Learning Outcome
- List the risk factors for glaucoma
- Describe the presentation of glaucoma
- Summarize the treatment of glaucoma
- Recall the nursing management of a patient with glaucoma

Glaucoma is the second leading cause of permanent blindness in the United States and occurs most often in older adults.[1] There are four general categories of adult glaucoma: primary open-angle and angle-closure, and the secondary open and angle closure glaucoma. The most common type in the United States is primary, open-angle glaucoma (POAG).[1] Glaucoma is defined as an acquired loss of retinal ganglion cells and axons within the optic nerve or optic neuropathy, that results in a characteristic optic nerve head appearance and a corresponding progressive loss of vision. This pattern of peripheral loss of vision can also be a distinguishing characteristic from other forms of vision loss.[2]
The patient with POAG is often asymptomatic until the optic nerve damage is severe unless signs of early glaucoma are recognized on a routine eye exam. Acute angle-closure glaucoma, in contrast, can develop suddenly and result in a more rapid decline in vision with associated corneal edema, eye pain, headache, nausea, and emesis. Secondary glaucoma is usually correlated with a prior eye injury or disease state causing elevated intraocular pressure (IOP) and related optic neuropathy. The last type is normal or low-tension type glaucoma in which patients have the same visual loss pattern as POAG but at normal intraocular pressure readings.
While there are congenital, infantile, development glaucomas, and a juvenile variant of POAG, the four previously mentioned glaucoma types typically occur in people over the age of 40. The cause is generally correlated with increased intraocular pressure, though it has not been proven to have a direct cause-and-effect relationship. There may also be a genetic component to the development of glaucoma. Monozygotic twin pairs have a higher percentage of concordance, but not pairs, which suggests that environmental factors also influence the development of the disease.[3] Currently, glaucoma cannot be prevented or cured, but progression can be controlled to help prevent further vision loss either through medication, glaucoma laser treatment, or incisional glaucoma surgeries.
Currently, the exact etiology of glaucoma is unknown but there is a clear correlation with elevated eye pressures in the majority of POAG cases. Open-angle glaucoma typically manifests as a slow painless damage to the optic nerve that is thought to be due to the drainage system in the eye becoming ineffective. In glaucoma, the resistance to drainage of aqueous humor most commonly starts at the inner wall of Schlemm’s canal at the juxtacanalicular trabecular meshwork. The decreased outflow facility, or increased resistance to outflow of aqueous results in the gradual elevation of IOP and a characteristic damage pattern to the optic nerve ganglion cell nerve fiber layer. Another theory is that the increased IOP causes decreased blood flow to the optic nerve fibers which leads to subtle ischemic damage. Either way, POAG patients often have elevated intraocular pressure (IOP) readings that seem to correlate with characteristic optic nerve damage patterns. As the disease progresses, there is a slow loss of peripheral vision in both eyes; eventually leading to loss of central vision if left undetected or untreated. It is because of this pattern of loss that affected persons do not notice a change in their vision until their loss is advanced and affecting the central vision. [2]
There are a couple subsets of open-angle glaucoma which are Juvenile open-angle glaucoma and low-tension/normal-tension glaucoma. Juvenile open-angle glaucoma affects patients between the ages of 5-35 years old. It is uncommon and tends to be found later in the disease process because its early but gradual IOP elevation. Patients also typically present with eye pressures greater than 30 mm Hg. Juvenile open-angle is thought to follow the same process of increased IOP leading to optic neuropathy as POAG, just in a younger patient population.[4]
Low-tension or normal-tension glaucoma resembles POAG as there is the characteristic optic disc cupping and peripheral visual-field loss finding but the IOP readings are consistently less than 21 mm Hg. Theories include having an abnormally pressure-sensitive optic nerve or intermittent ischemic change due to atherosclerosis/vascular insufficiency.[5] There appears to be a higher prevalence of vasospastic disorders such as migraines, Raynaud phenomenon, autoimmune diseases, ischemic vascular diseases and coagulopathies seen in these patients which may suggest a vascular autoregulatory defect playing a role in the pathogenesis of the disease. [5] Normal tension also tends to have a greater frequency of nerve fiber layer hemorrhages and a neuroretinal rim that is thinner inferiorly and inferotemporally than those with open-angle type. Visual field defects are more focal, deeper, and closer to fixation rather than the classic arcuate scotoma pattern in open-angle. [5]
Angle-closure is the type of glaucoma that can present as a medical emergency in the acute setting. This occurs when the drainage system of the eye becomes blocked abruptly due to the closure of the angle formed between the cornea and the iris. Typically, this occurs due to an age-related thickening of the lens, causing the gradual increase in a relative pupillary block which then pushes the iris anteriorly. This anteriorly displaced iris along with a natural anatomical variation of a smaller angle, as seen in far-sightedness or in certain ethnic groups, allows for easier blockage of the outflow tract. A pupillary block is considered to be the underlying cause of more than 90% of cases. When sudden pupil dilation occurs due to stimulus or drugs the iris becomes thick enough in its contracted state, or anteriorly displaced by pupillary block, to block the drainage of fluid via the trabecular meshwork. The pressure then rapidly increases within the eye. It is this rapid change in intraocular pressure that can cause vision loss to occur within a day of onset without intervention, due to retinal vascular occlusion, ischemic optic neuropathy, or glaucomatous optic nerve damage. However, only about 10% of glaucoma cases are this acute angle closure type.[6]
Angle-closure glaucoma can occur secondary to another cause. One such cause is lens subluxation in Marfan’s syndrome.[7] The lens can displace into the pupil or anterior chamber causing an acute pupillary block. Plateau iris can also cause an acute pupillary block, and a chronic angle closure, due to elongated or anteriorly positioned ciliary processes that push the edges of the iris forward.[8] In Iridocorneal endothelial syndrome, the corneal endothelium is irregular and can migrate onto the trabecular meshwork and peripheral iris. This creates a contraction causing high peripheral anterior synechiae which can close the angle, preventing outflow.[9] Neovascularization can cause closure of the angle by creating a fibrovascular membrane that flattens the iris and displaces it anteriorly and causing total synechial closure of the angle.[10] Angle-closure can occur after ophthalmic surgery due to ciliary body edema, scleral buckle placement, fibrin deposition, gas, or silicone oil like that used in retinal surgery.[11] Sulfa drugs such as topiramate can induce angle closure due to ciliochoroidal effusion that compresses the lens-iris diaphragm, displacing it anteriorly, thus closing off the angle.[12]
Secondary open angle type is due to injury, eye disease and rarely eye surgery causing increased intraocular pressure and therefore optic nerve damage like the open-angle form of glaucoma. One mechanism is from laser surgery which can cause pigment release, inflammatory cells, debris, and mechanical deformation resulting in blockage of the trabecular meshwork leading to increased intraocular pressure. The most common mechanism for secondary type is from diseases causing neovascularization. Neovascularization can either physically block the outflow tracts.[10] Pseudoexfoliative type is when flaky material peels off the outer lens capsule and collects in the angle, clogging the trabecular meshwork, leading to increased eye pressure. Pigmentary type is similar to exfoliative except the debris are pigment granules from the back of the iris that break off and clog the trabecular meshwork due to contact with the peripheral lens capsule and zonules in typically myopic, or near-sighted eyes.[13] Steroids can induce secondary glaucoma due to increased outflow resistance by the upregulation of glucocorticoid receptors on cells within the trabecular meshwork and accumulation of glycosaminoglycans in the meshwork pores. Steroids also suppress the phagocytic activity which decreases debris deposition removal from the meshwork as well as stimulates the expression of extracellular matrix proteins.[14] A carotid-cavernous fistula causes an abnormal communication between the cavernous sinus and carotid artery. This causes an arterial flow and venous engorgement leading to elevated episcleral venous pressure. It also causes a dilation of retinal veins and optic disc swelling that can concurrently damage optic nerve fibers.[15] Glaucomatocyclitic Crisis manifests as recurrent acute attacks of increased intraocular pressure that resolve without treatment but with repeated attacks, has been reported to cause glaucomatous damage to the optic nerve over time.[16][17]
Worldwide, an estimated 60 million people have optic neuropathy due to glaucoma. The African population has the highest prevalence of open-angle type. The likelihood of blindness from open-angle glaucoma is up to 15-times greater in those with African-decent compared to other population groups. [2] The highest prevalence for angle-closure is in the Inuit population and has also been shown to affect a higher rate in women than men, and in those of Asian-decent, with these groups generally having a shallower anterior chamber.[18] Normal-tension type is most prevalent in Japanese populations. Across all types, age is a major risk factor to the continual loss of retinal ganglion cells. Other risk factors for developing glaucoma include those with family history of glaucoma in a primary relative (mother, father, brother, sister, or children), medical conditions such as diabetes, high blood pressure, heart disease, eye trauma, anatomical differences such as thinner corneas, history of retinal detachment, eye tumors or inflammation, and corticosteroid use for prolonged periods of time.
Many patients with glaucoma, especially early in the disease, are not aware they have this condition until it is discovered on a routine eye exam. People generally slowly lose peripheral vision but retain central vision until the disease process is severe. This can present in a classic arcuate pattern on Humphrey visual field testing. On comprehensive eye examination, optic nerves may have a focally notched neural retinal rim or diffuse cup enlargement, a decrease in peripheral vision detected on visual field testing, and (although not required for diagnosis) an increased intraocular pressure reading on tonometry. Typically changes will be seen bilaterally but may not progress at the same rate, resulting in an asymmetric optic nerve cup. A cup to disc ratio of > 0.5 is considered suggestive for glaucoma and typically starts with a loss on the inferotemporal and superotemporal poles of the optic disc.[19]
Normal tension glaucoma patients will typically be asymptomatic and have an intraocular pressure of less than 21mm Hg. On slit lamp examination, changes in the optic disc such as increased cup to disc ratio will be seen, disc hemorrhage in the nerve fiber layer may also be present. Patients also may have a history of vasospasm, coagulopathies, nocturnal hypotension, autoimmune diseases, vascular diseases, thyroid dysfunction, or sleep apnea.
In the acute angle-closure type, patients typically present with severe sudden ocular pain, redness, blurry vision/decreased visual acuity, headache, nausea or vomiting, and may complain of seeing halos of light. Patients will have an unresponsive mid-dilated pupil on examination and a firm feeling eyeball on palpation. Typically, attacks are precipitated by pupillary dilation due to weak mydriatic, or dilating, drops. Intraocular pressure will typically be high and often in the 30-50 mm Hg range. The angle between the iris and the cornea will be around 20° or less on examination with gonioscopy and/or an anterior chamber depth of less than 2.5mm can be predisposing risk factors.[20] Patients with these findings should be warned to avoid dilating medications to reduce their risk of developing an acute attack. On slit lamp examination, a large optic cup with narrowing of the neuroretinal rim and splinter hemorrhages may also be present.[21]
Patients with Secondary glaucoma will typically have a history of recent ophthalmic procedure, trauma or health condition causing neovascularization like diabetes. However, some patients will not have a clear precipitating factor in their history but will have sometime subtle clinical exam findings pointing to the cause of the IOP elevation. On exam, findings can include exfoliative material on the anterior lens capsule, pigment deposition on corneal endothelium, cell and flare in the anterior chamber typical of uveitis, abnormal blood vessels on the iris or evidence of trauma; depending on the underlying etiology.
Evaluation is based on fundoscopic examination, visual field testing, tonometry, optical coherence tomography, and gonioscopy. Other helpful tests include visual acuity to see if vision is being affected, pachymetry to evaluate corneal thickness, and retinal scans to help monitor for progressive changes in the retinal nerve fiber layer.
Glaucoma is diagnosed based on clinical characteristic findings of a progressive optic neuropathy or visual field defects based on the testing modalities listed above. There is no single ‘gold standard’ test for the diagnosis of glaucoma. Providers must recognize the characteristic optic nerve appearance, risk factors, and collate the results of ancillary testing to establish a correct diagnosis and staging of glaucoma. Currently, the American Academy of Ophthalmology recommends routine comprehensive eye examinations for patients with risk factors for glaucoma with a frequency determined on an individual basis, considering age, risk factors, race, and family history.
Glaucoma management is tailored to the specific type and severity. However, there is no treatment at this time that can reverse any of the vision loss that has occurred, it can only help to prevent further damage and vision loss. Visual field testing and mapping of vision loss are helpful in monitoring disease progression.
Open-angle glaucoma is generally managed initially with medications to lower eye pressure. Medication classes include prostaglandin analogs, beta blockers, carbonic anhydrase inhibitors, an alpha-2 agonist, miotic agents, and more recently rho-kinase inhibitors and nitric-oxide donating medications. Laser trabeculoplasty is also used as a primary treatment option in some cases. If medical management cannot be achieved successfully, procedures like laser trabeculoplasty, trabeculectomy, inserting a drainage valve/tube shunt, or laser treatment to the ciliary body to reduce aqueous production can be used to establish better control of IOP. Minimally invasive glaucoma surgery (MIGS) is another evolving option for those who have mild-moderate glaucoma. MIGS has a more favorable overall safety profile compared with conventional trabeculectomy and tube shunts, more rapid recovery time, and have proven effective for IOP reduction to the mid-high teens level. Studies also support that MIGS placement can reduce the number of pressure lowering medications required to maintain target IOP levels.[22]
Normal-tension glaucoma can be treated with medications to lower intraocular pressure and should also have any other possible underlying medical conditions treated. Medications such as prostaglandin analogs, alpha-2 agonists, carbonic anhydrase inhibitors and miotics. Beta-blockers are controversial due to questions of decreased optic nerve head perfusion, especially with the potential exacerbation of the early AM nadir in blood pressure observed. If medical management fails, laser trabeculoplasty or filtration surgery can be utilized if continued progression of vision loss. In the Collaborative normal tension glaucoma study, patients with normal-tension glaucoma have been shown to slow or stabilize their field loss after a 30% reduction in IOP.[23]
Angle-closure is an emergency and must be treated as such. This is because pressures can be high enough to cause glaucomatous optic nerve damage, ischemic nerve damage, or retinal vascular occlusion.[24] Patients can take medication to reduce eye pressure as quickly as possible but usually require a laser procedure called laser peripheral iridotomy. This laser creates a small hole in the iris to relieve the pupillary block, causing the pressure gradient between the posterior and anterior chambers to equalize, resolving iris bombe and opening the anterior chamber drainage angle, then the peripheral iris can be flattened with laser iridoplasty and, less commonly, with laser pupilloplasty. Decreased intraocular pressure is not necessarily a confirmation that the angle has reopened since the ciliary body can undergo ischemic damage during an attack and have decreased production for a few weeks, so it is important to have a follow up gonioscopy to ensure the angle has reopened and to comment on the percentage of the angle with peripheral anterior synechia from the acute or prior subacute attacks.[24] Once the acute crisis has been taken care of, patients are at high risk of having an attack in the contralateral eye and therefore should be considered for gonioscopy and if narrow, prophylactic iridotomy in the other eye.[24]
Secondary glaucoma should be treated for the underlying cause of glaucoma with the possible addition of medications to lower intraocular pressure depending on the underlying cause. [25]
Glaucoma is a chronic and serious disease that can result in permanent vision loss if not taken care of properly. Regular eye appointments and compliance with medication are vital to helping slow down disease progression. Since glaucoma has a hereditary component, it is important to educate family members that they may be at an increased risk to develop glaucoma and may need to have screening done regularly by an eye doctor for early detection.
If the patient has elevated intraocular pressure, the patient must be referred to an ophthalmologist.
Glaucoma is a chronic and serious disease that can result in permanent vision loss if not taken care of properly. To reduce the morbidity of the disorder, the condition is best managed by an interprofessional team that is dedicated to the management of patients with vision problems. The key to treatment is patient education. The pharmacist should emphasize the importance of medication compliance and the need to follow up with the eye surgeon. The ophthalmic nurse should assess the intraocular pressure and convey the result to the ophthalmologist.
Regular eye appointments and compliance with medication are vital to helping slow down disease progression. Since glaucoma has a hereditary component, it is important to educate family members that they may be at an increased risk to develop glaucoma and may need to have screening done regularly by an eye doctor for early detection.
No member of the team should change the dose or frequency without first consulting with the ophthalmologist. Only through open communication between the members can the morbidity of glaucoma be decreased. [26](Level V)
Glaucoma is not a benign disorder and if left untreated can lead to permanent vision loss. The higher the pressure, the greater the risk of damaging the optic nerve. However, with treatment, the prognosis is good for most patients.
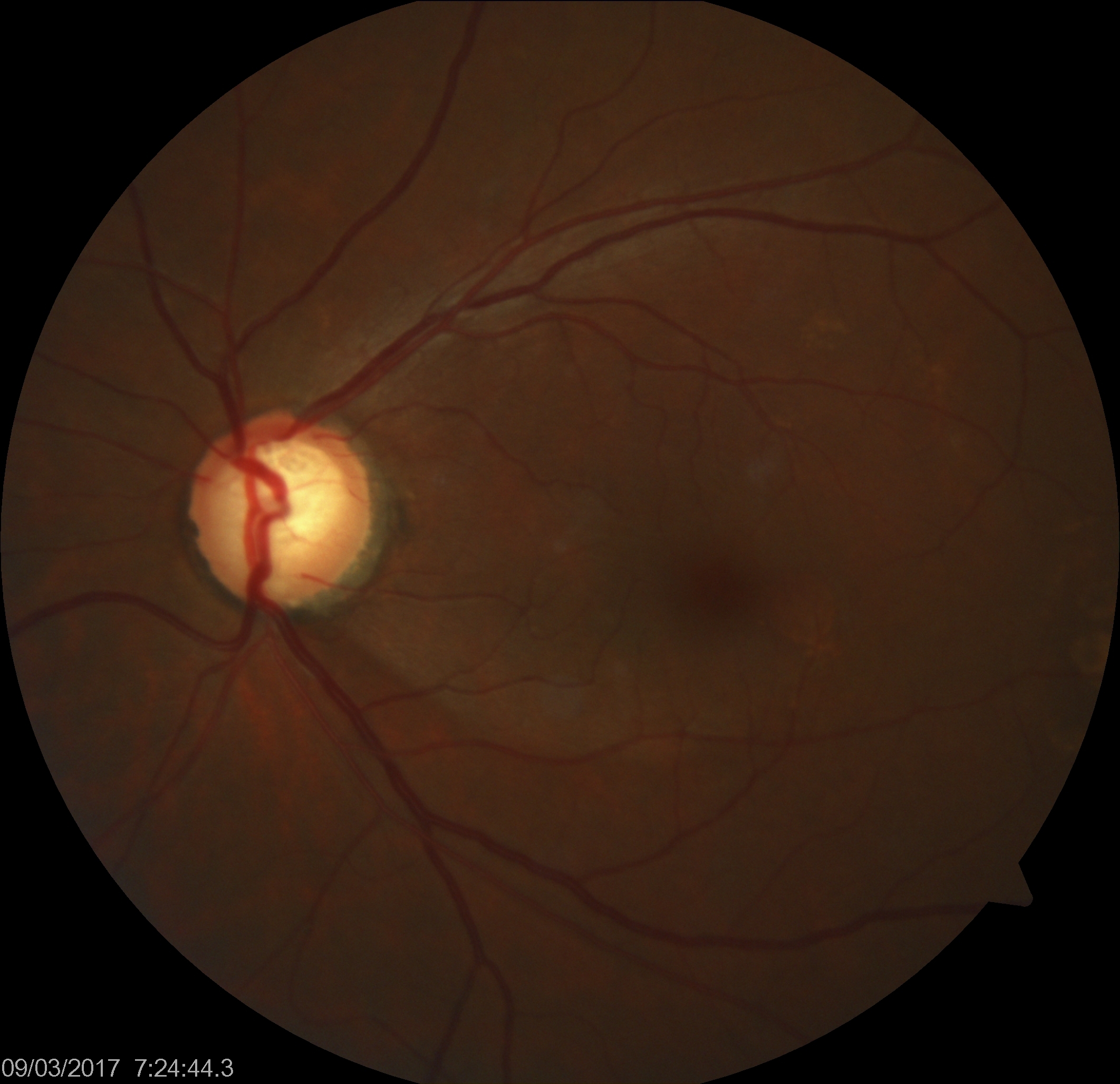
Glaucomatous Optic Nerve Head Showing Inferotemporal Retinal Nerve Fiber Layer Defect. Increased intraocular pressure can result in reduced blood supply to the optic nerve fibers, resulting in subtle ischemic injury.
Contributed by K Tripathy, MD
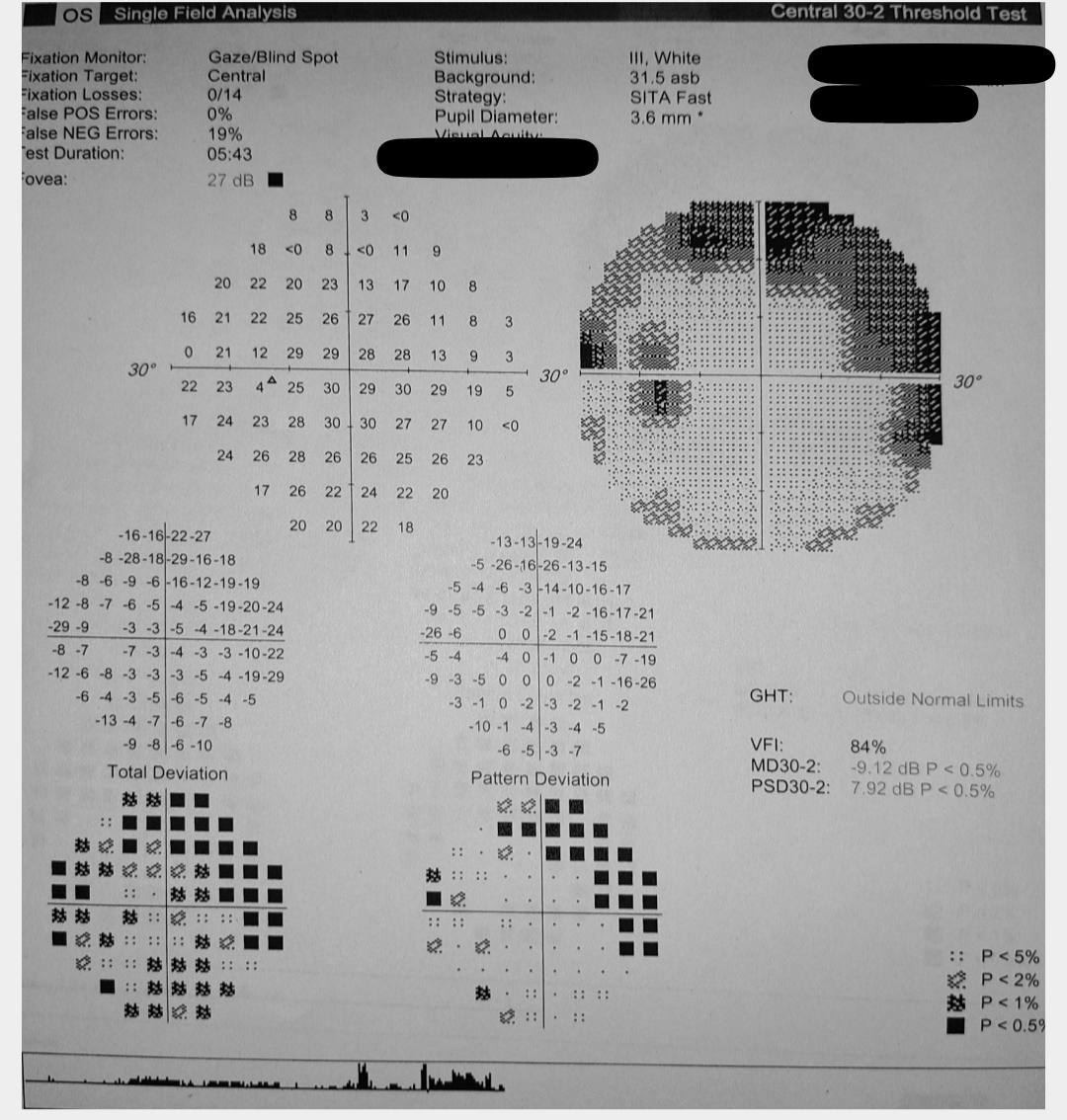
Glaucomatous Visual Field Changes in the Left Eye. This image displays the results of a visual field test indicating characteristic changes associated with glaucoma in the left eye, as observed on perimetry.
Contributed by S Shah, MBBS
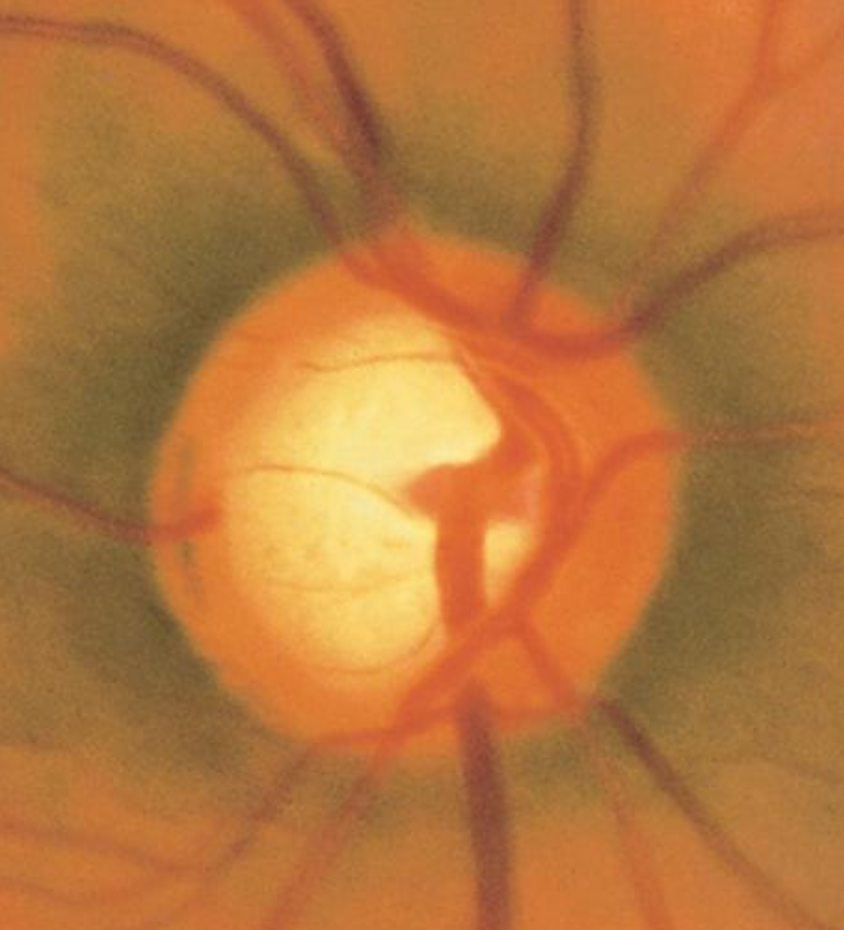
Optic Nerve Cup-to-Disc Ratio of 0.75. A cup-to-disc ratio greater than 0.5 is often associated with glaucoma, and initial loss is typically observed in the inferotemporal and superotemporal poles of the optic disc.
Contributed by AS Huang, MD
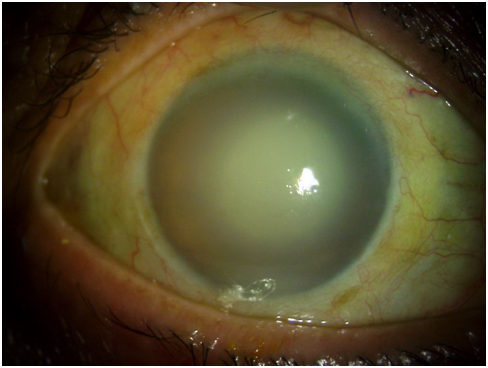
Hypermature Morgagnian Cataract. This image captures the outcome of treatment for an older male patient who initially presented with severe corneal edema, congestion, and elevated intraocular pressure. Following the administration of antiglaucoma medications and topical steroids, a remarkable reduction in corneal edema was observed, exposing a hypermature Morgagnian cataract.
Sridhar U. Cornea Illustrated: A Guide to Clinical Diagnosis. Kolkata, West Bengal, India: New Central Book Agency; 2017.
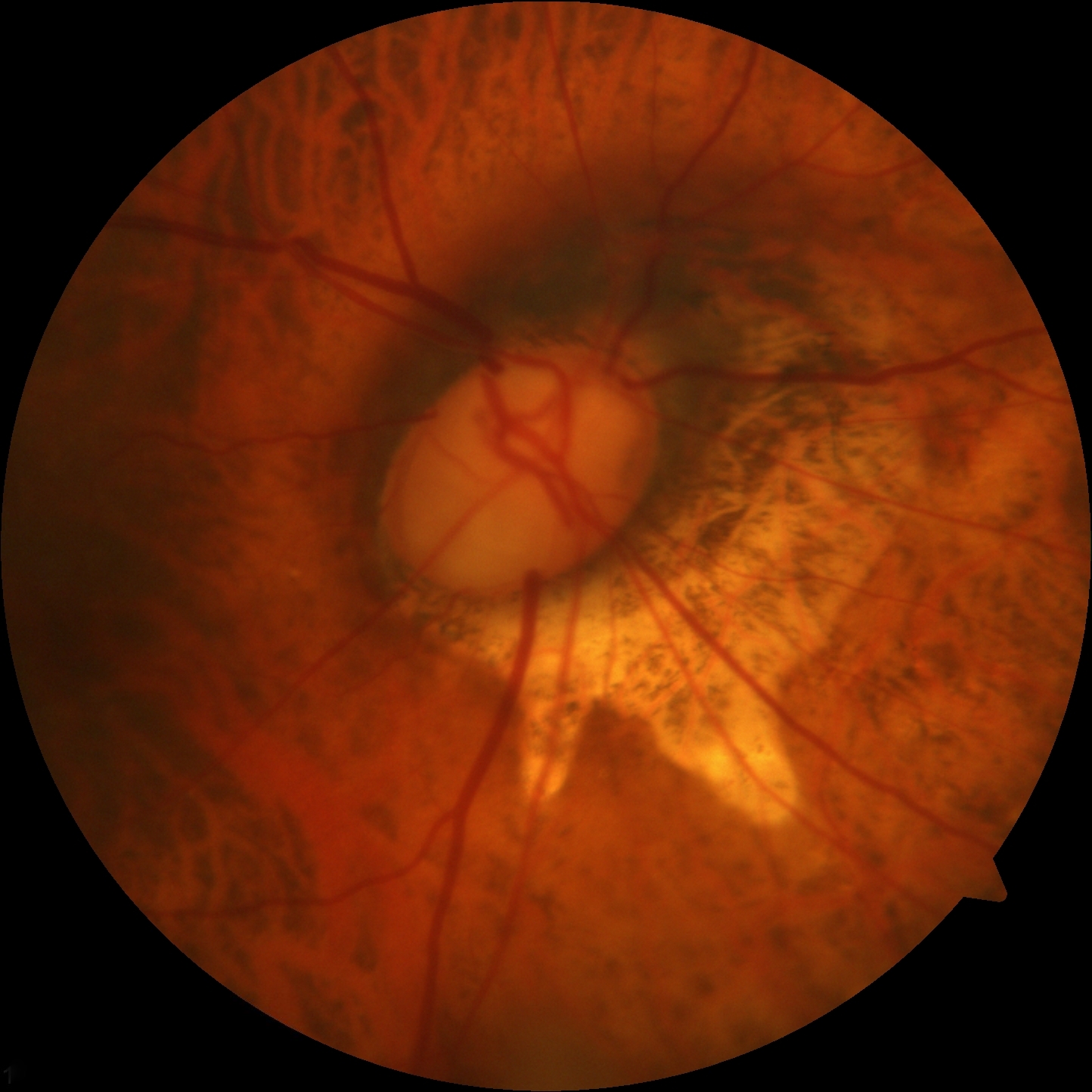
Advanced Glaucomatous Damage to the Optic Nerve. This image illustrates the severe and advanced glaucomatous damage to the optic nerve observed in a patient with high myopia.
Contributed by K Tripathy, MD
Ezinne NE, Shittu O, Ekemiri KK, Kwarteng MA, Tagoh S, Ogbonna G, Mashige KP. Visual Impairment and Blindness among Patients at Nigeria Army Eye Centre, Bonny Cantonment Lagos, Nigeria. Healthcare (Basel, Switzerland). 2022 Nov 18:10(11):. doi: 10.3390/healthcare10112312. Epub 2022 Nov 18 [PubMed PMID: 36421637]
Mahabadi N, Foris LA, Tripathy K. Open Angle Glaucoma. StatPearls. 2024 Jan:(): [PubMed PMID: 28722917]
Wagner IV, Stewart MW, Dorairaj SK. Updates on the Diagnosis and Management of Glaucoma. Mayo Clinic proceedings. Innovations, quality & outcomes. 2022 Dec:6(6):618-635. doi: 10.1016/j.mayocpiqo.2022.09.007. Epub 2022 Nov 16 [PubMed PMID: 36405987]
Cook C, Foster P. Epidemiology of glaucoma: what's new? Canadian journal of ophthalmology. Journal canadien d'ophtalmologie. 2012 Jun:47(3):223-6. doi: 10.1016/j.jcjo.2012.02.003. Epub [PubMed PMID: 22687296]
Gallo Afflitto G, Aiello F, Cesareo M, Nucci C. Primary Open Angle Glaucoma Prevalence in Europe: A Systematic Review and Meta-Analysis. Journal of glaucoma. 2022 Oct 1:31(10):783-788. doi: 10.1097/IJG.0000000000002083. Epub 2022 Aug 9 [PubMed PMID: 35980843]
Singh K, Bhushan P, Mishra D, Kaur K, Gurnani B, Singh A, Pandey S. Assessment of optic disk by disk damage likelihood scale staging using slit-lamp biomicroscopy and optical coherence tomography in diagnosing primary open-angle glaucoma. Indian journal of ophthalmology. 2022 Dec:70(12):4152-4157. doi: 10.4103/ijo.IJO_1113_22. Epub [PubMed PMID: 36453304]
Jonas JB, Aung T, Bourne RR, Bron AM, Ritch R, Panda-Jonas S. Glaucoma. Lancet (London, England). 2017 Nov 11:390(10108):2183-2193. doi: 10.1016/S0140-6736(17)31469-1. Epub 2017 May 31 [PubMed PMID: 28577860]
Parab A, Kavitha S, Odayappan A, Venkatesh R. Clinical and demographic profile of patients less than 40 years of age presenting to glaucoma services at a tertiary care eye hospital in South India. Indian journal of ophthalmology. 2022 Dec:70(12):4186-4192. doi: 10.4103/ijo.IJO_963_22. Epub [PubMed PMID: 36453311]
Khazaeni B, Zeppieri M, Khazaeni L. Acute Angle-Closure Glaucoma. StatPearls. 2024 Jan:(): [PubMed PMID: 28613607]
Foster PJ, Luben R, Khawaja AP. Association, Risk, and Causation-Examining the Role of Systemic Medications in the Onset of Acute Angle-Closure Episodes. JAMA ophthalmology. 2022 Nov 1:140(11):1064-1065. doi: 10.1001/jamaophthalmol.2022.3724. Epub [PubMed PMID: 36136324]
Xu KM, Cho R, Chan TYB. Retrospective Analysis of Switching Bimatoprost 0.01% to Bimatoprost 0.03% in Patients with Various Types of Glaucoma and Ocular Hypertension. Clinical ophthalmology (Auckland, N.Z.). 2022:16():2385-2390. doi: 10.2147/OPTH.S368214. Epub 2022 Jul 29 [PubMed PMID: 35936971]
Gosling D, Meyer JJ. Normal Tension Glaucoma. StatPearls. 2024 Jan:(): [PubMed PMID: 35015402]
Bailey JN, Loomis SJ, Kang JH, Allingham RR, Gharahkhani P, Khor CC, Burdon KP, Aschard H, Chasman DI, Igo RP Jr, Hysi PG, Glastonbury CA, Ashley-Koch A, Brilliant M, Brown AA, Budenz DL, Buil A, Cheng CY, Choi H, Christen WG, Curhan G, De Vivo I, Fingert JH, Foster PJ, Fuchs C, Gaasterland D, Gaasterland T, Hewitt AW, Hu F, Hunter DJ, Khawaja AP, Lee RK, Li Z, Lichter PR, Mackey DA, McGuffin P, Mitchell P, Moroi SE, Perera SA, Pepper KW, Qi Q, Realini T, Richards JE, Ridker PM, Rimm E, Ritch R, Ritchie M, Schuman JS, Scott WK, Singh K, Sit AJ, Song YE, Tamimi RM, Topouzis F, Viswanathan AC, Verma SS, Vollrath D, Wang JJ, Weisschuh N, Wissinger B, Wollstein G, Wong TY, Yaspan BL, Zack DJ, Zhang K, Study EN, ANZRAG Consortium, Weinreb RN, Pericak-Vance MA, Small K, Hammond CJ, Aung T, Liu Y, Vithana EN, MacGregor S, Craig JE, Kraft P, Howell G, Hauser MA, Pasquale LR, Haines JL, Wiggs JL. Genome-wide association analysis identifies TXNRD2, ATXN2 and FOXC1 as susceptibility loci for primary open-angle glaucoma. Nature genetics. 2016 Feb:48(2):189-94. doi: 10.1038/ng.3482. Epub 2016 Jan 11 [PubMed PMID: 26752265]
Wu X, Yang X, Liang Q, Xue X, Huang J, Wang J, Xu Y, Tong R, Liu M, Zhou Q, Shi J. Drugs for the treatment of glaucoma: Targets, structure-activity relationships and clinical research. European journal of medicinal chemistry. 2021 Dec 15:226():113842. doi: 10.1016/j.ejmech.2021.113842. Epub 2021 Sep 11 [PubMed PMID: 34536672]
Buffault J, Labbé A, Hamard P, Brignole-Baudouin F, Baudouin C. The trabecular meshwork: Structure, function and clinical implications. A review of the literature. Journal francais d'ophtalmologie. 2020 Sep:43(7):e217-e230. doi: 10.1016/j.jfo.2020.05.002. Epub 2020 Jun 16 [PubMed PMID: 32561029]
Shen WC, Huang BQ, Yang J. Regulatory mechanisms of retinal ganglion cell death in normal tension glaucoma and potential therapies. Neural regeneration research. 2023 Jan:18(1):87-93. doi: 10.4103/1673-5374.344831. Epub [PubMed PMID: 35799514]
Kaur K, Gurnani B. Primary Congenital Glaucoma. StatPearls. 2024 Jan:(): [PubMed PMID: 34662067]
Yeung HH, Kumar-Singh R, Walton DS. Infantile Aphakic Glaucoma: A Proposed Mechanism. Journal of pediatric ophthalmology and strabismus. 2022 Jul-Aug:59(4):236-242. doi: 10.3928/01913913-20210929-02. Epub 2021 Dec 20 [PubMed PMID: 34928772]
Jafer Chardoub AA, Blair K. Juvenile Glaucoma. StatPearls. 2024 Jan:(): [PubMed PMID: 32965934]
Turalba AV, Chen TC. Clinical and genetic characteristics of primary juvenile-onset open-angle glaucoma (JOAG). Seminars in ophthalmology. 2008 Jan-Feb:23(1):19-25. doi: 10.1080/08820530701745199. Epub [PubMed PMID: 18214788]
Drance S, Anderson DR, Schulzer M, Collaborative Normal-Tension Glaucoma Study Group. Risk factors for progression of visual field abnormalities in normal-tension glaucoma. American journal of ophthalmology. 2001 Jun:131(6):699-708 [PubMed PMID: 11384564]
Terelak-Borys B, Czechowicz-Janicka K. Investigation into the vasospastic mechanisms in the pathogenesis of glaucomatous neuropathy. Klinika oczna. 2011:113(7-9):201-8 [PubMed PMID: 22256559]
Reinehr S, Guntermann A, Theile J, Benning L, Grotegut P, Kuehn S, Serschnitzki B, Dick HB, Marcus K, Joachim SC, May C. Proteomic Analysis of Retinal Tissue in an S100B Autoimmune Glaucoma Model. Biology. 2021 Dec 23:11(1):. doi: 10.3390/biology11010016. Epub 2021 Dec 23 [PubMed PMID: 35053014]
Nowrouzi A, Benitez-Del-Castillo J, Kafi-Abasabadi S, Rodriguez-Calzadilla M, Diaz-Ramos A, Rodriguez-Suarez A, Mota-Chozas I. Peripheral vascular disease - a new vascular disease associated with normal tension glaucoma: a case report. Journal of medical case reports. 2020 Nov 19:14(1):224. doi: 10.1186/s13256-020-02533-3. Epub 2020 Nov 19 [PubMed PMID: 33208187]
Sung MS, Ji YS, Heo H, Park SW. Comparison of the Structure-Function Relationship Between Advanced Primary Open Angle Glaucoma and Normal Tension Glaucoma. Journal of glaucoma. 2022 Jul 1:31(7):574-583. doi: 10.1097/IJG.0000000000002053. Epub 2022 May 16 [PubMed PMID: 35583511]
Dave SD, Meyer JJ. Chronic Closed Angle Glaucoma. StatPearls. 2024 Jan:(): [PubMed PMID: 32644524]
Sener H, Evereklioglu C, Horozoglu F, Sener ABG. Optic nerve head vessel density using OCTA in patients with primary angle closure disease: A systematic review and network meta-analysis. Photodiagnosis and photodynamic therapy. 2023 Mar:41():103209. doi: 10.1016/j.pdpdt.2022.103209. Epub 2022 Dec 6 [PubMed PMID: 36493693]
Samokhvalov NV, Sorokin EL, Marchenko AN, Pashentsev IE. [Anatomical and morphometric features of anterior eye segment structures in hyperopia and the risk of developing primary angle-closure glaucoma]. Vestnik oftalmologii. 2022:138(5):22-28. doi: 10.17116/oftalma202213805122. Epub [PubMed PMID: 36288414]
Cai JC, Chen YL, Cao YH, Babenko A, Chen X. Numerical study of aqueous humor flow and iris deformation with pupillary block and the efficacy of laser peripheral iridotomy. Clinical biomechanics (Bristol, Avon). 2022 Feb:92():105579. doi: 10.1016/j.clinbiomech.2022.105579. Epub 2022 Jan 19 [PubMed PMID: 35085976]
Douglas GR, Drance SM, Schulzer M. The visual field and nerve head in angle-closure glaucoma. A comparison of the effects of acute and chronic angle closure. Archives of ophthalmology (Chicago, Ill. : 1960). 1975 Jun:93(6):409-11 [PubMed PMID: 1131080]
Izquierdo NJ, Traboulsi EI, Enger C, Maumenee IH. Glaucoma in the Marfan syndrome. Transactions of the American Ophthalmological Society. 1992:90():111-7; discussion 118-22 [PubMed PMID: 1494814]
Kondo K, Isono H. A case of angle-closure glaucoma caused by spontaneous lens dislocation. Clinical case reports. 2022 Dec:10(12):e6670. doi: 10.1002/ccr3.6670. Epub 2022 Dec 5 [PubMed PMID: 36483875]
Shah SS, Meyer JJ. Lens-Induced Glaucoma. StatPearls. 2024 Jan:(): [PubMed PMID: 34662038]
Kale Y, Isik DU, Celik U, Hekimoglu E, Celik IH, Bas AY, Demirel N. Neonatal Marfan syndrome with angle-closure glaucoma, tricuspid and mitral insufficiency. Genetic counseling (Geneva, Switzerland). 2015:26(1):95-8 [PubMed PMID: 26043516]
Alshomar K, Alsirhy E, Mirza A, Osman M, Alobaidan A, Osman EA. Prevalence of Plateau Iris Syndrome among Patients Presenting with Primary Angle Closure and Primary Angle-Closure Glaucoma in a Tertiary Eye Care Hospital. Middle East African journal of ophthalmology. 2021 Oct-Dec:28(4):221-225. doi: 10.4103/meajo.meajo_232_21. Epub 2022 Apr 30 [PubMed PMID: 35719280]
Kiuchi Y, Kanamoto T, Nakamura T. Double hump sign in indentation gonioscopy is correlated with presence of plateau iris configuration regardless of patent iridotomy. Journal of glaucoma. 2009 Feb:18(2):161-4. doi: 10.1097/IJG.0b013e31817d23b5. Epub [PubMed PMID: 19225356]
Laganowski HC, Kerr Muir MG, Hitchings RA. Glaucoma and the iridocorneal endothelial syndrome. Archives of ophthalmology (Chicago, Ill. : 1960). 1992 Mar:110(3):346-50 [PubMed PMID: 1543451]
D'cruz RP, Rao A. 'Progressive peripheral anterior synechiae in iridocorneoendothelial syndrome- a crawling disaster'. European journal of ophthalmology. 2023 May:33(3):NP40-NP44. doi: 10.1177/11206721211070095. Epub 2021 Dec 29 [PubMed PMID: 34964381]
Sivak-Callcott JA, O'Day DM, Gass JD, Tsai JC. Evidence-based recommendations for the diagnosis and treatment of neovascular glaucoma. Ophthalmology. 2001 Oct:108(10):1767-76; quiz1777, 1800 [PubMed PMID: 11581047]
Mishra C, Meyer JJ. Neovascular Glaucoma. StatPearls. 2024 Jan:(): [PubMed PMID: 35015418]
Perez RN, Phelps CD, Burton TC. Angel-closure glaucoma following scleral buckling operations. Transactions. Section on Ophthalmology. American Academy of Ophthalmology and Otolaryngology. 1976 Mar-Apr:81(2):247-52 [PubMed PMID: 936397]
Aminlari A, East M, Wei W, Quillen D. Topiramate induced acute angle closure glaucoma. The open ophthalmology journal. 2008 Mar 28:2():46-7. doi: 10.2174/1874364100802010046. Epub 2008 Mar 28 [PubMed PMID: 19478906]
Shivkumar C, Gadiwan M, Rout M, Ghosh A, Haroon S, Ramakrishnan R. Visual outcomes and complications of manual small-incision cataract surgery in patients with pseudoexfoliation. Indian journal of ophthalmology. 2022 Nov:70(11):3912-3917. doi: 10.4103/ijo.IJO_1581_22. Epub [PubMed PMID: 36308126]
Collao V, Morris J, Chauhan MZ, Abdelrahman L, Martínez-de-la-Casa JM, Vidal-Villegas B, Burgos-Blasco B, Bhattacharya SK. Analyses of pseudoexfoliation aqueous humor lipidome. Molecular omics. 2022 Jun 13:18(5):387-396. doi: 10.1039/d1mo00495f. Epub 2022 Jun 13 [PubMed PMID: 35485348]
Tuteja S, Zeppieri M, Chawla H. Pseudoexfoliation Syndrome and Glaucoma. StatPearls. 2024 Jan:(): [PubMed PMID: 34662036]
Gurnani B, Kaur K. Pigment Dispersion Syndrome. StatPearls. 2024 Jan:(): [PubMed PMID: 35593834]
Plateroti P, Plateroti AM, Abdolrahimzadeh S, Scuderi G. Pseudoexfoliation Syndrome and Pseudoexfoliation Glaucoma: A Review of the Literature with Updates on Surgical Management. Journal of ophthalmology. 2015:2015():370371. doi: 10.1155/2015/370371. Epub 2015 Oct 29 [PubMed PMID: 26605078]
Zeppieri M. Pigment dispersion syndrome: A brief overview. Journal of clinical and translational research. 2022 Oct 31:8(5):344-350 [PubMed PMID: 36518550]
Zeppieri M, Tripathy K. Pigment Dispersion Glaucoma. StatPearls. 2024 Jan:(): [PubMed PMID: 35593820]
Feroze KB, Zeppieri M, Khazaeni L. Steroid-Induced Glaucoma. StatPearls. 2024 Jan:(): [PubMed PMID: 28613653]
Roll P, Benedikt O. [Electronmicroscopic studies of the trabecular meshwork in corticosteroid glaucoma]. Klinische Monatsblatter fur Augenheilkunde. 1979 Mar:174(3):421-8 [PubMed PMID: 480814]
Khurana M, Alam MS, Balekudaru S, Vijaya L, Madhuri MB, Halbe SV, Noronha VO, George RJ, Mukherjee B. Intraocular Pressure in the Eyes of Patients With Carotid-Cavernous Fistulas: Profile, Intereye Asymmetry, and Treatment Outcomes. Journal of glaucoma. 2019 Dec:28(12):1074-1078. doi: 10.1097/IJG.0000000000001392. Epub [PubMed PMID: 31658226]
Calafiore S, Perdicchi A, Scuderi G, Contestabile MT, Abdolrahimzadeh S, Recupero SM. Glaucoma Management in Carotid Cavernous Fistula. Case reports in ophthalmology. 2016 May-Aug:7(2):296-302. doi: 10.1159/000446151. Epub 2016 Jun 2 [PubMed PMID: 27462258]
Greslechner R, Helbig H, Spiegel D. [Secondary open-angle glaucoma: uveitic secondary glaucoma, steroid-induced glaucoma, posttraumatic and postoperative glaucoma, tumor-related glaucoma and glaucoma due to elevated episcleral venous pressure]. Der Ophthalmologe : Zeitschrift der Deutschen Ophthalmologischen Gesellschaft. 2022 May:119(5):533-546. doi: 10.1007/s00347-022-01630-6. Epub 2022 Apr 26 [PubMed PMID: 35471612]
Sen S, Tripathy K. Uveitis Glaucoma Hyphema Syndrome. StatPearls. 2024 Jan:(): [PubMed PMID: 35593837]
Okonkwo ON, Tripathy K. Posner-Schlossman Syndrome. StatPearls. 2024 Jan:(): [PubMed PMID: 35015437]
Choong YF, Irfan S, Menage MJ. Acute angle closure glaucoma: an evaluation of a protocol for acute treatment. Eye (London, England). 1999 Oct:13 ( Pt 5)():613-6 [PubMed PMID: 10696311]
POSNER A, SCHLOSSMAN A. Further observations on the syndrome of glaucomatocyclitic crises. Transactions - American Academy of Ophthalmology and Otolaryngology. American Academy of Ophthalmology and Otolaryngology. 1953 Jul-Aug:57(4):531-6 [PubMed PMID: 13090248]
Allison K, Patel D, Alabi O. Epidemiology of Glaucoma: The Past, Present, and Predictions for the Future. Cureus. 2020 Nov 24:12(11):e11686. doi: 10.7759/cureus.11686. Epub 2020 Nov 24 [PubMed PMID: 33391921]
Imrie C, Tatham AJ. Glaucoma: the patient's perspective. The British journal of general practice : the journal of the Royal College of General Practitioners. 2016 May:66(646):e371-3. doi: 10.3399/bjgp16X685165. Epub [PubMed PMID: 27127293]
Bourne RR, Stevens GA, White RA, Smith JL, Flaxman SR, Price H, Jonas JB, Keeffe J, Leasher J, Naidoo K, Pesudovs K, Resnikoff S, Taylor HR, Vision Loss Expert Group. Causes of vision loss worldwide, 1990-2010: a systematic analysis. The Lancet. Global health. 2013 Dec:1(6):e339-49. doi: 10.1016/S2214-109X(13)70113-X. Epub 2013 Nov 11 [PubMed PMID: 25104599]
Leung DYL, Tham CC. Normal-tension glaucoma: Current concepts and approaches-A review. Clinical & experimental ophthalmology. 2022 Mar:50(2):247-259. doi: 10.1111/ceo.14043. Epub 2022 Feb 7 [PubMed PMID: 35040248]
Heijl A, Bengtsson B, Hyman L, Leske MC, Early Manifest Glaucoma Trial Group. Natural history of open-angle glaucoma. Ophthalmology. 2009 Dec:116(12):2271-6. doi: 10.1016/j.ophtha.2009.06.042. Epub 2009 Oct 24 [PubMed PMID: 19854514]
Reina-Torres E, Baptiste TMG, Overby DR. Segmental outflow dynamics in the trabecular meshwork of living mice. Experimental eye research. 2022 Dec:225():109285. doi: 10.1016/j.exer.2022.109285. Epub 2022 Oct 21 [PubMed PMID: 36273576]
Gupta V, Singh A, Pandya I, Sofi R, Sen S, Somarajan BI, Gupta S, Nag TC. Differences in outflow channels between two eyes of unilateral primary congenital glaucoma. Acta ophthalmologica. 2021 Mar:99(2):187-194. doi: 10.1111/aos.14540. Epub 2020 Jul 23 [PubMed PMID: 32701215]
Tan S, Yu M, Baig N, Chan PP, Tang FY, Cheung CY, Tham CCY. Association of Ultra-Short-Term Intraocular Pressure Fluctuation With Disease Progression in Primary Angle Closure Glaucoma: The CUPAL Study. Journal of glaucoma. 2022 Nov 1:31(11):874-880. doi: 10.1097/IJG.0000000000002103. Epub 2022 Aug 16 [PubMed PMID: 35980863]
Omodaka K, Kikawa T, Kabakura S, Himori N, Tsuda S, Ninomiya T, Takahashi N, Pak K, Takeda N, Akiba M, Nakazawa T. Clinical characteristics of glaucoma patients with various risk factors. BMC ophthalmology. 2022 Sep 19:22(1):373. doi: 10.1186/s12886-022-02587-5. Epub 2022 Sep 19 [PubMed PMID: 36123604]
Wolvaardt E, Stevens S. Measuring intraocular pressure. Community eye health. 2019:32(107):56-57 [PubMed PMID: 32123477]
Arora T, Bali SJ, Arora V, Wadhwani M, Panda A, Dada T. Diurnal versus office-hour intraocular pressure fluctuation in primary adult onset glaucoma. Journal of optometry. 2015 Oct-Dec:8(4):239-43. doi: 10.1016/j.optom.2014.05.005. Epub 2014 Jun 16 [PubMed PMID: 26386536]
Levene RZ. Low tension glaucoma: a critical review and new material. Survey of ophthalmology. 1980 May-Jun:24(6):621-64 [PubMed PMID: 7414505]
Drance SM, Sweeney VP, Morgan RW, Feldman F. Factors involved in the production of low tension glaucoma. Canadian journal of ophthalmology. Journal canadien d'ophtalmologie. 1974 Oct:9(4):399-403 [PubMed PMID: 4423185]
Soh Z, Yu M, Betzler BK, Majithia S, Thakur S, Tham YC, Wong TY, Aung T, Friedman DS, Cheng CY. The Global Extent of Undetected Glaucoma in Adults: A Systematic Review and Meta-analysis. Ophthalmology. 2021 Oct:128(10):1393-1404. doi: 10.1016/j.ophtha.2021.04.009. Epub 2021 Apr 16 [PubMed PMID: 33865875]
Jonas JB, Fernández MC, Stürmer J. Pattern of glaucomatous neuroretinal rim loss. Ophthalmology. 1993 Jan:100(1):63-8 [PubMed PMID: 8433829]
Chuangsuwanich T, Tun TA, Braeu FA, Wang X, Chin ZY, Panda SK, Buist M, Strouthidis N, Perera S, Nongpiur M, Aung T, Girard MJA. Differing Associations between Optic Nerve Head Strains and Visual Field Loss in Patients with Normal- and High-Tension Glaucoma. Ophthalmology. 2023 Jan:130(1):99-110. doi: 10.1016/j.ophtha.2022.08.007. Epub 2022 Aug 11 [PubMed PMID: 35964710]
Moghimi S, Ramezani F, He M, Coleman AL, Lin SC. Comparison of Anterior Segment-Optical Coherence Tomography Parameters in Phacomorphic Angle Closure and Acute Angle Closure Eyes. Investigative ophthalmology & visual science. 2015 Dec:56(13):7611-7. doi: 10.1167/iovs.15-17336. Epub [PubMed PMID: 26624492]
Thomas R, George R, Parikh R, Muliyil J, Jacob A. Five year risk of progression of primary angle closure suspects to primary angle closure: a population based study. The British journal of ophthalmology. 2003 Apr:87(4):450-4 [PubMed PMID: 12642309]
Bader J, Zeppieri M, Havens SJ. Tonometry. StatPearls. 2024 Jan:(): [PubMed PMID: 29630277]
Brusini P, Salvetat ML, Zeppieri M. How to Measure Intraocular Pressure: An Updated Review of Various Tonometers. Journal of clinical medicine. 2021 Aug 27:10(17):. doi: 10.3390/jcm10173860. Epub 2021 Aug 27 [PubMed PMID: 34501306]
Brusini P, Salvetat ML, Zeppieri M. It Is All about Pressure. Journal of clinical medicine. 2022 Jun 23:11(13):. doi: 10.3390/jcm11133640. Epub 2022 Jun 23 [PubMed PMID: 35806926]
Zeppieri M, Gurnani B. Applanation Tonometry. StatPearls. 2024 Jan:(): [PubMed PMID: 35881737]
Salvetat ML, Zeppieri M, Tosoni C, Brusini P. Repeatability and accuracy of applanation resonance tonometry in healthy subjects and patients with glaucoma. Acta ophthalmologica. 2014 Feb:92(1):e66-73. doi: 10.1111/aos.12209. Epub 2013 Jul 10 [PubMed PMID: 23837834]
Salvetat ML, Zeppieri M, Tosoni C, Brusini P. Comparisons between Pascal dynamic contour tonometry, the TonoPen, and Goldmann applanation tonometry in patients with glaucoma. Acta ophthalmologica Scandinavica. 2007 May:85(3):272-9 [PubMed PMID: 17488456]
Salvetat ML, Zeppieri M, Tosoni C, Felletti M, Grasso L, Brusini P. Corneal Deformation Parameters Provided by the Corvis-ST Pachy-Tonometer in Healthy Subjects and Glaucoma Patients. Journal of glaucoma. 2015 Oct-Nov:24(8):568-74. doi: 10.1097/IJG.0000000000000133. Epub [PubMed PMID: 25318572]
Zeppieri M, Brusini P, Miglior S. Corneal thickness and functional damage in patients with ocular hypertension. European journal of ophthalmology. 2005 Mar-Apr:15(2):196-201 [PubMed PMID: 15812759]
Salvetat ML, Zeppieri M, Tosoni C, Parisi L, Brusini P. Non-conventional perimetric methods in the detection of early glaucomatous functional damage. Eye (London, England). 2010 May:24(5):835-42. doi: 10.1038/eye.2009.216. Epub 2009 Aug 21 [PubMed PMID: 19696803]
Mahmoudinezhad G, Moghimi S, Proudfoot JA, Brye N, Nishida T, Yarmohammadi A, Kamalipour A, Zangwill LM, Weinreb RN. Effect of Testing Frequency on the Time to Detect Glaucoma Progression With Optical Coherence Tomography (OCT) and OCT Angiography. American journal of ophthalmology. 2023 Jan:245():184-192. doi: 10.1016/j.ajo.2022.08.030. Epub 2022 Sep 10 [PubMed PMID: 36096181]
Kelly SR, Khawaja AP, Bryan SR, Azuara-Blanco A, Sparrow JM, Crabb DP. Progression from ocular hypertension to visual field loss in the English hospital eye service. The British journal of ophthalmology. 2020 Oct:104(10):1406-1411. doi: 10.1136/bjophthalmol-2019-315052. Epub 2020 Mar 25 [PubMed PMID: 32217541]
Tan C, Hou Y, Qiao YS, Chen JY, Sun XH. [The study of the correlation between age and the pathogenic factors of primary glaucoma: a review]. [Zhonghua yan ke za zhi] Chinese journal of ophthalmology. 2022 Dec 11:58(12):1106-1110. doi: 10.3760/cma.j.cn112142-20220616-00297. Epub [PubMed PMID: 36480899]
Salvetat ML, Zeppieri M, Tosoni C, Brusini P, Medscape. Baseline factors predicting the risk of conversion from ocular hypertension to primary open-angle glaucoma during a 10-year follow-up. Eye (London, England). 2016 Jun:30(6):784-95. doi: 10.1038/eye.2016.86. Epub 2016 May 13 [PubMed PMID: 27174381]
Buffault J, Brignole-Baudouin F, Reboussin É, Kessal K, Labbé A, Mélik Parsadaniantz S, Baudouin C. The Dual Effect of Rho-Kinase Inhibition on Trabecular Meshwork Cells Cytoskeleton and Extracellular Matrix in an In Vitro Model of Glaucoma. Journal of clinical medicine. 2022 Feb 15:11(4):. doi: 10.3390/jcm11041001. Epub 2022 Feb 15 [PubMed PMID: 35207274]
Walters TR, Kothe AC, Boyer JL, Usner DW, Lopez K, Duquesroix B, Fechtner RD, Navratil T. A Randomized, Controlled Comparison of NCX 470 (0.021%, 0.042%, and 0.065%) and Latanoprost 0.005% in Patients With Open-angle Glaucoma or Ocular Hypertension: The Dolomites Study. Journal of glaucoma. 2022 Jun 1:31(6):382-391. doi: 10.1097/IJG.0000000000002030. Epub 2022 Apr 6 [PubMed PMID: 35394456]
Zhou R, Sun Y, Chen H, Sha S, He M, Wang W. Laser Trabeculoplasty for Open-Angle Glaucoma: A Systematic Review and Network Meta-Analysis. American journal of ophthalmology. 2021 Sep:229():301-313. doi: 10.1016/j.ajo.2020.07.046. Epub 2020 Sep 2 [PubMed PMID: 32888900]
Muralidharan S, Kumar S, Ichhpujani P, Dhillon HK. Quality of life in glaucoma patients: Comparison of medical therapy, trabeculectomy, and glaucoma drainage device surgery. Indian journal of ophthalmology. 2022 Dec:70(12):4206-4211. doi: 10.4103/ijo.IJO_667_22. Epub [PubMed PMID: 36453315]
Brusini P, Papa V, Zeppieri M. Canaloplasty in Pseudoexfoliation Glaucoma. Can It Still Be Considered a Good Choice? Journal of clinical medicine. 2022 Apr 30:11(9):. doi: 10.3390/jcm11092532. Epub 2022 Apr 30 [PubMed PMID: 35566656]
Rojananuangnit K, Jiaranaisilawong P, Rattanaphaithun O, Sathim W. Surgical Outcomes of Glaucoma Drainage Device Implantation in Refractory Glaucoma Patients in Thailand. Clinical ophthalmology (Auckland, N.Z.). 2022:16():4163-4178. doi: 10.2147/OPTH.S393730. Epub 2022 Dec 14 [PubMed PMID: 36540897]
Gurnani B, Tripathy K. Minimally Invasive Glaucoma Surgery. StatPearls. 2024 Jan:(): [PubMed PMID: 35881761]
Craven ER, Katz LJ, Wells JM, Giamporcaro JE, iStent Study Group. Cataract surgery with trabecular micro-bypass stent implantation in patients with mild-to-moderate open-angle glaucoma and cataract: two-year follow-up. Journal of cataract and refractive surgery. 2012 Aug:38(8):1339-45. doi: 10.1016/j.jcrs.2012.03.025. Epub [PubMed PMID: 22814041]
Anderson DR, Normal Tension Glaucoma Study. Collaborative normal tension glaucoma study. Current opinion in ophthalmology. 2003 Apr:14(2):86-90 [PubMed PMID: 12698048]
Wright C, Tawfik MA, Waisbourd M, Katz LJ. Primary angle-closure glaucoma: an update. Acta ophthalmologica. 2016 May:94(3):217-25. doi: 10.1111/aos.12784. Epub 2015 Jun 27 [PubMed PMID: 26119516]
Bai HQ, Yao L, Wang DB, Jin R, Wang YX. Causes and treatments of traumatic secondary glaucoma. European journal of ophthalmology. 2009 Mar-Apr:19(2):201-6 [PubMed PMID: 19253235]
Musa MJ, Zeppieri M. Foster Kennedy Syndrome. StatPearls. 2024 Jan:(): [PubMed PMID: 35881754]
Leibowitz HM. The red eye. The New England journal of medicine. 2000 Aug 3:343(5):345-51 [PubMed PMID: 10922425]
Greenfield DS. Glaucomatous versus nonglaucomatous optic disc cupping: clinical differentiation. Seminars in ophthalmology. 1999 Jun:14(2):95-108 [PubMed PMID: 10758217]
Pasol J. Neuro-ophthalmic disease and optical coherence tomography: glaucoma look-alikes. Current opinion in ophthalmology. 2011 Mar:22(2):124-32. doi: 10.1097/ICU.0b013e328343c1a3. Epub [PubMed PMID: 21307679]
Harwerth RS, Quigley HA. Visual field defects and retinal ganglion cell losses in patients with glaucoma. Archives of ophthalmology (Chicago, Ill. : 1960). 2006 Jun:124(6):853-9 [PubMed PMID: 16769839]
Pelčić G, Ljubičić R, Barać J, Biuk D, Rogoić V. Glaucoma, depression and quality of life: multiple comorbidities, multiple assessments and multidisciplinary plan treatment. Psychiatria Danubina. 2017 Sep:29(3):351-359. doi: 10.24869/psyd.2017.351. Epub [PubMed PMID: 28949316]