[1]
Bargen GA, Chirp-Evoked Auditory Brainstem Response in Children: A Review. American journal of audiology. 2015 Dec;
[PubMed PMID: 26649461]
[2]
Jewett DL,Williston JS, Auditory-evoked far fields averaged from the scalp of humans. Brain : a journal of neurology. 1971;
[PubMed PMID: 5132966]
[3]
Year 2007 position statement: Principles and guidelines for early hearing detection and intervention programs. Pediatrics. 2007 Oct;
[PubMed PMID: 17908777]
[4]
Peterein JL,Neely JG, Auditory brainstem response testing in neurodiagnosis: structure versus function. Journal of the American Academy of Audiology. 2012 Apr;
[PubMed PMID: 22463940]
[5]
Felix RA 2nd,Gourévitch B,Portfors CV, Subcortical pathways: Towards a better understanding of auditory disorders. Hearing research. 2018 May;
[PubMed PMID: 29395615]
Level 3 (low-level) evidence
[6]
Biacabe B,Chevallier JM,Avan P,Bonfils P, Functional anatomy of auditory brainstem nuclei: application to the anatomical basis of brainstem auditory evoked potentials. Auris, nasus, larynx. 2001 Jan;
[PubMed PMID: 11137368]
[7]
Pecka M,Siveke I,Grothe B,Lesica NA, Enhancement of ITD coding within the initial stages of the auditory pathway. Journal of neurophysiology. 2010 Jan;
[PubMed PMID: 19846624]
[8]
Gorga MP,Kaminski JR,Beauchaine KL,Jesteadt W,Neely ST, Auditory brainstem responses from children three months to three years of age: normal patterns of response. II. Journal of speech and hearing research. 1989 Jun;
[PubMed PMID: 2739379]
[9]
Kanji A,Khoza-Shangase K,Moroe N, Newborn hearing screening protocols and their outcomes: A systematic review. International journal of pediatric otorhinolaryngology. 2018 Dec;
[PubMed PMID: 30368368]
Level 1 (high-level) evidence
[10]
Dille MF,Ellingson RM,McMillan GP,Konrad-Martin D, ABR obtained from time-efficient train stimuli for cisplatin ototoxicity monitoring. Journal of the American Academy of Audiology. 2013 Oct;
[PubMed PMID: 24224985]
[11]
Glasscock ME 3rd,Jackson CG,Josey AF,Dickins JR,Wiet RJ, Brain stem evoked response audiometry in a clinical practice. The Laryngoscope. 1979 Jul;
[PubMed PMID: 449545]
[12]
Bauch CD,Rose DE,Harner SG, Auditory brain stem response results from 255 patients with suspected retrocochlear involvement. Ear and hearing. 1982 Mar-Apr;
[PubMed PMID: 7075874]
[13]
Gordon ML,Cohen NL, Efficacy of auditory brainstem response as a screening test for small acoustic neuromas. The American journal of otology. 1995 Mar;
[PubMed PMID: 8572110]
[14]
Gosepath K,Maurer J,Mann W, [Diagnostic intra-meatal acoustic neurinoma--the role of acoustically evoked brain stem potentials and other otoneurologic studies]. Laryngo- rhino- otologie. 1995 Dec;
[PubMed PMID: 8579671]
[15]
Godey B,Morandi X,Beust L,Brassier G,Bourdinière J, Sensitivity of auditory brainstem response in acoustic neuroma screening. Acta oto-laryngologica. 1998 Jul;
[PubMed PMID: 9726673]
[16]
Don M,Kwong B,Tanaka C,Brackmann D,Nelson R, The stacked ABR: a sensitive and specific screening tool for detecting small acoustic tumors. Audiology
[PubMed PMID: 15925862]
[18]
Rouillon I,Parodi M,Denoyelle F,Loundon N, How to perform ABR in young children. European annals of otorhinolaryngology, head and neck diseases. 2016 Dec;
[PubMed PMID: 27453092]
[19]
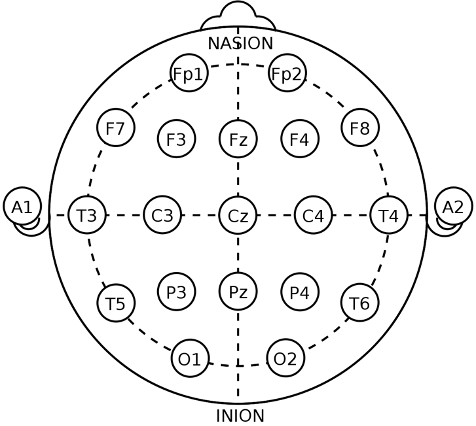
American Electroencephalographic Society guidelines for standard electrode position nomenclature. Journal of clinical neurophysiology : official publication of the American Electroencephalographic Society. 1991 Apr;
[PubMed PMID: 2050819]
[21]
Sininger YS, Auditory brain stem response for objective measures of hearing. Ear and hearing. 1993 Feb;
[PubMed PMID: 8444334]
[22]
Coats AC,Martin JL, Human auditory nerve action potentials and brain stem evoked responses: effects of audiogram shape and lesion location. Otolaryngology. 1978 Jan-Feb;
[PubMed PMID: 114907]
[23]
Pantev C,Lagidze S,Pantev M,Kevanishvili Z, Frequency-specific contributions to the auditory brain stem response derived by means of pure-tone masking. Audiology : official organ of the International Society of Audiology. 1985;
[PubMed PMID: 4051877]
[24]
Chertoff M,Lichtenhan J,Willis M, Click- and chirp-evoked human compound action potentials. The Journal of the Acoustical Society of America. 2010 May;
[PubMed PMID: 21117748]
[25]
Dau T,Wegner O,Mellert V,Kollmeier B, Auditory brainstem responses with optimized chirp signals compensating basilar-membrane dispersion. The Journal of the Acoustical Society of America. 2000 Mar;
[PubMed PMID: 10738807]
[26]
Wegner O,Dau T, Frequency specificity of chirp-evoked auditory brainstem responses. The Journal of the Acoustical Society of America. 2002 Mar;
[PubMed PMID: 11931309]
[27]
Elberling C,Don M, Auditory brainstem responses to a chirp stimulus designed from derived-band latencies in normal-hearing subjects. The Journal of the Acoustical Society of America. 2008 Nov;
[PubMed PMID: 19045789]
[28]
Suzuki J,Kodera K,Kaga K, Auditory evoked brainstem response assessment in otolaryngology. Annals of the New York Academy of Sciences. 1982;
[PubMed PMID: 6953884]
[29]
Kodera K,Yamane H,Yamada O,Suzuki JI, Brain stem response audiometry at speech frequencies. Audiology : official organ of the International Society of Audiology. 1977 Nov-Dec;
[PubMed PMID: 921605]
[30]
Legatt AD,Arezzo JC,Vaughan HG Jr, The anatomic and physiologic bases of brain stem auditory evoked potentials. Neurologic clinics. 1988 Nov;
[PubMed PMID: 3070334]
[32]
Melcher JR,Guinan JJ Jr,Knudson IM,Kiang NY, Generators of the brainstem auditory evoked potential in cat. II. Correlating lesion sites with waveform changes. Hearing research. 1996 Apr;
[PubMed PMID: 8735067]
[33]
Melcher JR,Kiang NY, Generators of the brainstem auditory evoked potential in cat. III: Identified cell populations. Hearing research. 1996 Apr;
[PubMed PMID: 8735068]
[34]
Buchwald JS,Huang C, Far-field acoustic response: origins in the cat. Science (New York, N.Y.). 1975 Aug 1;
[PubMed PMID: 1145206]
[35]
Caird DM,Klinke R, The effect of inferior colliculus lesions on auditory evoked potentials. Electroencephalography and clinical neurophysiology. 1987 May;
[PubMed PMID: 2436886]
[36]
Barrs DM,Brackmann DE,Olson JE,House WF, Changing concepts of acoustic neuroma diagnosis. Archives of otolaryngology (Chicago, Ill. : 1960). 1985 Jan;
[PubMed PMID: 3966892]
[37]
Zappia JJ,O'Connor CA,Wiet RJ,Dinces EA, Rethinking the use of auditory brainstem response in acoustic neuroma screening. The Laryngoscope. 1997 Oct;
[PubMed PMID: 9331319]
[38]
El-Kashlan HK,Eisenmann D,Kileny PR, Auditory brain stem response in small acoustic neuromas. Ear and hearing. 2000 Jun;
[PubMed PMID: 10890735]
[39]
Legatt AD, Electrophysiology of Cranial Nerve Testing: Auditory Nerve. Journal of clinical neurophysiology : official publication of the American Electroencephalographic Society. 2018 Jan;
[PubMed PMID: 29298210]
[40]
Jevtovic-Todorovic V,Brambrick A, General Anesthesia and Young Brain: What is New? Journal of neurosurgical anesthesiology. 2018 Jul;
[PubMed PMID: 28622158]
[41]
Wilder RT,Flick RP,Sprung J,Katusic SK,Barbaresi WJ,Mickelson C,Gleich SJ,Schroeder DR,Weaver AL,Warner DO, Early exposure to anesthesia and learning disabilities in a population-based birth cohort. Anesthesiology. 2009 Apr;
[PubMed PMID: 19293700]
[42]
Cullington HE,Bele D,Brinton JC,Cooper S,Daft M,Harding J,Hatton N,Humphries J,Lutman ME,Maddocks J,Maggs J,Millward K,O'Donoghue G,Patel S,Rajput K,Salmon V,Sear T,Speers A,Wheeler A,Wilson K, United Kingdom national paediatric bilateral project: Demographics and results of localization and speech perception testing. Cochlear implants international. 2017 Jan;
[PubMed PMID: 28010679]
[43]
Harrison RV,Gordon KA,Mount RJ, Is there a critical period for cochlear implantation in congenitally deaf children? Analyses of hearing and speech perception performance after implantation. Developmental psychobiology. 2005 Apr;
[PubMed PMID: 15772969]
[44]
Ching TY,Day J,Van Buynder P,Hou S,Zhang V,Seeto M,Burns L,Flynn C, Language and speech perception of young children with bimodal fitting or bilateral cochlear implants. Cochlear implants international. 2014 May;
[PubMed PMID: 24869442]
[45]
Matthies C,Samii M, Management of vestibular schwannomas (acoustic neuromas): the value of neurophysiology for intraoperative monitoring of auditory function in 200 cases. Neurosurgery. 1997 Mar;
[PubMed PMID: 9055284]
Level 3 (low-level) evidence
[46]
Voordecker P,Brunko E,de Beyl Z, Selective unilateral absence or attenuation of wave V of brain-stem auditory evoked potentials with intrinsic brain-stem lesions. Archives of neurology. 1988 Nov;
[PubMed PMID: 3190507]