Continuing Education Activity
Ocular hypotony can arise from several causes, including trauma, surgery, intraocular inflammation, and the use of systemic and topical medications. It can result in severe vision loss, especially if complicated by hypotony maculopathy or hypotony keratopathy. However, treatment, which can be medical or surgical, can be rewarding and result in the reversal of hypotony and return of vision. This activity reviews the evaluation and treatment of ocular hypotony and highlights the role of the interprofessional team in evaluating and treating patients with this condition.
Objectives:
- Describe the pathophysiology of ocular hypotony.
- Summarize the clinical features and evaluation of ocular hypotony.
- Review the complications of ocular hypotony.
- Explain the management of ocular hypotony.
Introduction
Ocular hypotony is a potentially vision-threatening condition.[1] It can be acute or chronic. Though controversy exists regarding the cut-off intraocular pressure (IOP) for the definition of hypotony, it is generally considered as an average IOP of 5 mm Hg or less measured at least three times.[2] Hypotony has also been defined as an IOP less than 6.5mmHg.[3]
Ocular hypotony can be clinical or non-clinical, depending on the occurrence of clinical features. It is not clear who will develop clinical signs of hypotony, and some patients can tolerate long periods of hypotony without loss of vision. Yet others develop features of keratopathy, maculopathy, and even choroidal effusion. Management depends on the identification and treatment of the cause. With timely diagnosis and prompt management, an excellent final visual outcome is possible in most cases with ocular hypotony.
Etiology
In general, ocular hypotony occurs following multiple causes, including a leak of intraocular fluid through ocular surgical wounds, reduction in aqueous humor production, use of some topical or systemic medications, and proliferative vitreoretinopathy (PVR). Hypotony occurs due to loss of aqueous humor which can be external following surgery and trauma or internal in cyclodialysis cleft or rhegmatogenous retinal detachment.[4]
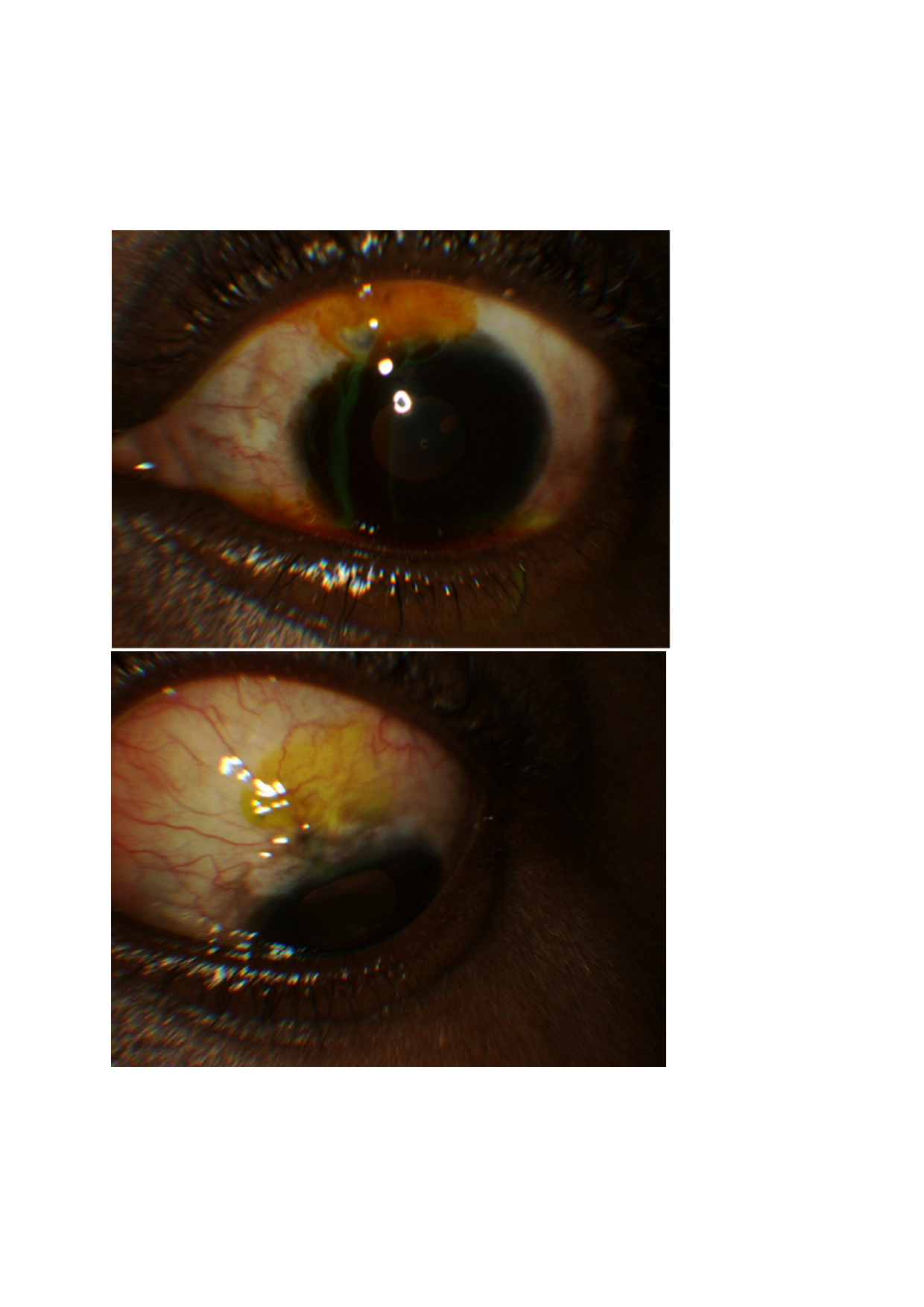
The most common clinical scenario for ocular hypotony is after filtration surgery for glaucoma (trabeculectomy), especially following the use of adjuvant antimetabolites such as mitomycin C (MMC) or 5 fluorouracil (5FU) to prevent postoperative fibrosis.[5] Figure 1 is a photograph of an eye showing leakage of aqueous from the anterior chamber through an atrophic cystic bleb several years after a trabeculectomy. There is a positive Seidel test in the upper frame of the photograph. The lower frame of the picture shows cessation of aqueous leakage and a negative Seidel test after revision of the filtering bleb. Other causes of ocular hypotony include intraocular inflammation, trauma, and other forms of ocular surgery such as vitreoretinal surgery.[3][4]
A good understanding of aqueous humor dynamics is essential to determine the etiology of ocular hypotony.[6][7] Aqueous humor is produced by the non-pigmented cells of the ciliary epithelium of the ciliary processes and is responsible for the maintenance of the intraocular pressure. Most of the aqueous humor, about 80%, is actively secreted by the ciliary processes, while the remaining is passively produced by ultrafiltration and diffusion.[8]
Normally the aqueous humor is secreted into the posterior chamber from where it passes through the pupil into the anterior chamber and baths the avascular structures, i.e., crystalline lens and cornea, acting as a surrogate for blood by providing much-needed oxygen and nutrients and removing the waste. Aqueous exits from the anterior chamber through the trabecular meshwork and the uveoscleral pathway. Therefore, causes of ocular hypotony can be broadly categorized into two, as indicated below. In addition, some systemic medications can result in ocular hypotony.
Decreased Aqueous Humor Production
- Intraocular inflammation
- Hypoperfusion
- Drug-induced (use of topical or systemic aqueous humor suppressants)
- Reduced ciliary body perfusion (ocular ischemic syndrome)
- Scarring or traction to the ciliary body, e.g., following trauma, proliferative vitreoretinopathy (PVR), chronic uveitis
- Cyclodestructive procedure
Increased Aqueous Humor Drainage
- Glaucoma filtering surgery
- Glaucoma drainage devices
- Angle-based surgery
- Iatrogenic creation of cyclodialysis cleft.
- Post-traumatic open globe injury
- Sequestration into intraocular spaces, such as in rhegmatogenous retinal detachment and cyclodialysis cleft
- Other surgeries, e.g., vitreoretinal surgery; corneal surgery (including full-thickness cornea transplant, corneal tear repair, and keratoprosthesis), scleral-fixated intraocular lens
Systemic Medications
- Carbonic anhydrase inhibitors acetazolamide and methazolamide
- Antihypertensive drugs, e.g., clonidine, beta-blockers
- Nitrates
- Antivirals like Cidofovir
- Hyperosmotic agents, e.g., mannitol
Systemic Causes
- Pregnancy
- Dehydration
- Uremia
- Diabetic coma
- Congenital weakness of the sclera, e.g., Marfan syndrome
- Other hereditary diseases, e.g., Myotonic dystrophy
More than one mechanism may account for the ocular hypotony in some cases. For instance, after glaucoma filtering surgery, hypotony may be because of over filtration of the surgical bleb or leakage from the bleb or elsewhere in the surgical wound. Hypotony after glaucoma surgery could also be due to mitomycin toxicity to the ciliary body.[9]
Careful examination is required to determine the exact mechanism of the postoperative hypotony as the management of each of these causes differs considerably. In the same light, after trauma, hypotony could arise from any of the following, open globe injury, cyclodialysis, ciliary body detachment, retinal detachment, and iridocyclitis. Rahman et al. have categorized the causes of post-glaucoma filtering surgery ocular hypotony based on postoperative timing as a. early and b. chronic. The causes of early postoperative hypotony after glaucoma surgery include the following:[10]
- Over-filtration
- Wound leak
- Reduced aqueous production
- Ciliochoroidal detachment
- Retinal detachment
- Globe perforation
- Iridocyclitis
Multiple causes can lead to chronic postoperative hypotony, including the following:
- Leaks in the conjunctiva
- Over-functioning bleb (excessive filtration)
- Avascular thin cystic bleb
- Cyclodialysis cleft
- Ciliary body detachment
- Retinal detachment
- Ciliary body atrophy
- Cyclitic membrane
Lastly, some systemic conditions can be associated with bilateral ocular hypotony, including dehydration, uremia, diabetic coma, myotonic dystrophy, and pregnancy. Systemically administered medications, as listed above, can be associated with ocular hypotony.
Epidemiology
The frequency of ocular hypotony in the general population is not known. The risk factors of ocular hypotony include surgery, trauma, and intraocular inflammation. Therefore, the frequency of ocular hypotony has been reported in these at-risk situations. Higashide et al. reported the five-year probability of ocular hypotony in a large series (955 eyes) that had glaucoma filtering surgery with mitomycin C to be 7.7 +/- 0.9 %.[11] Zacharia reported ocular hypotony in about one-third of eyes that had trabeculectomy with mitomycin C.[5]
Bohm et al. reported ocular hypotony in 15.6% of juvenile uveitis patients.[12] Ding et al. observed ocular hypotony in 6.9% of 145 eyes with blunt ocular trauma. Also, Ding reported that ocular hypotony was significantly higher amongst eyes with ciliochoroidal detachment, traumatic retinal detachment, and anterior proliferative vitreoretinopathy. The incidence of ocular hypotony after trans-scleral laser cycloablation has also been reported to be 10% in 70 eyes that received trans-scleral cyclophotocoagulation for glaucoma.[13]
A review on hypotony maculopathy put the incidence of this complication after glaucoma filtering surgery with antimetabolite use at 20%.[14]
Pathophysiology
Ocular hypotony is often encountered because of the excessive drainage of aqueous humor from the eye, which could occur following glaucoma filtering surgery or perforating globe injury. Less frequently, ocular hypotony can result from reduced aqueous humor production, secondary to intraocular inflammation. Following a decrease in the volume of circulating aqueous, the anterior-posterior axial length of the eyeball decreases with an accompanying inward displacement of the scleral wall. This creates redundancy in the choroid and retina, which manifests as choroidal-retinal folds that can be observed clinically as macular striae, retinal pigment epithelium changes, and retinal vascular tortuosity. With a decrease in the anteroposterior diameter of the vitreous cavity, the thick perifoveal retina is thrown into radial folds around the fovea.[14]
The clinical entity described is known as hypotony maculopathy. Hypotony maculopathy occurs in up to 20% of cases after glaucoma filtering surgery. The occurrence of this complication has become more common after introducing antimetabolites.[15] Also, similar Descemet membrane folds and cornea edema may be seen on the cornea as evidence of hypotony keratopathy.[16] Hypotony keratopathy is thought to be related to endothelial dysfunction secondary to hypotony.[17]
Other effects of ocular hypotony include a hyperopic shift in refraction due to a reduction in axial length. Because of the anterior bowing of the lamina cribrosa, there is restricted axoplasmic flow, which results in optic disc swelling. The edges of the Bruch membrane and the openings in the lamina cribrosa are thought to constrict axon bundles in ocular hypotony. Also, the finding of optic disc swelling has been associated with posterior globe flattening.[18]
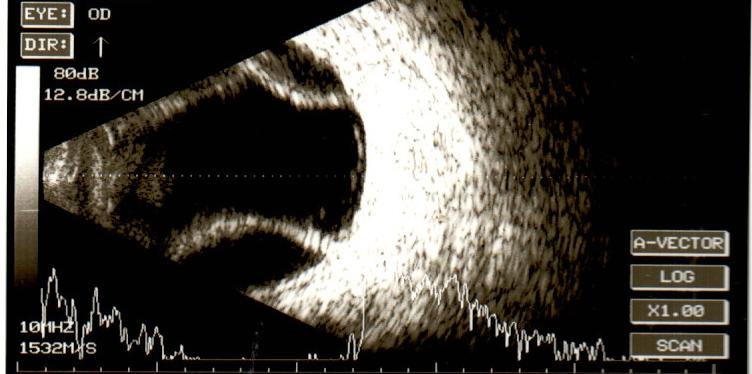
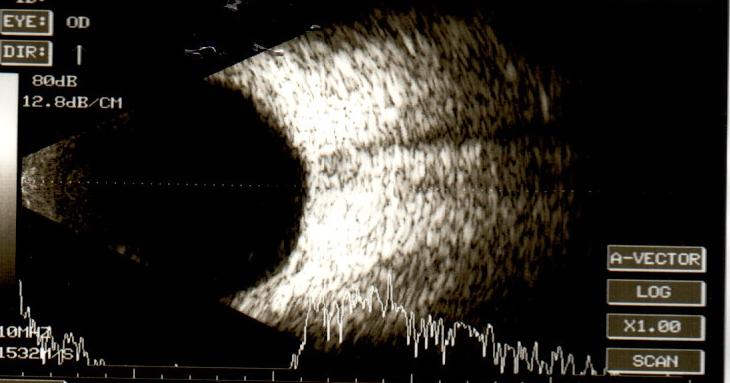
Other common posterior segment associations of ocular hypotony after glaucoma surgeries include choroidal detachment and ocular decompression retinopathy.[19] Rupture of choroidal vessels may create a hemorrhagic component to the serous fluid resulting in a hemorrhagic choroidal detachment. Figure 2 shows a post-operative choroidal detachment on the B scan of a patient's right eye after glaucoma filtering surgery resulted in ocular hypotony. Figure 3, a repeat B scan after normalization of the IOP weeks later, shows a complete resolution of the choroidal detachment and a normal-appearing posterior segment.
Histopathology
The histological findings of the conjunctiva and sclera following mitomycin C application have been studied using light microscopy. They have shown hypocellularity of the fibroblasts and distortion of the typical architecture. Post trabeculectomy with mitomycin C, documented electron microscopic findings include the presence of myelin figures and increased melanolipofuscin granules.[20]
Also present are vacuolated cytoplasm and disrupted mitochondria of the ciliary body epithelium. As a result of these findings, it has been suggested that over filtration and aqueous hyposecretion are the mechanisms of the post-operative chronic hypotony occurring after using mitomycin C for trabeculectomy.[10]
Furthermore, histological examination of mitomycin C treated trabeculectomy eyes revealed the presence of patent sclerotomies with hypocellular formed bleb cavities. The findings confirm the inhibitory effects of mitomycin-C on fibrovascular, fibrocellular, and collagen cells.
History and Physical
The clinical presentation of ocular hypotony depends on the etiology. Aside from the history of presenting symptoms, it is essential to investigate for a history of ocular trauma or surgery and other ocular conditions such as uveitis and retinal detachment that are known causes of hypotony. Systemic diseases associated with ocular hypotony should be determined, such as pregnancy, uremia, diabetes, and myotonic dystrophy.
The attending clinician should search for vascular causes of decreased blood flow to the ciliary body, such as ocular ischemic syndrome. It is not unusual for the patient's ocular hypotony to be drug-induced. Therefore, the use of any topical and systemic medications that can cause ocular hypotony should be explored.
A history of vision loss or distortion in images may suggest a significant effect of ocular hypotony on the eye. However, in several cases, the patient is asymptomatic and will have reasonably good vision with an IOP of 5 mm Hg or less. Clinical ocular hypotony may be consequential to any previously listed ocular sequelae of hypotony, including hypotony maculopathy, keratopathy, optic disc swelling, and even refractive error changes. In some cases of ocular hypotony, rapid progression of cataract occurs.
On clinical examination, the visual acuity may be reduced or normal. The measured intraocular pressure is significantly reduced to 5 mm Hg or less. There may be a demonstrable compromise to the globe integrity, such as leakage from a bleb, perforation of the globe, or corneal laceration. In all cases of aqueous humor leakage from the eye, a Seidel test utilizing fluorescein dye should be used to demonstrate the leakage.[21][22]
The Seidel test assesses the occurrence of aqueous humor leakage through a defect in the integrity of the cornea or sclera from the anterior chamber, as shown in Figure 1. The defect in the cornea or sclera could be from several causes, including trauma, post-surgical leak, and corneal perforation.[23] Fluorescein dye is applied to the ocular surface, making the egress of aqueous humor visible when observed with the cobalt blue light of the slit lamp biomicroscope.
Furthermore, examination using the slit lamp biomicroscope could reveal the presence of corneal striae and corneal edema. This finding may be associated with a shallow anterior chamber. There may be trembling (donesis) of the intraocular lens (pseudophacodonesis) or the crystalline lens (phacodonesis), or iris (iridodonesis) during ocular movements. Signs of intraocular inflammation may be evident such as keratic precipitates and fibrin in the anterior chamber. Cyclic membranes and synechiae may also be observed.
In some cases of ocular hypotony, there is the formation of cataracts consequent to decreased nourishment from reduced circulating aqueous supply to the crystalline lens. Though tasking to perform in a hypotonic eye, Gonioscopy could reveal a cyclodialysis or other anterior chamber angle trauma signs.
Fundus examination could indicate the presence of ciliochoroidal detachment, which arises from transudation from the choroidal vessels in the suprachoroidal space. Rupture of these vessels may create a hemorrhagic component to the serous fluid. Other posterior segment findings include tortuosity of the blood vessels, optic disc edema, choroidal folds, and macula striae characteristic of hypotony maculopathy.
Retinal pigment epithelial changes in the macula can also be seen. Lastly, posterior segment examination may also reveal causes of ocular hypotony such as rhegmatogenous retinal detachment, advanced stages of proliferative vitreoretinopathy (PVR), and features of significant ocular ischemia.
Evaluation
Ocular hypotony is primarily a clinical diagnosis. In all cases of hypotony, an open wound or leak should be ruled out. Seidel test is beneficial in this regard. Other diagnostic procedures help outline ocular anatomy when evaluating a case of ocular hypotony and provide information on the etiology and presence of severe ocular hypotony.[3]
An instance of this is the use of ultrasound biomicroscopy (UBM). UBM uses an ultrasonic probe of 35 MHz or 50 MHz. The 35 MHz probes are used to evaluate the ciliary body as they can visualize deeper structures compared to the 50 MHz one. UBM helps assess the anterior chamber depth, image a shallow or flat anterior chamber, and the forward bowing of the iris seen in a situation of hypotony. The UBM can also image the ciliary body and reveal clinically missed cyclodialysis, atrophy, membrane over the ciliary body, detachment of the ciliary body, and intraocular foreign body.[24][25]
The choroidal effusion present in some cases of severe ocular hypotony can be imaged with a B (brightness) mode ultrasound scan. The B scan can also show the presence of a choroidal or retinal detachment when the fundal view is not entirely clear.
A choroidal detachment in a postoperative hypotonic eye can be seen in the B scan in figure 2. Similarly, for the imaging and evaluation of retinal and choroidal folds, fundus fluorescein angiography (FFA), optical coherence tomography, and optical coherence tomography angiography can be utilized.[26]
On FFA, choroidal folds appear as alternating hyper fluorescence and hypo fluorescence bands. Hyperfluorescent crests appear due to atrophy of the RPE, while the troughs are hypo fluorescent. Disc swelling associated with hypotony could demonstrate features of leakage on FFA. Spectral-domain OCT is more sensitive than fundus photographs in diagnosing hypotony maculopathy and can detect folds in the presence of normal eye examination.[27]
Indocyanine Green Angiography (ICG) can also be used to image choroidal folds in situations of ocular hypotony and could detect folds missed by FFA.[28]
Treatment / Management
The treatment of ocular hypotony can be medical or surgical. Management of ocular hypotony depends on the cause, as outlined above. A good history and physical examination will usually reveal the cause and direct the treatment. The treatment could be relatively straightforward, such as discontinuing a specific culprit medication, surgical repair of a leaking globe injury, or more complicated with uncertain outcomes such as revising a bleb (demonstrated in figure 1) or repairing a large cyclodialysis cleft.
The goals of treating ocular hypotony depend on the cause and clinical impact of ocular hypotony. They include reversing the causative pathology, maintaining the anatomical integrity of the eye, and restoring any compromised visual function.[3] With this in mind, these principles can be applied to a clinician's diverse clinical scenarios.
Medical/Conservative Treatment
Ocular hypotony is commonly observed after filtering surgery and may result from a leaking bleb or over filtration. A large diameter (14 mm) bandage contact lens encourages epithelial migration and wound healing; this effectively manages early bleb leaks.[29][30]
Other options for managing a leaking bleb include cyanoacrylate glue, autologous blood injection, and compression sutures.[31] Cyanoacrylate glue is applied to the defective edge of the leaking conjunctival tissue but not into the bleb.
Uveitis-induced ocular hypotony is reported to occur after noninfectious and infectious uveitis.[32] The risk of ocular hypotony is higher after anterior uveitis and panuveitis. A diversity of mechanisms can be responsible for uveitis-induced ocular hypotony. This includes but is not limited to the following: acute ciliary shutdown leading to decreased aqueous production, ciliary body detachment (which can be induced by tractional membranes or serous ciliochoroidal effusion), atrophy of the ciliary processes, and in some cases, increased uveoscleral outflow. To manage the uveitis-induced acute ocular hypotony, aggressive, timely treatment of the active inflammation is essential to restore vision and prevent ocular complications.
Options for treatment include systemic corticosteroids, systemic nonsteroidal anti-inflammatory drugs, a topical steroid (including prednisolone acetate, difluprednate) and non-steroid, and local injection of steroids (including posterior subtenon triamcinolone, peribulbar/transseptal triamcinolone/methylprednisolone). In some cases, systemic immunomodulatory agents could be used to manage the primary inflammatory condition. Corticosteroid therapy can be used with good effect if the cause of hypotony is associated with intraocular inflammation and shuts down the production of aqueous by the ciliary processes.[32]
Corticosteroids also work by inducing a change in the extracellular matrix of the trabecular meshwork. Cycloplegic agents (including atropine) help treat ocular hypotony and provide posterior rotation of the ciliary processes, maintaining the anterior chamber depth. Topical ibopamine 2% has been used twice daily, with reports of good effect in treating patients suffering from chronic ocular hypotony attributable to vitreoretinal surgery, uveitis, and penetrating trauma.[33]
Injection of an ophthalmic viscosurgical device (OVD) has been used to treat ocular hypotony.[34] Intracameral injections of OVDs are often employed postoperatively to treat or prevent flat anterior chambers. Severe intraocular pressure rise has been documented as a complication of this procedure.[34]
Other reported complications of intracameral OVD injection include the need for severe inflammation, repeated OVD injections, and Descemet membrane detachment. It is recommended that OVDs with greater cohesiveness and viscosity be used for this purpose as they have better anterior chamber stabilization.
Cidofovir is an example of a systemic medication that can induce ocular hypotony and anterior uveitis.[35] Cidofovir is used for treating Cytomegalovirus retinitis in immunocompromised patients, including AIDS (acquired immunodeficiency syndrome).[36]
It is usually used as an intravenous infusion; however, topical and intravitreal preparations have also been used.[37] The use of cidofovir can result in ocular hypotony and severe uveitis with hypopyon simulating endophthalmitis. Therefore, cidofovir therapy necessitates slit-lamp surveillance, especially in patients on HAART (highly active antiretroviral therapy). Cidofovir-related uveitis requires a local steroid treatment. In situations of clinical hypotony, cidofovir should be withdrawn. In one report on intravenous cidofovir, a significant number of patients developed anterior uveitis.[36]
The cellular anterior chamber activity resolved with topical corticosteroid administration in all eyes with uveitis, but some patients had a significant flare that persisted despite topical steroids. Posterior synechiae responded poorly to topical mydriatic therapy—visually significant hypotony maculopathy developed in a minority of patients.
The same authors advised that cidofovir should be discontinued in favor of an alternative anti-cytomegaloviral agent when ocular hypotony occurs. In another report, two patients developed severe cidofovir-related hypotony, necessitating discontinuation of therapy. They were treated successfully with Ibopamine 2% eye drops combined with dexamethasone 0.1% eyedrops.[38]
Surgical Treatment
In general, the surgical treatment of ocular hypotony is instituted when the conservative approach has not been successful, apart from cases that require immediate surgery, such as the repair of a globe perforation or retinal detachment. The excision and revision of a leaking bleb may be required using either the conjunctival advancement approach or a free conjunctival autograft.[39]
Ab Interno partial tube ligation has been used as an effective surgical option to achieve an immediate, predictable, and sustained intraocular pressure increase either as a primary procedure or after the failure of conventional methods to resolve hypotony in eyes with non-valved glaucoma drainage devices (GDDs).[40]
Prompt resolution of the hypotony often results in normalization of retinal anatomy. Other surgical treatments for ocular hypotony include the repair of a retinal detachment and cyclodialysis cleft.
Traction-induced ciliary body detachment is a cause of ocular hypotony, and it is associated with proliferative vitreoretinopathy, uveitis, and trauma. The use of silicone oil in vitreoretinal surgery for PVR or recurrent retinal detachments and chronic uveitis has improved ocular hypotony.[41] The excision of portions of the anterior retinal flap following a broad retinectomy is protective against PVR-induced postoperative hypotony.[42] The foldable capsular vitreous body was developed in China to treat severe retinal detachments and after severe ocular trauma to prevent phthisis.
The dissection of membranes from the ciliary body (through direct visualization or endoscopic viewing) also promotes recovery of the ciliary body and therefore improves aqueous production. Gürelik et al. have reported a simple technique for treating ocular hypotension post glaucoma filtering surgery and vitreoretinal surgery.[43]
This surgical technique increases the resistance to aqueous outflow by placing a capsular tension ring (CTR) in the iridocorneal angle through a cornea incision. They treated 13 eyes that suffered from chronic severe hypotony using this technique, with a follow-up of at least one year, and reported an improvement in all treated eyes. This surgical technique is remarkable considering the ease with which the surgery can be performed, and the authors reported no surgical complications.
Ocular Ischemic Syndrome (OIS) is associated with ocular hypoperfusion and hypotrophy of the ciliary body. This eventually results in decreased aqueous production and chronic hypotony. The primary cause of OIS is atherosclerosis. But it could be due to giant cell arteritis, carotid artery disease, Behçet disease, trauma, and inflammation. Management of OIS is by a multidisciplinary team consisting of a cardiologist, neurologist, and ophthalmologist. The goal is to improve or restore ocular blood perfusion.
In line with the treatment goals, complications of ocular hypotony can be successfully treated using surgical techniques. A good example is the report of successful treatment of hypotony maculopathy using vitrectomy for non-resolving chorioretinal folds.[44] Also, peeling of the internal limiting membrane has been shown to release the subclinical traction from proliferating fibrocellular membranes. Perfluorocarbon liquid has also been used to treat chorioretinal folds.[44]
Before removing silicone oil, possible persistent postoperative hypotony or phthisis should be considered, especially in eyes with an IOP of 10 mm Hg or less in silicone oil-filled eyes.
Differential Diagnosis
Differential diagnosis of hypotony maculopathy and chorioretinal fold includes:
- Tumors (choroidal melanomas and metastasis)
- Inflammatory (posterior scleritis)
- Neovascularization (age-related macular degeneration)
- Retrobulbar mass (orbital tumor)
- Papilledema (associated with radiating chorioretinal folds).
Other causes of chorioretinal folds include retinal detachment, extraocular materials fixed to the sclera, scleral buckles, and radioactive plaques. Idiopathic chorioretinal folds may also be diagnosed after excluding all other possible causes of such folds. Hypotony keratopathy is characterized by folds in the Descemet membrane and cornea edema.
Examples of disorders in which cornea fold may be seen include keratoconus, post keratorefractive surgery, and Haab striae in primary congenital glaucoma. In some instances, ocular hypotony can be wrongfully diagnosed in the clinical scenario of a thinner than usual central cornea, such as in cases of high myopia.[45][46] Adjusting the intraocular pressure appropriately for the thinner than normal cornea could reveal a normal eye pressure.
Prognosis
In general, the prognosis of ocular hypotony depends on the impact of the hypotony on the eye and the etiology of the ocular hypotony. Hypotonic eyes are apt to undergo various changes that will affect the media's clarity, including the formation of cataracts and cornea opacity.[47] Changes in a refractive error such as hyperopic shift with a reduction in axial diameter and myopic shift with anterior displacement of the lens can have a significant impact on the vision.[48]
Astigmatism can occur from the effect of adjacent extraocular muscles and adnexa on the soft eyeball and non-resistant sclera. Posterior segment findings, including ciliochoroidal detachment and hypotonic maculopathy, can also profoundly impact vision.[49]
The etiology of the ocular hypotony can directly affect the visual prognosis, such as the direct effect of trauma, ocular ischemia, and advanced PVR. Also, the duration of the hypotony is another prognostic factor. Chronic hypotony may be associated with more permanent changes and may fall within the constellation of phthisis bulbi. However, several authors have shown a reversal of the effect of ocular hypotony after successful treatment, including bleb revision.[43][50][51]
Complications
Ocular hypotony can be transient with limited risk to the eye. But in some instances, it can evolve into a more chronic situation with significant and devastating effects on the eye and vision, such as evolution to phthisis bulbi.[52][53]
Often, the complications of hypotony may co-exist with the primary pathology responsible for the hypotony. For instance, in the setting of trauma, complications of ocular hypotony may be associated with other features of trauma, which may result in disorganization of the globe. In uveitis, anterior and posterior synechia, macular edema, and cataract may also co-exist with hypotony and its effects.[54]
Complications specific to ocular hypotony include hypotony maculopathy with characteristics described in the earlier sections on pathophysiology. Other complications include choroidal detachment, hypotony keratopathy, refractive change, papilledema, and cataract formation.[15][16][55]
Treatment of these complications of ocular hypotony can result in a favorable response with improvement in vision.
Deterrence and Patient Education
Since ocular hypotony can considerably harm the vision, surgeons, their support team, and the patient should take measures to avoid its occurrence following surgery. In glaucoma filtering surgery, surgeons should pay attention to the careful use of intraoperative antimetabolites.
Care should be taken to prevent antimetabolite contact with the conjunctival edges resulting in conjunctival thinning and bleb leaks. Placement of releasable sutures, which can be removed post-operatively, resulting in increased aqueous outflow, enabling titration of intraocular pressure, is an effective method to prevent early postoperative hypotony.[56][57]
Releasable sutures have also been useful in preventing wound leaks and hypotony after vitreoretinal surgery.[58] The initial reports of hypotony and wound leaks following small gauge transconjunctival vitreoretinal surgery have been overcome by a better understanding the problem and improved wound construction among surgeons.
A patient who suffers from postoperative hypotony from wound leak must understand the risk of infection from the leakage site and be prescribed topical antibiotics. Some antibiotics, such as topical aminoglycosides, induce conjunctival inflammation, stimulating wound healing and closure of the conjunctival defect. Furthermore, the patient should be given specific instructions to avoid direct physical trauma to the hypotonic eye. This can result in more damage to the eye, including globe rupture and intraocular hemorrhage. A protective eye shield is appropriate to cover the hypotonic eye during sleep.[59]
Enhancing Healthcare Team Outcomes
Ocular hypotony can be caused by a wide range of ocular and systemic conditions, and the diagnosis is often clinical. Ocular hypotony may also result as a complication of drug use. The diagnosis and management of ocular hypotony may involve diverse ophthalmic subspecialists, including glaucoma, vitreoretinal, uveitis, and cornea.[10][60]
The systemic causes of hypotony could involve an interplay between the ophthalmologist, cardiologist, neurologist, rheumatologist, and obstetrician. Opthalmology NPs and PAs may also be involved in the case. In some cases, the input of a pharmacist is required if some of the topical and systemic medications associated with intraocular pressure reduction are in use and are possible culprits.[61]
For diagnosing and evaluating the effect of treatment on the ocular complications of hypotony such as hypotony maculopathy, diverse ocular imaging investigations including fundus photography, fundus autofluorescence, fluorescein angiography, optical coherence tomography (OCT), and OCT Angiography, and more is required.[27][62][63][64]
These investigations require the services and expertise of an ophthalmic photographer and ophthalmic technician. The nurses play a crucial role in the management team by educating the patient and relations on using prescribed medications without dropper contact with the eye, maintaining strict hygiene, and preventing infection.
The prognosis and outcome of ocular hypotony depend on the cause. However, quick resolution of the hypotony is beneficial to good vision. Several causes of ocular hypotony will require immediate treatment, such as retinal detachment and ocular trauma. Therefore, urgent consultation with a multidisciplinary and interprofessional team is advised.