Continuing Education Activity
Tip-shaping or refinement is a common request during a consultation for cosmetic nasal surgery. However, surgery of the nasal tip has a unique set of functional and aesthetic challenges that must be understood by the rhinoplasty surgeon to ensure a successful outcome. Unfortunately, poor nasal tip cosmesis or function is a frequent factor leading dissatisfied patients to seek secondary or revision rhinoplasty surgeries. Understanding the anatomic relationships of the nasal tip allows the surgeon to perform maneuvers to create the desired aesthetic changes while preserving critical function. This activity highlights the role of the interprofessional team in rhinoplasty.
Objectives:
- Review the relevant anatomy for performing nasal tip rhinoplasty.
- Describe the mechanisms of nasal tip support and the effects of various surgical techniques on tip support.
- Summarize surgical concepts and outline specific techniques commonly employed in nasal tip rhinoplasty.
- Outline post-surgical care for patients requiring rhinoplasty tip-shaping surgery.
Introduction
Tip-shaping or refinement is a common request during a consultation for cosmetic nasal surgery. However, surgery of the nasal tip has a unique set of functional and aesthetic challenges that must be understood by the rhinoplasty surgeon to ensure a successful outcome. Unfortunately, poor nasal tip cosmesis or function is a frequent factor leading dissatisfied patients to seek secondary or revision rhinoplasty surgeries. Understanding the anatomic relationships of the nasal tip allows the surgeon to competently perform the surgical maneuvers required to create desired aesthetic changes while preserving function.
Anatomy and Physiology
The nasal tip is a pyramidal structure emanating perpendicularly from the plane of the face. The key anatomic structure is the unit formed by the paired lower lateral or alar cartilages. Their lateral crurae sit above the alar creases on either side of the nose, with the medial crurae resting adjacent to each other and forming the structure of the columella; between the medial and lateral crura are the domes, or intermediate crura, which underlie the tip-defining point of the nose. The paired alar cartilages together are frequently thought of as a tripod structure, or alternatively, as an "M-arch," with the domes at the peak of the structure and the bilateral lateral and paired medial crura forming the arms of the tripod or arches.[1] This structure provides support to the position of the tip as well as structural support of the nasal valves intranasally. Understanding the relationship of the lower lateral cartilages to the external appearance of the nasal tip takes experience and often challenges the surgeon to develop enhanced three-dimensional perceptual abilities.[2][3]
The arch of the alar cartilages is supported in space through its attachments to different structures, which contribute to the support in the nasal tip.[4] Understanding the mechanisms of nasal tip support is fundamental to the rhinoplasty operation. The most structurally significant factors are considered "major" tip support mechanisms. These include:
- The shape, size, and strength of the alar cartilages themselves
- The attachment of the medial crura to the caudal septum
- The attachment of the cephalic margins of the lower lateral cartilages to the caudal borders of the upper lateral cartilages, also known as the scroll region
So-called "minor" tip support mechanisms include the anterior nasal spine, the lateral sesamoid cartilages, the interdomal ligaments, the caudal membranous septum, the dorsal septum, and the skin and soft tissue envelope overlying the nasal tip. It is essential to realize that different support mechanisms may take on relatively more or less importance in a given patient.
Disruption of the structures mentioned above will have predictable effects on nasal tip support, and therefore projection. In general, adequate tip support must be reconstituted at the end of a rhinoplasty operation. A slew of secondary problems, both aesthetic and functional, can be traced back to overaggressive manipulation that disrupts tip support. Preoperative support assessment can be performed by evaluating tip recoil on physical examination, carefully studying the preoperative photographs, and thoroughly understanding the numerous patient factors that affect tip support, such as ethnicity, skin thickness, individual anatomy, and prior surgical procedures or trauma.
One critical anatomical concept to understand is that the alar rims are only comprised of soft tissue and lack any cartilaginous structure because the lower lateral cartilages curve cephalically. Therefore, the surgeon needs to consider the effect of changes made to the alar cartilages on the caudal alar margins, realizing that they lack strong support. Failure to recognize this has both aesthetic and functional implications. Upward migration of the alar margins, or alar retraction, is aesthetically displeasing. From a functional standpoint, the external nasal valve is particularly susceptible to damage, resulting in unacceptable postoperative problems with nasal breathing.
Indications
Nasal Tip Analysis
The nasal tip should be evaluated utilizing standardized digital photography in the frontal, base, and bilateral oblique and lateral views. The patient must be positioned in the Frankfort horizontal plane (in which a line between the patient's porion and orbitale is parallel to the floor) to ensure consistency of pre-and postoperative photo documentation. Dynamic assessment of the nasal valve should also be performed, which can include close-up photography of inspiratory and expiratory phases and/or performance of a modified Cottle maneuver, in which the nasal valve is supported gently during respiration, without lateralization of the nasal sidewall, and any subjective improvement in nasal breathing is noted.
The lateral view demonstrates tip features such as projection, rotation, and alar-columellar relationship. This is often the most important view from a patient's perspective. Still, it is important to remember that nasal aesthetics in a real-world social environment are never perceived solely in profile.
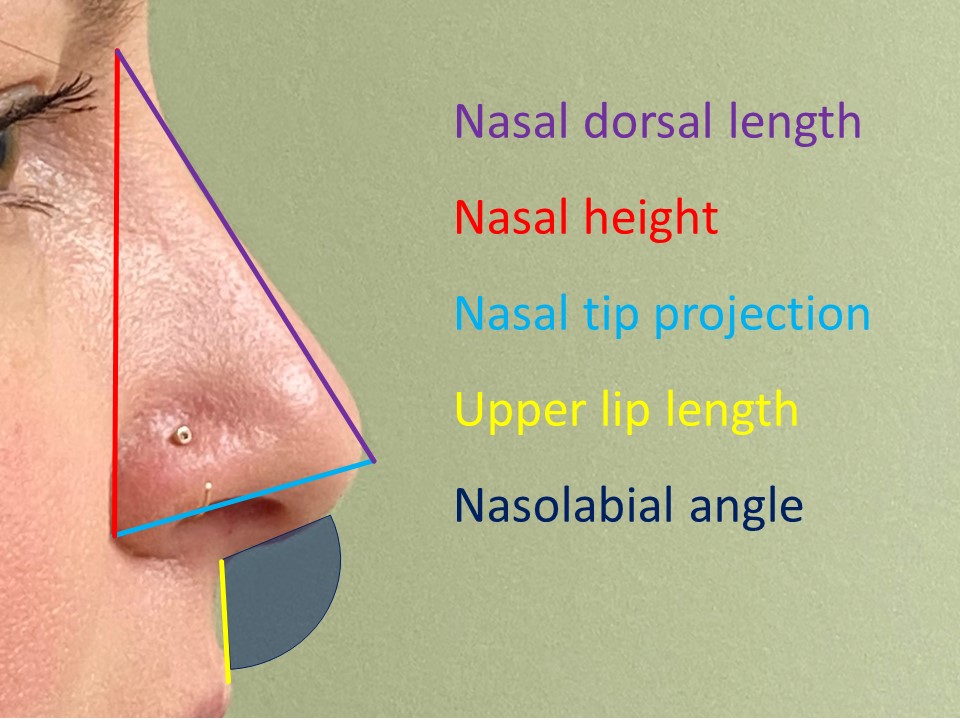
Projection is defined as the horizontal distance the nasal tip protrudes into space measured from the base of the columella. Multiple methods are used to describe ideal projection in a Caucasian nose. Crumley envisioned a 3-4-5 right triangle, wherein the projection is the base of the triangle, with a relative length of 3 units when compared to the height of the nose, which has a relative length of 4 units, and the length of the nose, which has a relative length of 5 units.[5] A similar method described by Goode compares a line drawn from the nasal tip to the alar-facial groove is 55 to 60% of the length of the nose from nasion to tip. In yet another method, Simons described tip projection measured from the subnasale equaling the length of the upper lip, as measured from the subnasale to the upper vermilion border. These methods are mathematically similar and academically useful but are ultimately supplanted by experience as the rhinoplasty surgeon develops his aesthetic sense and surgical skill. It is also important to remember that projection is often subject to patient preference and social and cultural considerations, and perception of nasal tip projection is easily affected by factors such as upper lip length and chin projection.
Rotation is understood as the angle between the upper lip and the nasal tip. Acceptable angles are sociocultural and gender-dependent and are generally accepted to be 90 to 95 degrees in men and 95 to 115 degrees in women. The upper end of the range is more acceptable for shorter women. An overrotated nose is a telltale sign of a poor rhinoplasty operation, as this appearance is highly unnatural and indicative of overly aggressive surgery.
The alar-columellar relationship is another important feature visualized on the lateral view. Disproportion is recognized as an excessive, typically greater than 4 mm, amount of caudal septum visible in this view. The surgeon must decide if the disproportion is due to retraction of the alar rim or excessive show of the columella, or both. A hidden columella occurs when the columellar show is less than 2 mm and can result from a hanging ala, a retracted columella, or both.[6] Appropriately diagnosing the underlying cause of the disproportion is the key to its correction. An oblique line drawn from the posteroinferior aspect of the nasal vestibule to the anterior apex can serve as a guide for determining the nature of the problem; if more columella is visible above the line, the ala is retracted; if more columella is visible below the line, the columella is hanging.
The transition from the tip lobule to the nasal dorsum is a key aesthetic feature. An ideal nasal profile has a straight transition to the tip or a slight supratip depression or "break." Convexity or fullness in this area is perceived as aesthetically displeasing and known as a "pollybeak" deformity because it resembles a parrot's beak.[7]
The postoperative pollybeak deformity is a well-described phenomenon that illustrates the challenges inherent to nasal tip surgery. When it occurs in this setting, there are three common reasons for fullness in the supratip:
- Inadequate resection of the cartilaginous portion of a dorsal hump or over-resection of the bony component
- Soft tissue fullness in the supratip, usually due to scarring
- Postoperative tip ptosis secondary to a failure of tip support
A severe depression in the supratip area is also not ideal and is termed a "saddle nose" deformity. This can indicate an underlying nasal structure lacking in support or significant over-projection of the tip itself. The apparent depth of a saddle nose may be augmented by a dorsal hump located just superior to it; likewise, a subtle saddle may bring attention to what would otherwise be an inapparent hump.
Similarly, inferior to the tip-defining points of an idealized nose, the infratip lobule transition to the columella on lateral view should possess a slight angulation; this finding, in conjunction with a supratip break, is often known as a "double break." This is one of the many nuanced aspects of tip aesthetics that is appreciated by the expert surgeon. Flattening the infratip lobule with loss of the double-break aesthetic leads to excessive sharpness of the nasal tip.
The base view provides important information on tip shape, projection, deviation, the contour of the medial crura, lateral wall support, and nasal valve function. Postoperatively, it allows the surgeon to evaluate the scar used for open approaches. An equilateral triangle with a columella to infratip lobule ratio of 2 to 1 is considered ideal on this view. Tip maneuvers, particularly those in which the domes are moved laterally or medially along the lower lateral cartilages (the so-called "steal" maneuvers), or in which the medial crura are moved significantly (such as via tongue-in-groove suturing), can potentially alter this relationship and should be accounted for during the tip surgery. Additionally, the medial crural footplates can contribute to nasal obstruction and hint at important operative factors such as a deviated caudal septum or relative weakness of tip support, in the case of short medial crura.[8][9] The lateral walls can be assessed from this vantage for weakness, especially when coupled with dynamic inspiratory base view photography, which can often demonstrate the collapse of the nasal valve. Obstructive curvature of the lower lateral cartilages directly into the nasal airway can also be seen in this view.
Oblique or three-quarter views provide complementary information and are particularly important because it is in this view that most observations of the nasal tip are made in real-world social settings. The tip of the nose is the distal end of the aesthetically important brow-tip aesthetic line, which should proceed symmetrically and smoothly along the dorsum. The alar margins can be viewed as well from this perspective.
The frontal view deserves special consideration. Frontal view aesthetics are often the most subtle and require a superior understanding of three-dimensional spatial relationships. A general assessment of symmetry and straightness should also be made, and the alar margins should be evaluated for a asymmetric "gull in flight" appearance. In a White patient or leptorrhine nose, the width of the nasal base (as measured from the lateral aspect of one ala to the other) should correspond to the intercanthal distance. The nasal base will be slightly wider in a platyrrhine patient, often of sub-Saharan African descent, corresponding to the distance between the lacrimal caruncles. Patients of Asian or Latin descent with mesorrhine noses will have a nasal base of intermediate width. These basic assessments of the nasal tip on the front view should be made routinely. Still, an expert rhinoplasty surgeon should assess the shape of the tip with a higher-order aesthetic sensibility.
Seminal work by Dean Toriumi modernized the practice of aesthetic nasal analysis.[10] The ideal tip shape is best understood in two dimensions by describing the way light and shadow interact on the nasal topography. Under standard lighting conditions for digital rhinoplasty photography, the nasal tip should exhibit a central highlight, representing the paired domes underlying the skin envelope. This highlight should be oval-shaped and symmetric, with the long axis oriented horizontally. This tip highlight should be in continuity with the paired brow-tip aesthetic lines, which terminate in a slight flare caudally to create the tip highlight. Lateral to the tip, the sidewalls of the nose should taper uninterrupted towards the face, resulting in an even shadowing that is symmetric bilaterally. Immediately superior to the tip should be a horizontally oriented demarcation or shadowing representing the recessed area of the supratip break. The key understanding is the transition of the tip highlight to the shadows of the nasal sidewalls, where the lower lateral cartilages traverse posteriorly towards the sesamoid complexes and nasofacial junction. The curvature, symmetry, and orientation of the lower lateral cartilages affect this transition area and are frequently overlooked and, therefore, may be inadequately addressed during rhinoplasty. Many preoperative and postoperative tip deformities are evident if one studies this area routinely. Understanding the relationship of the underlying structure to the surface anatomy in this area is the key to achieving excellent front view tip aesthetics.[10][11]
By understanding frontal view nasal appearance, one should be able to appreciate the orientation of the lower lateral cartilages. A simple way to think about orientation is whether the long axis is oriented toward the medial or lateral canthus. A more horizontal or caudal orientation of the lower lateral cartilages has an ideal configuration for both aesthetics and function, allowing for a smooth transition from the tip to the sidewall and providing stronger support to the caudal alar margin. In cephalically oriented lower lateral cartilages, the caudal border can be visible, disrupting the smooth transition to the nasal sidewalls. When this malorientation is severe and bilateral, it gives the appearance of open and closed parentheses, defined by lateral shadowing at the caudal border of the cartilages. The cephalically oriented structure provides less support to the caudal alar rim due to the increased distance from the caudal edge of the cartilage in this configuration. Over-resection of cephalically oriented lower lateral cartilages can lead to exaggerated parenthesis deformities, alar retraction, and deficiencies of the external nasal valve.[10][12]
Contraindications
Contraindications to rhinoplasty follow general guidelines for any elective surgery. The patient must be sufficiently healthy and motivated to undergo elective rhinoplasty surgery, typically under general anesthesia. The surgeon should also consider any adverse psychological features that may portend a poor outcome, such as unrealistic expectations, severe depression, or body dysmorphic disorder. A good method to assess patient expectations is to ensure that the patient's and the surgeon's goals for the operation are clearly defined and agreed upon before an operation is planned. The liberal use of digital photography and computer imaging improves communication regarding surgery goals and allows the surgeon to proactively manage expectations and screen for potential problems. That said, it should be emphasized that digital photograph manipulation is a useful tool for creating a shared understanding of surgical goals rather than a guarantee of post-operative appearance.
The additional complexity of secondary or revision cases should be respected as the risk of complications increases significantly in these cases.[13][14] The cartilaginous work itself is frequently challenging, sometimes requiring complete reconstruction of one or more anatomic units.[13] Repeated dissection of the soft tissue envelope may disrupt the vascular supply of the nasal skin, which runs within the superficial musculoaponeurotic system (SMAS) and result in life-altering skin necrosis requiring major reconstruction and a permanent loss of normal appearance. Healing and remodeling of the tissues are less predictable after revision surgeries and, combined with the more technically demanding surgical techniques often required, can lead to frustrating aesthetic or functional problems. Revision surgery requires an overall greater level of surgeon experience to achieve good outcomes; therefore, it is appropriate for the surgeon to approach these cases with a conservative mindset.[15]
Another potential relative contraindication for rhinoplasty is smoking. Many surgeons refuse to perform rhinoplasty on patients who are actively smoking and require that surgical candidates stop all tobacco product use for a certain period of time before and after surgery to reduce the risk of wound complications. An increasingly large body of literature suggests that wound complications or poor functional outcomes are no more likely in patients who smoke than those who do not, possibly due to the robust blood supply of the face.[16][17][18][19] That said, smoking cessation should always be encouraged due to its myriad health benefits and reduction of perioperative cardiopulmonary risk.
Equipment
The following equipment is required:
- Local anesthetic: 1% lidocaine with 1 to 100,000 epinephrine
- Cottonoid pledgets with 0.05% oxymetazoline HCL or 4% cocaine
- Fine tip skin marker
- Knife handles: #3 and/or #7 Bard-Parker handles, Beaver blade handle
- Scalpel blades: #15, #15C, #6700 Beaver or similar
- Bipolar electrocautery
- Scissors: Wilmer, Converse, Giunta, Joseph, iris, tenotomy
- Forceps: Adson-Brown, Cushing-Brown bayonets, 0.5 mm Castroviejo
- Retractors: Aufricht, Bernstein, Gruber
- Elevators: Woodson, Cottle, Freer, Pierce, Joseph
- Skin hooks: Joseph 2, 7, and 10 mm, Guthrie
- Specula: Cottle, Vienna, Killian
- Suction: 8 French Frazier tip
- Freer septal knife
- Cottle cartilage crusher
- Tebbetts caliper
- Needle drivers: Halsey, Webster, Castroviejo
- Sutures: 6-0 polypropylene, 6-0 plain gut, 5-0 polydioxanone, 5-0 chromic gut, 4-0 chromic gut, 3-0 nylon
- Septal splints
- Tape strips
- Thermal cast
Personnel
The following personnel is required:
- Surgeon
- First assistant
- Surgical technologist
- Circulating nurse
- Anesthesia provider
Preparation
The patient is placed supine on the operating table and intubated orally, with the tube taped to the midline of the lower lip to avoid distorting the nose. The eyes are protected with adhesive film dressings or tape strips, and the face is prepped with 10% betadine or 70% isopropyl alcohol, taking care to avoid exposing the corneas to the antiseptic solution. A local anesthetic is injected, and the nose is packed with cottonoid pledgets soaked in a vasoconstricting agent prior to beginning the surgery.
Technique or Treatment
Approaches
The tip can be surgically exposed through endonasal (closed) or open (external) approaches. Closed or endonasal approaches are classified as either non-delivery or delivery approaches.
Non-delivery approaches minimize surgical exposure and are therefore appropriate for patients with minimal bulbosity or other deformities of the nasal tip and who display symmetric triangularity on base view. Two types of incisions can be utilized that further subdivide non-delivery approaches into cartilage-splitting and retrograde. The cartilage splitting technique utilizes a transcartilaginous (through lateral crura of the lower lateral cartilages) incision placed 5, not 8 mm cephalic to the caudal margin of the lateral crus. The retrograde technique utilizes an intercartilaginous incision through the scroll region between upper and lower lateral cartilages, with retrograde dissection (cephalic to caudal) of the lateral crus as necessary to access the cephalic margin of the lower lateral cartilages.
In contrast, the delivery approach provides greater exposure of the alar cartilages. Intercartilaginous incisions are combined with marginal incisions along the caudal margin of the lower lateral cartilages to expose the lower lateral cartilages as bipedicled chondrocutaneous flaps. As a result of the increased exposure, more extensive nasal tip modification can be performed under direct visualization.
The incisions of the closed approaches are usually combined with a high partial or full transfixion incision to provide access to the nasal dorsum and caudal septum to allow for additional modification of the nasal tip geometry.
Closed approaches benefit from reducing soft tissue manipulation and disruption of tip support, which may expedite healing and recovery. However, closed approaches limit surgical exposure, which may, in turn, limit the extent to which the nasal tip can be accurately or symmetrically modified.
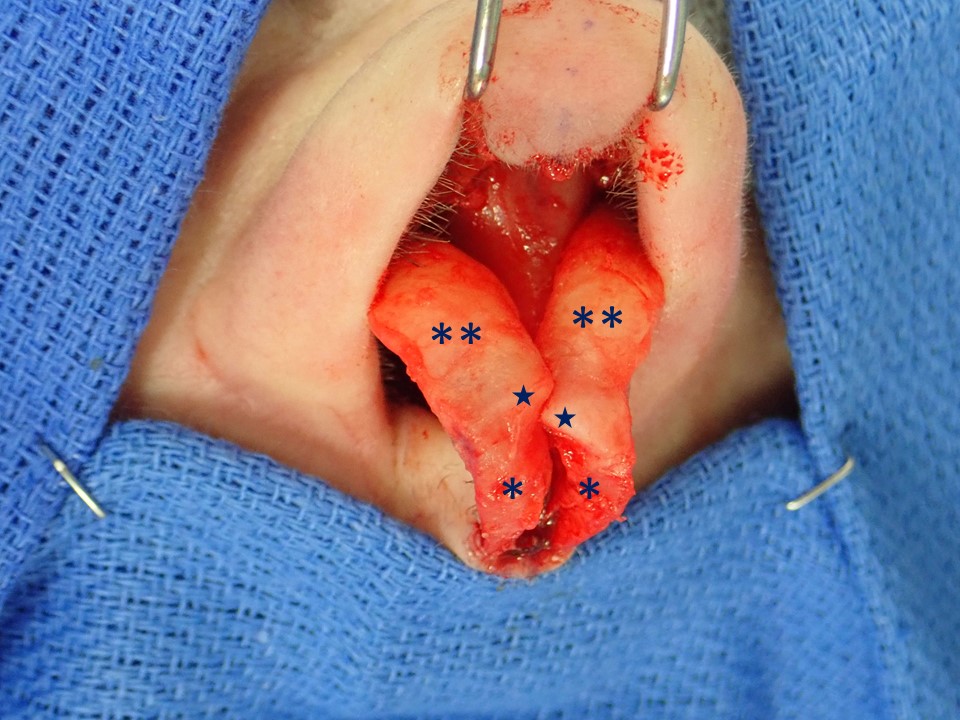
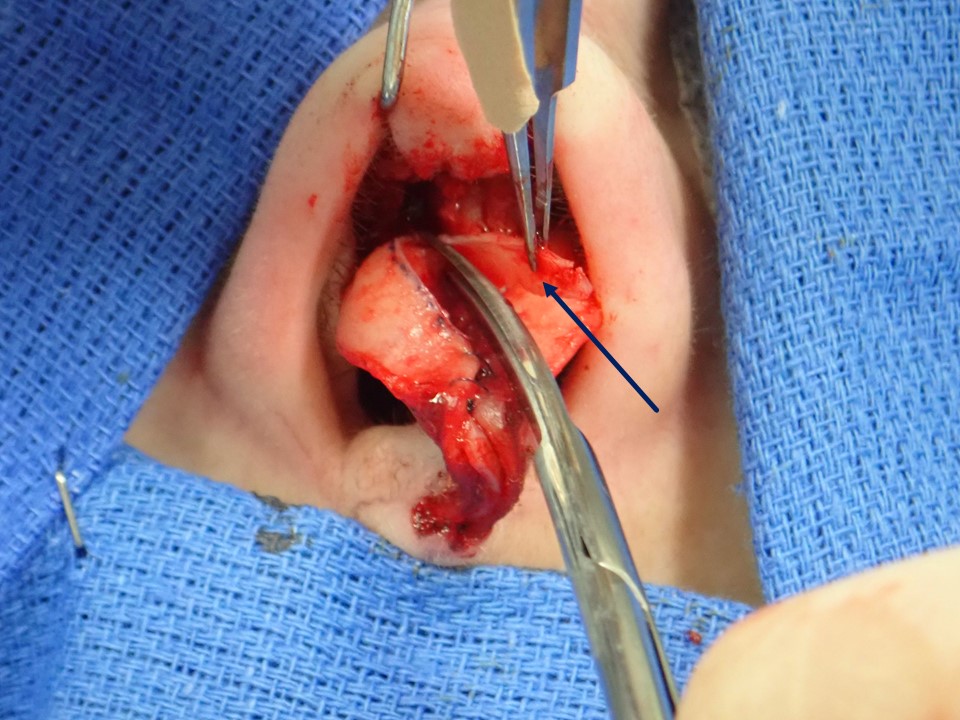
In contrast, the open or external approach provides the greatest exposure of the nasal framework. Marginal incisions are combined with a transcolumellar incision to elevate the skin-soft tissue envelope from the nasal framework in a sub-SMAS plane. The nasal tip cartilages can be viewed completely and manipulated in an anatomic position without tension. Disadvantages include a columellar scar, prolonged postoperative edema, and increased operative time. Importantly, anatomical tip support mechanisms are disrupted to a greater degree in the open approach and need to be reconstituted during the procedure to prevent postoperative loss of tip support. A distinct advantage of this approach is its unparalleled exposure, particularly useful for teaching rhinoplasty to trainees.
Specific Surgical Techniques
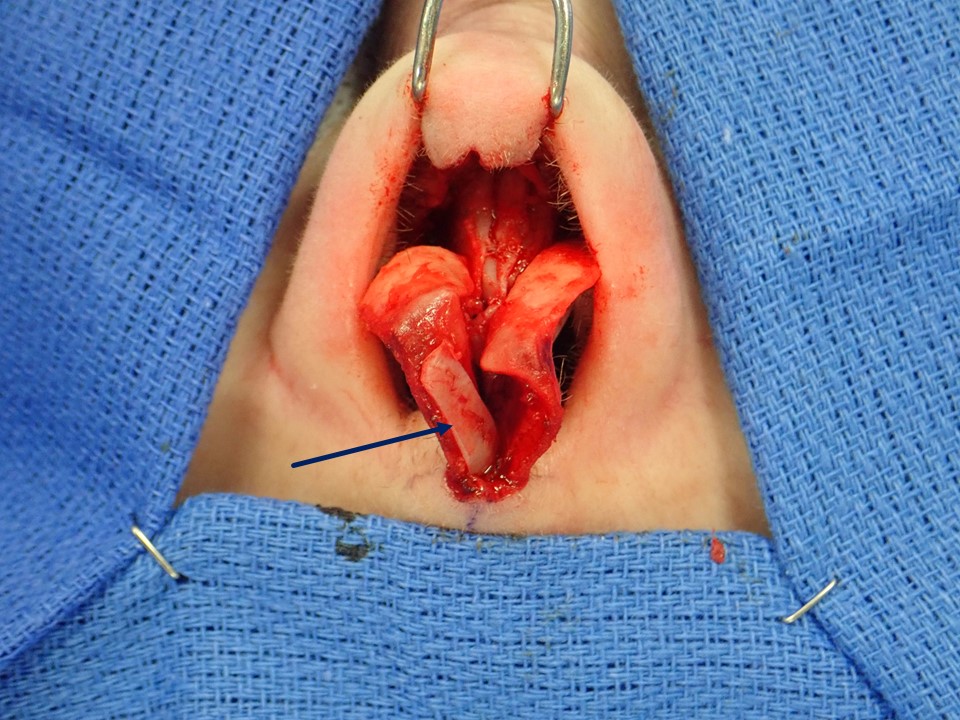
A discussion of surgical techniques to modify the nasal tip is a nearly inexhaustible topic.[10][20][21][22][23][24][25][26][27] To facilitate thinking about nasal tip surgery, it is helpful to recall the tripod theory discussed above. In this simplified model of tip structure, the tip is imagined as a familiar camera tripod, in which the two superolateral legs are comprised of the bilateral lateral crura of the lower lateral cartilages. In contrast, the inferomedial leg is comprised of the paired medial crura of the lower lateral cartilages within the columella. Understanding this idea allows one to understand that procedures modifying the lateral legs of the tripod primarily affect rotation, with a secondary effect on projection, while procedures modifying the medial leg primarily affect projection, with a secondary effect on rotation. It is also critical to understand that altering the position of the domes themselves can achieve desired changes in projection or rotation. "Steal" techniques utilize suture recruitment of either lateral or medial alar cartilage to reposition the domes laterally or medially, thus altering the configuration of the lateral, intermediate, and medial segments of the alar cartilages. "Overlay" techniques are more destructive to the lower lateral cartilage but allow for more significant changes to projection or rotation. In these techniques, the lateral crus or medial crus is elevated from the underlying mucosa, then transected and sutured back together in a shortened, overlaid configuration. More advanced lateral crural tensioning techniques and lateral crural repositioning techniques also typically allow the surgeon to define the dome segment more precisely, regardless of the original dome position.
A philosophically distinct category of tip shaping techniques relies primarily on grafting techniques to obtain desired changes.[25][26][27] These techniques are augmentation procedures by definition and can be very effective. The surgeon must still consider the downsides of adding bulk to the nasal structure or the risk of distortion, warping, and excessive skin contraction resulting in visible grafts or other aesthetic deformities.
Tip techniques are numerous and can be combined in nearly infinite variations. Reductive techniques are frequently combined with grafting to create structural support and aesthetic change. While reduction techniques have classically accounted for most rhinoplasties, cartilage augmentation has become more fashionable over the last decade or two, relegating aggressive reduction rhinoplasty to cases of very large noses and facial feminization for transgender patients.
Managing Tip Projection
Projection is generally described as "adequate," "excessive," or "inadequate." The alar cartilages and tip support mechanisms are the primary considerations when thinking about nasal tip projection. The surgeon should also consider the role of the premaxilla in the projection of the nose, particularly when congenital craniofacial abnormalities, however mild or subclinical, are present. The surgeon should also be aware of overall facial proportions that can affect the perception of nasal projection (e.g., a high radix reduces the nasofrontal angle and leads to the appearance of under projection, while a retruded chin causes the nasal tip to seem more projected).
Underprojection requires augmentation, and this is typically accomplished using suture techniques or grafts. Lateral crural steal, tip sutures, tip grafts, columellar struts, caudal septal extension grafts, and lateral crural tensioning techniques help increase tip projection. Medial crural sutures and tip sutures, including interdomal sutures and transdomal sutures, can achieve a limited increase in projection, usually about 1 to 2 mm. Projection beyond this limit typically requires grafting. Cap grafts, onlay tip grafts, and shield grafts directly augment the nasal tip but run the risk of visibility or asymmetry. Columellar strut grafts, extended spreader grafts, and caudal septal extension grafts can be used as vertical anchors to advance the domes into a more projected location and serve a more structural role projecting the tip. Lateral crural tensioning recruits the lateral crura to a projected position on a caudal septal extension graft to provide tension to the lateral cartilage and reduce bulbosity of the lateral tip. Lateral crural repositioning allows the surgeon to place the tip in essentially any position desired; the caudal septal extension graft is the structural support that allows for this.
Excessive nasal tip projection results from overlong medial and lateral crura or projection of the anterior septal angle. Lateral or medial crural overlay techniques directly address the elongated cartilages, as does lateral crural repositioning, which allows for tailoring the cartilages to a precise length. Reducing the projection of the anterior septal angle is straightforward, although one should keep in mind that inadequate reduction of the dorsum just cephalic to this region can result in pollybeak deformity postoperatively; however, this should be apparent before the conclusion of the operation. The common "tongue-in-groove" setback technique is a powerful method to manage the nasolabial angle, increase rotation, and reduce columellar show. A posterior vector of the setback of the medial crura tends to deproject the domes, which, depending on the goals of the operation, typically need to be reconstituted in a relatively projected position to restore the original projection or to increase the projection. Lateral crural recruitment into the new dome is usually required to accomplish this. This deproject-reproject maneuver is a good example of the dynamics that must be respected to precisely manage the appearance of the nasal tip.
It is important to consider the effects of disrupting tip support on tip projection. For example, nasal spine reduction reduces a minor tip support mechanism and can result in some degree of deprojection. A full transfixion incision in the endonasal approach reduces projection by a similar mechanism. However, perhaps more relevant to the rhinoplasty surgeon is the matter of postoperative loss of tip projection, an insidious and exceedingly common clinical challenge directly related to loss of tip support during standard surgical maneuvers. The open approach is especially prone to this phenomenon, which usually manifests as the subtle and progressive development of a supratip fullness in the months following surgery. Again, the surgeon must understand tip support mechanisms to negotiate this challenging arena of tip dynamics successfully.
Managing Tip Rotation
Rotation of the nose is a frequently desired surgical outcome, especially in female rhinoplasty patients. However, rotation maneuvers must be treated with respect. Excessive rotation of the nose is a classic hallmark of the "overdone" nose job. Mercifully, these aggressive techniques have been replaced, emphasizing natural, ethnically appropriate aesthetics in the modern era. Changing rotation involves altering the angular relationship between the caudal septum and the alar cartilages. The common "tongue-in-groove" medial crural setback technique directly changes this relationship, typically resulting in nasal rotation. Techniques that mobilize the alar cartilages include lateral crural steal, which recruits lateral cartilage into a more projected and rotated neodome, and lateral crural overlay, which rotates and secondarily deprojects the tip complex by shortening the lateral legs of the tripod.[9]
Simple suture techniques of the domes coupled with cephalic trimming can also affect a small degree of rotation. Manipulations of the anterior septal angle and caudal septum are also used to increase rotation. Columellar struts, and more significantly caudal septal extension grafts, provide a rotational force to the tip complex.[10] Base-up triangular resection of the caudal septum results in rotation since more cartilage is removed at the anterior septal angle relative to the posterior septal angle. Lateral crural tensioning and lateral crural repositioning techniques use the caudal septum or caudal septal extension graft to place the tip in the desired position, either rotated or counterrotated - the latter requiring a more substantial extension graft. Finally, the nasolabial angle itself can be augmented with a plumping graft, which pushes the junction of the columella and upper lip anteriorly and creates a more obtuse-appearing angle without actually altering the position of the domes.
Counterrotation is a common goal of secondary rhinoplasty surgery, where prior surgeries have left the tip unacceptably overrotated. Frequently, a lengthening of the nose is simultaneously required in this setting, and for this reason, counterrotating a surgically overrotated nose is considerably more challenging than achieving rotation. Again the relationship between the caudal septum and alar cartilages controls the degree of rotation. A medial crural overlay will deproject the nose and secondarily counterrotate the tip. Tip grafts placed anteriorly over the domes or medial crura (shield grafts, infratip lobule grafts) can mildly decrease the rotation of the tip. Caudal septal extension grafts can also be applied to counterrotate the tip by lengthening the caudal septum and anterior septal angle. Loss of tip support, as occurs during dissection in the open approach or during full transfixion incision in the closed approach, resulting in loss of projection, can also cause counterrotation, increasing the potential for a postoperative pollybeak deformity.
Tip Definition
Improved tip definition is a common goal of aesthetic rhinoplasty, but it is the most subjective and nuanced aspect of tip surgery. Any of the standard techniques, if applied injudiciously, can result in an unnatural appearance and even nasal valve problems if severe. A review of the above discussion of frontal view aesthetics is critical to understanding techniques that will create a natural-appearing tip definition.
Various colloquial terminology is applied to describe the surface appearance of the tip: boxy, bulbous, pinched, narrow, wide, asymmetric. The crucial skill in assessing the tip is correlating surgical anatomy to surface anatomy. When the cartilages are exposed, the surgeon should assess the shape, curvature, symmetry, and strength of the lower lateral cartilages and generate a hypothesis on how these features, together with the skin and soft tissue envelope, create the surface appearance. An excessive convex curvature is a frequent culprit resulting in a large, bulbous, or boxy nasal tip and is often caused by excessive length of the lower lateral cartilages. Concavity of the lower lateral cartilages may create a more narrow tip but can obstruct the nasal valves due to the intranasal convexity of the same cartilage. Asymmetry between right and left alar cartilages is common in primary and revision cases. The surgeon will frequently encounter over resected or even absent lower lateral cartilages in revision or secondary surgeries. An understanding of the ideal anatomy of the lower lateral cartilages is essential to their correct reconstruction.
Certain features of the tip are worth contemplating and may be amenable to correction with standard suture techniques. For example, a boxy tip may result from an increased angle of divergence between the domes of the lower lateral cartilages and/or wide dome arc. Various degrees of cephalic trim and suture reconstitution can reduce the dome arc or angle of divergence, resulting in aesthetic tip definition, provided alar cartilages that are otherwise symmetric and have minimal excess curvature as they course laterally. The typical sutures used for this purpose are horizontal mattress dome sutures, interdomal sutures, and sutures between the medial crura, typically with a caudal septal extension columellar strut graft placed between the medial crura. In more extreme cases, particularly non-Caucasian patients with very thick skin and soft tissue, more aggressive maneuvers are required to refine the tip; a classic example is the Goldman tip technique, which involves dividing the domes and suturing them together to create two sharp ridges, which are then visible as tip-defining points.[28] Cephalic trimming of the alar cartilage lateral crura will also help define the tip by reducing supratip bulk; it is important to leave an adequate width of lower lateral cartilage intact for structural support of the nasal valve and alar margins, however, typically 6 to 8 mm. The risk with this technique is that, if applied indiscriminately to every patient, asymmetries and unnatural results in a subset of patients are practically guaranteed, with alar retraction being a common sequela.
An alternative approach to tip definition is seen in the techniques that manipulate the lower lateral cartilages rather than just the dome or intermediate segment. A classic example is lateral crural tensioning. A lateral crural steal mobilizes the dome to a point on a caudal septal extension graft, providing tension or a straightening force to the lateral crura. Lateral crural strut grafting with or without lateral crural repositioning may produce a similar effect as well. Lateral crural strut grafts, or Gunter grafts, directly support the lateral crura on the vestibular side of the cartilage and provide a platform against which convex cartilages can be flattened and supported.[29]
Lateral crural repositioning refers to a technique in which the lower lateral cartilages are released from their lateral piriform attachments, tailored to a specific length and width, and then supported with lateral crural strut grafts repositioned in a favorable orientation. The lateral crura can also be incised via cephalic trimming. Still, if the cephalic cartilage strip is then folded over behind the remaining lateral crus (a cephalic turn-in flap), an effect similar to both cephalic trimming and lateral crural strut grafting is achieved: flattening and narrowing of the lateral crura.[30] The commonality of these techniques is that they each contain a mechanism to flatten the lateral crura, remove asymmetries of the cartilages, and support the sidewalls of the nose. On the surface, this allows for creating a flat, natural transition from the tip highlight through the sidewalls of the nose to the nasofacial junction, a key component of ideal tip aesthetics. Suture techniques with cephalic trimming in the absence of grafting cannot inherently achieve this degree of favorable definition or symmetry, except in select cases.
Postoperative Care
The tip is supported with tape in the immediate postoperative period and a thermoplastic cast placed over the dorsum. If excessive dissection of the lower lateral cartilages is performed, lateral wall splints are applied across the sidewall. All nasal or septal dressings are removed on postoperative day 7. It is important to counsel the patient that nasal tip swelling is frequently the most significant recovery issue from the patient perspective and resolves over a period of many months to years, with fluctuations in swelling commonplace and sensitive to changes in diet, temperature, and activity. Focal areas of problematic postoperative edema can be managed with interventions, including self-massage or nasal exercises, taping, or physician-administered steroid injections. Vigilant follow-up with judicious use of these interventions can lead to improved outcomes. Follow-up with standard digital photography should occur at regular intervals after surgery, ideally over several years. This helps the surgeon understand the relationship between their techniques and the long-term stability of postoperative results.
Complications
Rhinoplasty is an elective procedure, even in cases of significant nasal airway obstruction. In an ethical practice with careful patient selection, complications of tip rhinoplasty surgery are primarily aesthetic or related to nasal breathing, most commonly patient dissatisfaction with or without depression, although certainly epistaxis and infection can occur in the early postoperative setting. It is essential to understand that undergoing a rhinoplasty requires a significant psychological adjustment during the recovery period. This is due to its nature as a “type change” operation as opposed to a procedure that restores the appearance to a prior, younger state with which the patient is already familiar.[31]
It is, therefore, a critical part of the postoperative follow-up period to manage the patient’s expectations and, in many cases counsel patience, because it can take months for a patient to get used to a new nose, even when the rhinoplasty was executed perfectly and heals well. If the patient and surgeon mutually agree that some aspect of the outcome is suboptimal, a revision or secondary surgery can be considered. These should only take place several months to years after the initial surgery, after a time sufficient to reduce edema and accommodate the many nuances of the dynamic healing process, at least 6 to 12 months after the primary operation.
Additionally, the surgeon should have confidence that a particular operative plan has a high likelihood of improving the specific problem to be addressed. In complex secondary or tertiary cases (or beyond), it is critical to understand the limitations of the skin and soft tissue envelope. Irrevocable damage to the blood supply of the skin can lead to unacceptable skin necrosis, with life-altering consequences. A conservative approach to these cases is thus always appropriate; however, with experience and proper diligence, revision rhinoplasty can be rewarding and successful for the patient and the surgeon.
Clinical Significance
According to the American Society of Plastic Surgeons, rhinoplasty was the most common cosmetic surgical procedure in 2020, with 352,555 cases completed in the United States. For rhinoplasty candidates, tip reshaping is one of the most frequent requests encountered during a patient consultation. Surgery of the nasal tip presents a unique set of functional and aesthetic challenges that must be understood by the rhinoplasty surgeon to ensure a successful outcome. Unfortunately, poor nasal tip cosmesis or function is a frequent factor leading dissatisfied patients to seek secondary or revision rhinoplasty. Understanding the anatomic relationships of the nasal tip cartilages allows the successful surgeon to perform the maneuvers that create desired aesthetic changes while preserving critical function.
Enhancing Healthcare Team Outcomes
Nasal tip rhinoplasty is typically an elective, ambulatory surgical procedure. In this setting, the rate of complications must be minimized; an interprofessional team approach likely improves patient safety.
The surgical and perioperative staff should emphasize fluid, closed-loop communication to achieve optimal outcomes. The process begins well before the surgical date. Preoperatively, a multidisciplinary risk assessment is frequently performed, the so-called surgical "clearance." Candidates for elective aesthetic surgery should be acceptably low-risk patients as determined by a primary care physician or another appropriate medical specialist. The surgeon should spend time reviewing the risks of the procedure and clarifying expectations for both long-term results and the immediate postoperative period. A thorough informed consent process should be implemented as a routine part of the surgeon's practice. Instructions for the night before surgery and the recovery process should be discussed in detail. The patient should be provided with written information, and a clear communication plan should the patient need to contact the surgeon emergently.
Before surgery, systematic patient identification procedures should be in place to ensure that the correct procedure is being performed on the correct patient. An additional consent process is usually performed, and the patient should have the chance to address any last-minute concerns or questions. Additionally, any updates to the history and physical examination should be documented. Occasionally, it is necessary to postpone or cancel surgery due to developments in the patient's health after clearance.
In the operating room, "time out" procedures are useful to reduce the incidence of unacceptable wrong-site or wrong-patient medical errors. During surgery, communication among the surgeon, anesthesiologist, surgical scrub technicians, and operating room nursing staff is critical to allow the case to proceed safely and efficiently. Ideally, perioperative staff should already be familiar with the surgeon and the procedure being performed. Delays in the operating room should be kept to a minimum to maximize efficiency and patient safety.
In the recovery area, communication between the recovery staff and the surgeon is critical. The staff should have a reliable means of communication to relay information that may indicate a complication and require an escalation of care and/or transfer to a hospital. Although ambulatory surgery is known to be safe, a streamlined system to address emergencies must be in place. The post-anesthesia care staff should also have a general understanding of the surgeon's recovery protocols because they will often guide the patient at discharge. [Level 3]