Introduction
The vasculature of the body is an essential network for maintaining healthy skin tissue. Skin changes, including blanching, ecchymosis, and edema, are a result of changes in vascularity. The face is a highly vascularized region of the body with constant exposure to the harsh environment. One of the most dominant features on the face is the lips, which serve many functions for daily living. The lips are composed of skin, a network of vessels, and muscles. The functionality of the lips relies on the simultaneous action of many muscles to carry out each movement. The movements of these muscles can only function with proper nerve impulses and good blood supply.
The lips receive most of their blood supply from the labial arteries. Due to the various branches, the labial arteries can efficiently provide blood to the lips. Aside from providing blood to the lips for proper function, the blood flow also contributes to the color in the lips. Adequate blood supply is required to maintain appropriate functioning, including breathing, eating, and facial expression.
Structure and Function
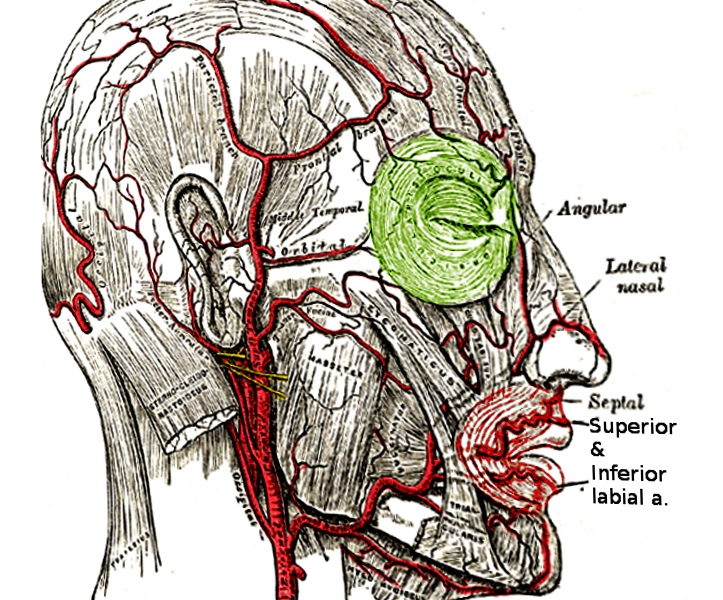
The labial arteries are direct branches from the facial arteries. The labial arteries can further subdivide into the superior labial arteries and inferior labial arteries. The superior labial arteries are larger than the inferior labial arteries. The labial arteries branch from the facial artery at the region where the vermillion border of the upper lip meets the vermillion border of the lower lip. The superior labial artery traverses between the mucosal and upper part of the orbicularis oris muscle. The inferior labial artery traverses between the mucosal and lower part of the orbicularis oris muscle. As the labial arteries traverse the lips, they will anastomose with the labial arteries of the contralateral side. The anastomosis forms collateral blood flow for the lips and underlying muscles.
The superior labial arteries form a network around the upper lip. This network contains many branches that contribute to the blood supply for the upper lip, mucosal, and nose. Many small septal branches will provide blood to the lip. Once the superior labial artery reaches the philtrum, it gives off the columellar artery. The columellar artery ascends the philtrum column up to the nasal septum. At the nasal septum, the columellar arteries and septal branches become part of the Kiesselbach plexus at the anterior part of the nasal septum.
The inferior labial artery traverse the lower lip and fuses with the mental branch of the inferior alveolar artery and the inferior labial artery on the contralateral side. The anastomosis form by the inferior labial arteries supplies the lower lip and the chin region.
Embryology
Blood vessels derive from mesenchyme tissue during development. The blood vessels of the face and head originate from the mesoderm of the brachial arches. The labial artery arises from the third brachial arch. The third branchial arch forms the common carotid artery. The common carotid artery goes on to divide into the internal and external carotid arteries. As the external carotid artery ascends the face, it branches into the facial artery. The facial artery will give rise to the labial arteries. The labial arteries will develop from the angiogenesis effects exerted on the maxillary and mandible regions. The maxillary processes migrate to fuse with the intermaxillary process. During the migration, the blood supply will form and migrate with the maxillary processes. After the fusion of the maxillary processes, the anastomosis of the superior labial arteries eventually follows. The inferior labial artery migrates as the mandible migrate to fuse with the contralateral side. After the mandible fuses to form the mandibular symphysis, the inferior labial arteries eventually anastomose together.
Blood Supply and Lymphatics
The labial arteries are branches from the facial artery.[1] The facial artery provides the blood supply for the labial arteries. The labial artery perfuses the lips, nose, and muscles around the lip region. The upper lip region receives blood from the superior labial artery. As the superior labial artery traverse across the upper lip, it will anastomose with the Kiesselbach plexuses and the contralateral superior labial artery. The superior labial artery's anastomosis with the Kiesselbach plexus via septal branches and the columellar branch provide the nasal septum with blood. The ala of the nose will also receive blood from the septal branches of the superior labial artery. The anastomosis between the two labial arteries provides collateral blood flow to each other.[2]
The inferior labial artery branches off the facial artery around the same region as the superior labial artery. The main difference in that the inferior labial artery will traverse inferior to the lower lip. The inferior labial artery anastomoses with the contralateral inferior labial artery and mental arteries.
The branching of the labial arteries from the facial artery and the anastomoses with the contralateral side forms a network around the lips. This network helps perfuse the lips and the muscles in this region. The anastomose network of vessels can provide blood flow to either side if one side becomes compromised.
The lymphatic drainage system for the lips is divide by the upper and lower lips. The upper lip drains into the submandibular, infraparotid, and the preauricular lymph nodes. While the lower lip drains lymph fluid into the submental and submandibular lymph nodes. These lymph nodes eventually drain back into the thoracic duct on the left side or the right lymphatic duct on the right side.[3]
Nerves
The nerve that is involved in opening and closing the mouth is the trigeminal nerve. This nerve innervates the muscles used for mastication. The lips are only involved because the muscle around the lips is a sphincter used for eating and speaking. The muscle that is around the lips is the orbicularis oris; this muscle acts as a sphincter muscle. The orbicularis oris muscle receives innervation from the facial nerve. The facial nerve also innervates muscles that attach to or close to the lips used in facial expression.[4]
Muscles
The primary muscle that is around the lips is the orbicularis oris muscle. This muscle is a sphincter muscle that is involved in the opening and closing of the mouth. The main blood supply for the orbicularis oris muscle is from both the superior and inferior labial arteries.
Some muscles influence the action so the lips in facial expression due to their attachments. Due to the attachments from the levator labii, the zygomaticus minor, the zygomaticus major, and the levator anguli oris, they act on the orbicularis oris in laughing and smiling. While the depressor anguli oris and the depressor labii inferioris muscle act on the orbicularis oris in sadness and frowning.
Physiologic Variants
The size of the superior labial artery and the inferior labial artery may vary from person to person. The branches that come off the superior labial artery that supply the ala of the nose can sometimes branch directly from the facial artery.[5] In congenital anomalies, there may be an absence in anastomoses between the labial arteries such as cleft lip.
Surgical Considerations
Patients born with cleft lip deformities may undergo reconstruction of the defect. The anatomy of the superior labial artery is altered in cleft lip patients. They may lack the anastomosis between the two superior labial arteries.[6] In the reconstruction process, the superior labial arteries may or may not be anastomose together. With this in mind, proper precautions are taken when dissecting close to the superior labial arteries because there may not be any collateral blood flow.
In plastic surgery, the facial artery's pulsatile motion may create an undesirable appearance unilaterally. The ligation of one facial artery usually causes no severe consequences because of the collateral blood flow from the contralateral facial artery's branches.[7] Another cosmetic procedure is lip fillers, with the knowledge of the anatomy of the labial arteries, which can provide maximally aesthetic appearance with optimal safety. Since the labial artery is deep in the lips, fillers may be injected superficially without damaging the underlying arteries.[8]
As for traumatic damage to the lips that require reconstruction. Reconstruction of the lips has a good prognosis because of the vast blood supply in the lips promoting proper perfusion and a quicker healing process.[2][9][10]
Clinical Significance
Since the blood supply in the lips is from the labial arteries, the lips appear pink with adequate perfusion and blue in ischemia or hypoxia. The appearance of the lips can be a supporting indicator of the perfusion and oxygenation status in a patient.[11]
The lip is a vascular region of the face formed from the network of arteries. When it comes to lip laceration or trauma, compressing the bleeding lip may require more pressure and time to achieve hemostasis.[12]
Other Issues
Since the main vessel that supplies the labial arteries with blood is the facial artery. Damage to the facial artery or any location proximal to the labial arteries results in compromised blood flow. Compromised of blood flow to the labial arteries can come in many forms. Neoplasm, trauma, and infection can cause occlusion or reduced blood flow to the labial arteries; this may result in a decrease in metabolic activities of the tissues in the mid-face region.
The Kiesselbach plexus contains a branch of the superior labial artery. If this plexus is damaged, the anterior nasal septum may bleed. Anterior nasal bleeds usually come from the Kiesselbach plexus. These bleeds tend to occur in children due to mechanical nasal trauma. Fortunately, anterior nasal bleeds are controllable with compression, packing, or chemical cauterization.