rewarm patients may precipitate increases CV load and collapse as peripheral vasodilation this may lead to an after-drop cooling of core temperature from sudden return of cold blood from the extremities. Due to the amount of energy expended by the body trying to maintain adequate temperature it is also appropriate to administer calories to patients in either IV or oral form. Even mildly hypothermic individuals can have significant hypovolemia from effect of cold diuresis and benefit from IV Fluids. If
Normothermic with stable vital signs
No sign of end organ injury
Hypothermia is potentially lethal if not quickly recognized and treated. The majority of patients first present to the emergency department, and the triage nurse should promptly accept the patient and inform the emergency department physicians. In general, treating patients with hypothermia requires an interprofessional team of healthcare professionals.
EMS personnel provide the initial encounter and resuscitation effort. They will remove wet clothing and initiate external passive rewarming. After reaching the hospital, nurses and emergency room physicians will work together to further warm the patient with external and internal invasive rewarming methods.
Hypothermic patients are prone to many complications and require admission to the ICU, where there will be continuous monitoring by the nurses. The pulmonologist and cardiologist should be involved if the patient has pulmonary edema or aspiration pneumonia. Since frostbite is a common outcome, wound care must take part in therapy. Regular debridement of the wound may be necessary. Blood work requires monitoring for rhabdomyolysis. Nursing must remain in attendance constantly and report any deterioration in condition to the physician staff, as well as administering fluids and any medications.
Nephrologists, surgeons, and cardiology may be required if ECMO, hemodialysis, or cardiopulmonary bypass is needed.[1]
Hypothermia is a medical emergency and requires an interprofessional team approach, including physicians, specialists, specialty-trained nurses, and pharmacists, all collaborating across disciplines to achieve optimal patient results. [Level V]
For those who survive, education is necessary to prevent a repeat episode. These individuals should avoid alcohol, dress appropriately, and carry a survival bag with the essential equipment and material to protect the body. Only through an interprofessional team approach can be morbidity of hypothermia be lowered.
Outcomes
Patients who receive rapid resuscitation usually have good results but residual frostbite and muscle injury may be present. Outcomes are worst for the very young and elderly.
Hypothermia occurs when your body can no longer produce enough heat to overcome cold exposure. Hypothermia is an extremely dangerous entity that has the potential to lead to death if not treated quickly. Luckily, hypothermia can be avoided. Do not stay outside too long if the weather is cold. If you’re outside during this arduous climate, proper clothing is key. If your clothes are wet, quickly change out of them.
Certain patient populations are at a higher risk of developing hypothermia. Infants and young children are at greater risk due to their underdeveloped bodies and their inability to communicate reliably. On the other end of the age spectrum, the elderly are also at greater risk. They tend to have multiple comorbidities. Physical and cognitive limitations could prevent them from seeking warmer environments in certain situations.
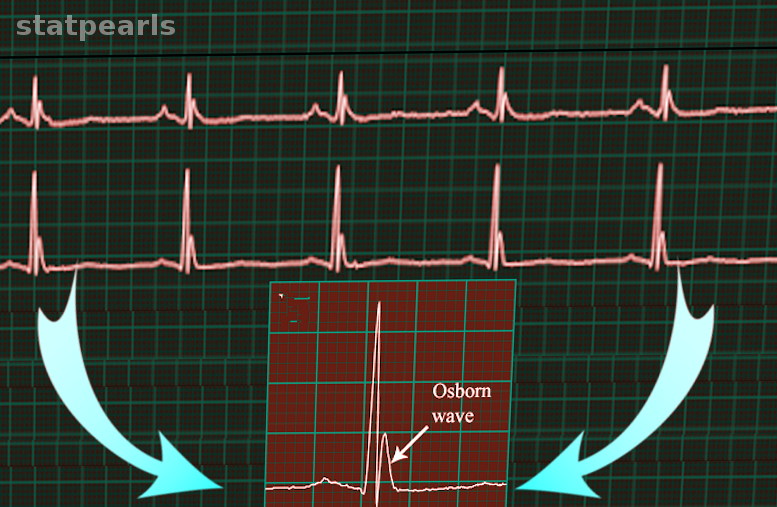
Osborn Wave On Electrocardiography. This electrocardiogram (ECG) strip shows Osborn waves.
Image courtesy S. Bhimji MD
Kempainen RR, Brunette DD. The evaluation and management of accidental hypothermia. Respiratory care. 2004 Feb:49(2):192-205 [PubMed PMID: 14744270]
Brychta RJ, Chen KY. Cold-induced thermogenesis in humans. European journal of clinical nutrition. 2017 Mar:71(3):345-352. doi: 10.1038/ejcn.2016.223. Epub 2016 Nov 23 [PubMed PMID: 27876809]
Durrer B, Brugger H, Syme D, International Commission for Mountain Emergency Medicine. The medical on-site treatment of hypothermia: ICAR-MEDCOM recommendation. High altitude medicine & biology. 2003 Spring:4(1):99-103 [PubMed PMID: 12713717]
Petrone P, Asensio JA, Marini CP. In brief: Hypothermia. Current problems in surgery. 2014 Oct:51(10):414-5. doi: 10.1067/j.cpsurg.2014.07.005. Epub 2014 Jul 29 [PubMed PMID: 25242453]
Paal P, Pasquier M, Darocha T, Lechner R, Kosinski S, Wallner B, Zafren K, Brugger H. Accidental Hypothermia: 2021 Update. International journal of environmental research and public health. 2022 Jan 3:19(1):. doi: 10.3390/ijerph19010501. Epub 2022 Jan 3 [PubMed PMID: 35010760]
Epstein E, Anna K. Accidental hypothermia. BMJ (Clinical research ed.). 2006 Mar 25:332(7543):706-9 [PubMed PMID: 16565126]
Paal P, Brugger H, Strapazzon G. Accidental hypothermia. Handbook of clinical neurology. 2018:157():547-563. doi: 10.1016/B978-0-444-64074-1.00033-1. Epub [PubMed PMID: 30459025]
Petrone P, Asensio JA, Marini CP. Management of accidental hypothermia and cold injury. Current problems in surgery. 2014 Oct:51(10):417-31. doi: 10.1067/j.cpsurg.2014.07.004. Epub 2014 Jul 29 [PubMed PMID: 25242454]
Davis PR, Byers M. Accidental hypothermia. Journal of the Royal Army Medical Corps. 2005 Dec:151(4):223-33 [PubMed PMID: 16548338]
Zafren K. Out-of-Hospital Evaluation and Treatment of Accidental Hypothermia. Emergency medicine clinics of North America. 2017 May:35(2):261-279. doi: 10.1016/j.emc.2017.01.003. Epub [PubMed PMID: 28411927]
Danzl DF, Pozos RS. Accidental hypothermia. The New England journal of medicine. 1994 Dec 29:331(26):1756-60 [PubMed PMID: 7984198]
Dow J, Giesbrecht GG, Danzl DF, Brugger H, Sagalyn EB, Walpoth B, Auerbach PS, McIntosh SE, Némethy M, McDevitt M, Schoene RB, Rodway GW, Hackett PH, Zafren K, Bennett BL, Grissom CK. Wilderness Medical Society Clinical Practice Guidelines for the Out-of-Hospital Evaluation and Treatment of Accidental Hypothermia: 2019 Update. Wilderness & environmental medicine. 2019 Dec:30(4S):S47-S69. doi: 10.1016/j.wem.2019.10.002. Epub 2019 Nov 15 [PubMed PMID: 31740369]
Lloyd EL. Accidental hypothermia. Resuscitation. 1996 Sep:32(2):111-24 [PubMed PMID: 8896051]
Haverkamp FJC, Giesbrecht GG, Tan ECTH. The prehospital management of hypothermia - An up-to-date overview. Injury. 2018 Feb:49(2):149-164. doi: 10.1016/j.injury.2017.11.001. Epub 2017 Nov 4 [PubMed PMID: 29162267]
Avellanas Chavala ML, Ayala Gallardo M, Soteras Martínez Í, Subirats Bayego E. Management of accidental hypothermia: A narrative review. Medicina intensiva. 2019 Dec:43(9):556-568. doi: 10.1016/j.medin.2018.11.008. Epub 2019 Jan 22 [PubMed PMID: 30683520]
Smith TM, Berk AS, Upadhyay H. Severe hypothermia in a patient with spinal cord injury without radiological abnormality. Journal of emergencies, trauma, and shock. 2011 Jul:4(3):421-4. doi: 10.4103/0974-2700.83878. Epub [PubMed PMID: 21887040]
Lloyd EL. Treatment of accidental hypothermia with the Clinitron bed. Anaesthesia. 1987 Oct:42(10):1121-2 [PubMed PMID: 3688406]
van Veelen MJ, Brodmann Maeder M. Hypothermia in Trauma. International journal of environmental research and public health. 2021 Aug 18:18(16):. doi: 10.3390/ijerph18168719. Epub 2021 Aug 18 [PubMed PMID: 34444466]
Brown DJ, Brugger H, Boyd J, Paal P. Accidental hypothermia. The New England journal of medicine. 2012 Nov 15:367(20):1930-8. doi: 10.1056/NEJMra1114208. Epub [PubMed PMID: 23150960]
Kakizaki R, Bunya N, Uemura S, Odagiri A, Kasai T, Narimatsu E. Takotsubo cardiomyopathy developed during rewarming of accidental hypothermia with extracorporeal membrane oxygenation. Acute medicine & surgery. 2019 Apr:6(2):201-205. doi: 10.1002/ams2.399. Epub 2019 Mar 1 [PubMed PMID: 30976450]
Kirkegaard H, Grejs AM, Gudbjerg S, Duez C, Jeppesen A, Hassager C, Laitio T, Storm C, Taccone FS, Skrifvars MB, Søreide E. Electrolyte profiles with induced hypothermia: A sub study of a clinical trial evaluating the duration of hypothermia after cardiac arrest. Acta anaesthesiologica Scandinavica. 2022 May:66(5):615-624. doi: 10.1111/aas.14053. Epub 2022 Mar 28 [PubMed PMID: 35218019]
Polderman KH, Peerdeman SM, Girbes AR. Hypophosphatemia and hypomagnesemia induced by cooling in patients with severe head injury. Journal of neurosurgery. 2001 May:94(5):697-705 [PubMed PMID: 11354399]
Metz C, Holzschuh M, Bein T, Woertgen C, Frey A, Frey I, Taeger K, Brawanski A. Moderate hypothermia in patients with severe head injury: cerebral and extracerebral effects. Journal of neurosurgery. 1996 Oct:85(4):533-41 [PubMed PMID: 8814152]
Escolar JC, Hoo-Paris R, Castex C, Sutter BC. Effect of low temperatures on glucose-induced insulin secretion and glucose metabolism in isolated pancreatic islets of the rat. The Journal of endocrinology. 1990 Apr:125(1):45-51 [PubMed PMID: 2187049]