Indications
As of January 24, 2022, the United States Food and Drug Associated (FDA) fact-sheet for the drug bamlanivimab states that "due to the high frequency of the Omicron variant, bamlanivimab and etesevimab, administered together, are not currently authorized for use in any U.S. region because of markedly reduced activity against the Omicron variant. These drugs may not be administered for treatment or post-exposure prevention of COVID-19 under the Emergency Use Authorization until further notice by the Agency." This article is for historical purposes only to review the indications, mechanism, and administration of this therapy when it was first developed.
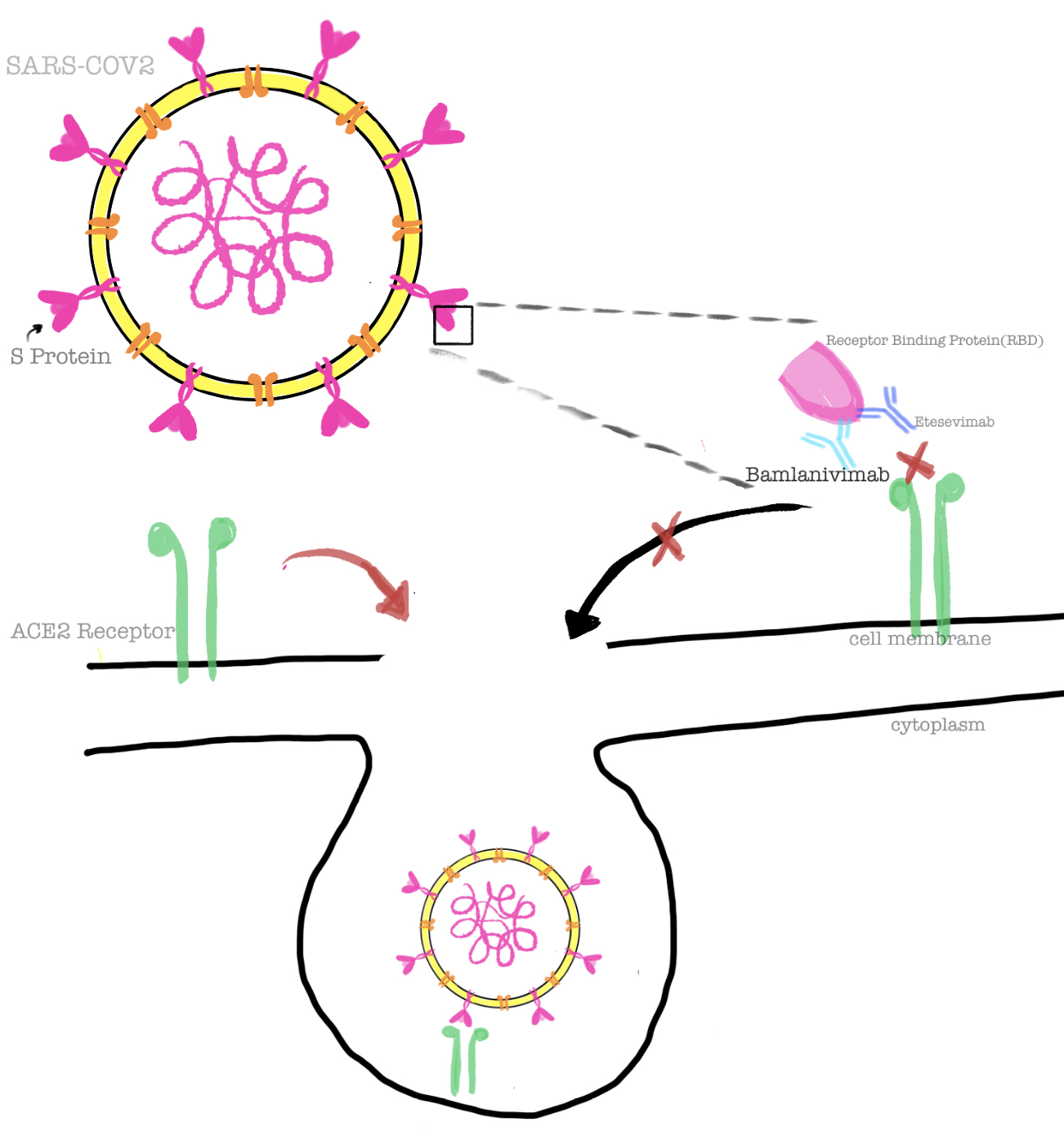
Bamlanivimab is a monoclonal antibody (mAb) directed against the spike protein (S-Protein) of severe acute respiratory syndrome-coronavirus-2 (SARS-CoV-2). Bamlanivimab, also known as LY-COV555, was derived from the convalescent plasma of coronavirus disease 2019 (COVID-19) patients.[1]
It is one of the potent neutralizing antibodies approved by the Food and Drug Administration (FDA) under Emergency Use Authorization (EUA) in August 2021 to be used in combination with etesivimab (another mAb against S-protein of SARS-CoV-2).[2] The other neutralizing antibodies available are casirivimab and imdevimab, which are used in combination therapy.[3][4][5] The other novel agent in this class is sotrovimab.[6]
The FDA has approved the administration of the combination drug as treatment and post-exposure prophylaxis in patients meeting the following criteria:
Treatment
- Mild to moderate COVID-19, at higher risk of progression to severe disease including hospitalization or death
- Patients with Direct SARS-CoV-2 Viral test positive results and within ten days of symptom onset
- Adults and pediatric population including neonates meeting above two criteria
Post-Exposure Prophylaxis
- Exposed to an individual infected with SARS-CoV-2 defined by close contact criteria as per Centers for Disease Control and Prevention (CDC) or at high risk for exposure in same institutional setting due to occurrence of SARS-CoV-2 in that setting, such as nursing home, prisons.
- At higher risk of progression to severe disease, including hospitalization or death
- Not fully vaccinated or not expected to have adequate response to complete vaccination. For example - patients with immunocompromising conditions, including those on immunosuppressive drugs.
- CDC describes close contact with an infected individual as being within 6 feet for at least 15 minutes, direct physical contact, droplet exposure, or providing care at home to an infected individual.
The following patient population qualifies as high-risk individuals:
- Age ≥ 65 years or <1 year
- Body mass index (BMI): Adults - BMI > 25 kg/m^2; age 12 to 17 years - BMI ≥ 85th percentile for age and sex
- Pregnancy
- Diabetes
- Cardiovascular disease including hypertension, congenital heart disease
- Lung disease - moderate to severe asthma, chronic obstructive pulmonary disease (COPD), Interstitial lung disease (ILD), cystic fibrosis, and pulmonary hypertension
- Chronic kidney disease
- Neurodevelopmental disorders
- Immunocompromised state including cancer, organ transplant, HIV, individuals on immunosuppressive treatment
- Sickle cell disease
- Dependence on medical-related technology, like tracheostomy, gastrostomy, or positive pressure ventilation unrelated to COVID-19[2]
Due to emerging variants, the FDA has authorized the combination drug to be used only in the states and territories where the data shows that resistance to the variants is < 5%. Health care providers are recommended to check the FDA website regularly for updates regarding this medication.