Learning Outcome
- Describes the types of anemia
- List the causes of anemia
- Summarize the treatment of anemia

The word anemia derives from an ancient Greek word anaimia, meaning “lack of blood.”
Anemia, like a fever, is not a diagnosis but a presentation of an underlying disease. Multiple diseases can present as anemia due to various mechanisms.
Anemia affects a significant number of people worldwide (more so in the developing world), resulting in a considerable increase in the cost of medical care.
Anemia can be defined as a reduction in hemoglobin (less than 13.5 g/dL in men; less than 12.0 g/dL in women) or hematocrit (less than 41.0% in men; less than 36.0% in women) or red blood cell (RBC) count. The terms hemoglobin and hematocrit are more commonly used than RBC count in day-to-day clinical practice. There are different lower limits of normal range based on ethnicity, gender, and age.
Anemia causes decreased oxygen-carrying capacity of the blood leading to tissue hypoxia.
Grading of Anemia, according to the National Cancer Institute, is as follows:
Anemia classified into acute anemia and chronic anemia. Acute anemia is predominantly due to acute blood loss or acute hemolysis. Chronic anemia is more common and is secondary to multiple causes.
Etiology of chronic anemia based on mean corpuscular volume (MCV is the average size of RBC).
Microcytic Anemia (MCV less than 80 femtoliters [fL])
Macrocytic Anemia (MCV greater than 100 fL)
Normocytic Anemia (MCV 80 to 100 fL)
Some conditions can present in more than 1 classification. For example, early iron deficiency can be normocytic. Anemia of chronic disease is mostly normocytic but can be microcytic too. Hemolytic anemia[2] can cause either macrocytic or normocytic anemia.
Iron deficiency anemia is the most common type of anemia, affecting approximately 8% to 9% of the world’s population.
Anemia is more prevalent in:
Symptoms and signs of chronic anemia are mostly due to decreased tissue oxygenation from the reduction of the oxygen-carrying capacity of the blood. Symptoms are worse when anemia is severe, with a rapid decrease in hemoglobin/HCT and with increased oxygen demands states like exercise.
Common presenting symptoms include:
A detailed history should include medical history, home medications, alcohol use, and family history. Ethnicity and country of origin are also helpful.
Important examination findings include:
Initial Work-Up
Differentiation of Microcytic Anemias Based on Iron Studies
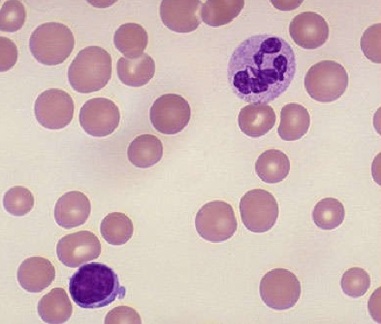
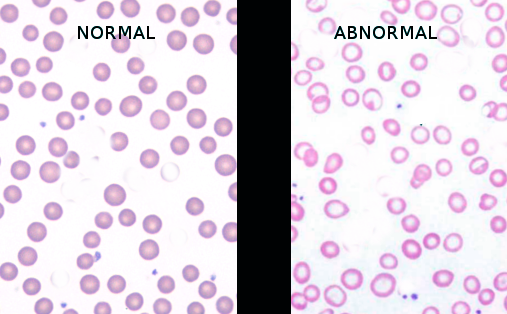
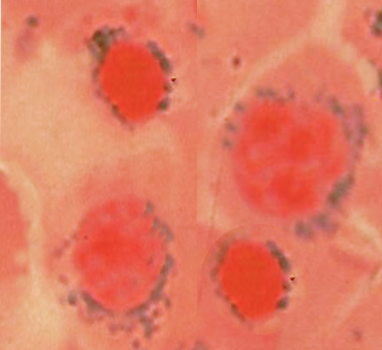
Peripheral smear, hemoglobin electrophoresis, and bone marrow examination if needed. Further testing would include esophagogastroduodenoscopy (EGD) and colonoscopy if gastrointestinal (GI) bleeding is suspected and imaging studies if malignancy suspected.
Chronic anemia is managed predominantly in outpatient settings. They need hospitalization if:
If hemoglobin is less than 7 g/dL or if a patent is symptomatic, transfusion of packed red blood cells (PRBC) is indicated.
Transfusions should be done with caution in patients with volume overload status like end-stage renal disease (on hemodialysis) and congestive heart failure (CHF).
Other treatments include treating underlying conditions as below.
Chronic anemia is a very common condition seen in day-to-day clinical practice and managed in outpatient settings. Anemia management can range from simple to complex based on the underlying condition causing it. Most of the time patient's primary care physician needs help with a specialist based on underlying condition either a gastroenterologist or a hematologist or a nephrologist or a gynecologist. It is very important to have good interprofessional communication and care coordination for the management of anemia appropriately and promptly. This would help both in correcting anemia and treating underlying conditions.
Anemia is a condition with decreased oxygen-carrying capacity of the blood. Anemia is very common and caused by different conditions ranging from simple nutritional deficiencies (iron, vitamin B12, and folic acid) to blood loss to other complicated causes.
Anemia is a common medical condition and easily diagnosed with a simple blood work CBC. Treatment can be simple like nutritional supplements (iron, vitamin B12, and folic acid) to blood transfusion to treating complex underlying conditions.
It is very important to follow up with the doctor and sometimes with a specialist to treat anemia because untreated anemia can be life-threatening and may even cause death.
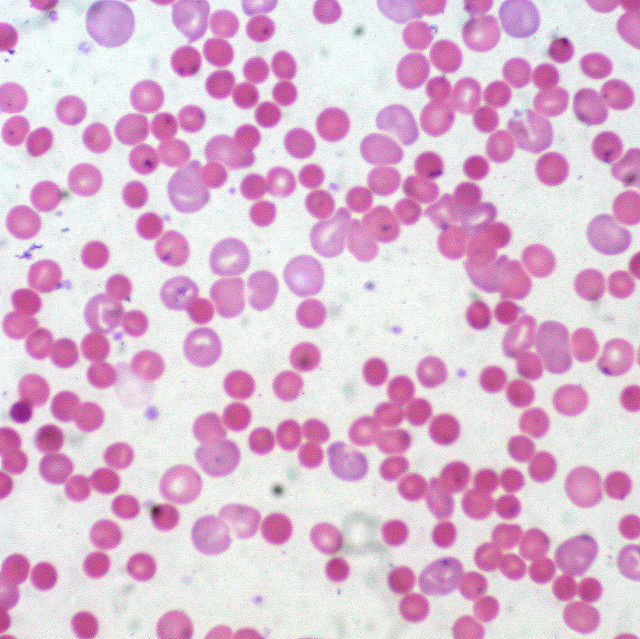
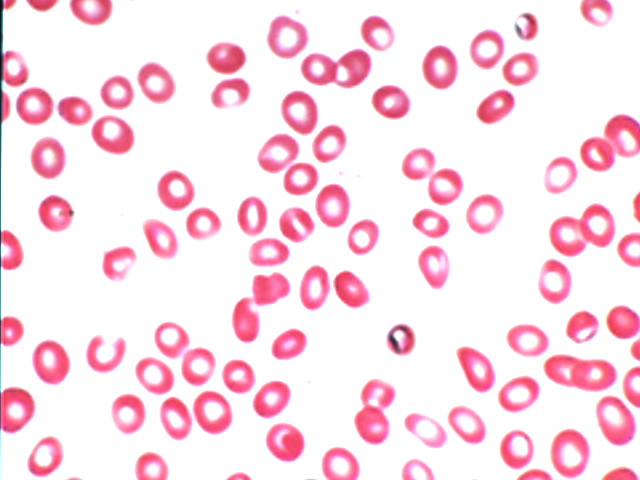
Hypochromic Microcytic Anemia
Image courtesy S Bhimji MD
Tas F, Eralp Y, Basaran M, Sakar B, Alici S, Argon A, Bulutlar G, Camlica H, Aydiner A, Topuz E. Anemia in oncology practice: relation to diseases and their therapies. American journal of clinical oncology. 2002 Aug:25(4):371-9 [PubMed PMID: 12151968]
Sachdev V, Rosing DR, Thein SL. Cardiovascular complications of sickle cell disease. Trends in cardiovascular medicine. 2021 Apr:31(3):187-193. doi: 10.1016/j.tcm.2020.02.002. Epub 2020 Feb 11 [PubMed PMID: 32139143]
Baradwan S, Alyousef A, Turkistani A. Associations between iron deficiency anemia and clinical features among pregnant women: a prospective cohort study. Journal of blood medicine. 2018:9():163-169. doi: 10.2147/JBM.S175267. Epub 2018 Oct 3 [PubMed PMID: 30323700]
Lanier JB, Park JJ, Callahan RC. Anemia in Older Adults. American family physician. 2018 Oct 1:98(7):437-442 [PubMed PMID: 30252420]
Kunireddy N, Jacob R, Khan SA, Yadagiri B, Sai Baba KSS, Rajendra Vara Prasad I, Mohan IK. Hepcidin and Ferritin: Important Mediators in Inflammation Associated Anemia in Systemic Lupus Erythematosus Patients. Indian journal of clinical biochemistry : IJCB. 2018 Oct:33(4):406-413. doi: 10.1007/s12291-017-0702-1. Epub 2017 Oct 28 [PubMed PMID: 30319186]
Anand S,Thomas B,Remuzzi G,Riella M,Nahas ME,Naicker S,Dirks J, Kidney Disease null. 2017 Nov 17 [PubMed PMID: 30212067]
Hong CT, Hsieh YC, Liu HY, Chiou HY, Chien LN. Association Between Anemia and Dementia: A Nationwide, Populationbased Cohort Study in Taiwan. Current Alzheimer research. 2020:17(2):196-204. doi: 10.2174/1567205017666200317101516. Epub [PubMed PMID: 32183675]
Agbozo F, Abubakari A, Der J, Jahn A. Maternal Dietary Intakes, Red Blood Cell Indices and Risk for Anemia in the First, Second and Third Trimesters of Pregnancy and at Predelivery. Nutrients. 2020 Mar 15:12(3):. doi: 10.3390/nu12030777. Epub 2020 Mar 15 [PubMed PMID: 32183478]
Ray JG, Davidson A, Berger H, Dayan N, Park AL. Haemoglobin levels in early pregnancy and severe maternal morbidity: population-based cohort study. BJOG : an international journal of obstetrics and gynaecology. 2020 Aug:127(9):1154-1164. doi: 10.1111/1471-0528.16216. Epub 2020 Apr 6 [PubMed PMID: 32175668]