
Introduction
The scapula or shoulder blade is the bone that connects the clavicle to the humerus. The scapula forms the posterior of the shoulder girdle. It is a sturdy, flat, triangular bone. The scapula provides attachment to several groups of muscles. The intrinsic muscles of the scapula include the rotator cuff muscles, teres major, subscapularis, teres minor, and infraspinatus. These muscles attach the scapular surface and assist with abduction and external and internal rotation of the glenohumeral joint. The extrinsic muscles include the triceps, biceps, and deltoid. The third group of muscles includes the levator scapulae, trapezius, rhomboids, and serratus anterior. These muscles are responsible for rotational movements and stabilization of the scapula.
Structure and Function
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Structure and Function
The scapula is an important bone in the function of the shoulder joint. It engages in 6 types of motion, which allow for full-functional upper extremity movement including protraction, retraction, elevation, depression, upward rotation, and downward rotation. Protraction is accomplished by the actions of the serratus anterior, pectoralis major, and pectoralis minor muscles. Retraction is accomplished by the actions of the trapezius, rhomboids, and latissimus dorsi muscles. The elevation is accomplished by the trapezius, levator scapulae, and rhomboid muscles. Depression is accomplished through the force of gravity and the actions of the latissimus dorsi, serratus anterior, pectoralis major and minor, and the trapezius muscles. Upward rotation is accomplished by the trapezius and serratus anterior muscles. Downward rotation is accomplished by the force of gravity as well as the latissimus dorsi, levator scapulae, rhomboids, and the pectoralis major and minor muscles. Through these six motions, the scapula allows full function of the shoulder joint, one of the most mobile and versatile joints in the human body. One example of the importance of scapular motion for the full range of motion of the upper extremity is that of the winged scapula (See Clinical Significance), in which paralysis of the serratus anterior or trapezius prohibits the raising of the upper extremity above the level of the shoulder.
Embryology
The scapula begins osteogenic development via endochondral ossification in week 11 of human embryogenesis. This occurs shortly after week 10 of humerus development, during which it will form the glenohumeral joint.
Blood Supply and Lymphatics
The scapular blood supply is complex due to its position and role as a critical component of the shoulder joint and the necessity for adaptability. It is largely fed by an anastomosis between the axillary artery and subclavian artery known as the scapular anastomosis. Contributory arteries to this anastomosis are the dorsal scapular artery, the suprascapular artery, the deep scapular artery, the circumflex scapular branch of the subscapular artery, and the medial anastomoses with the intercostal arteries. The scapular anastomosis allows for collateral blood flow when lying supine and when using the shoulder in its multitude of positions.
The venous drainage of the scapula is largely accomplished by the axillary vein, the suprascapular veins, and numerous small and highly variable anastomotic tributaries.
The lymphatic drainage from the right scapula empties into the right lymphatic duct and into the thoracic duct from the left scapula. The lymph nodes associated with the scapula include the axillary and the supraclavicular lymph nodes.
Nerves
The nerves to the scapula include the dorsal scapular, upper and lower subscapular, and suprascapular nerves, which arise from the brachial plexus at the anterior ramus C5 root, the posterior cord, and the superior trunk respectively. See "Muscles" section below for more details regarding specific muscle innervations.
Muscles
The intrinsic muscles of the scapula attach directly to the surface of the bone. These muscles are the four members of the rotator cuff and act to stabilize the glenohumeral joint. These include:
Supraspinatus
- Function: Initiation of arm abduction (first 15 degrees), stabilize glenohumeral joint
- Origin: Supraspinous fossa
- Insertion: Top of the greater tubercle
- Innervation: Suprascapular nerve (C5, C6)
Infraspinatus
- Function: Lateral rotation of the arm, stabilize glenohumeral joint
- Origin: Infraspinous fossa
- Insertion: Greater tubercle of humerus, between the supraspinatus and teres minor insertion
- Innervation: Suprascapular nerve (C5, C6)
Teres minor
- Function: Lateral rotation of the arm, stabilize glenohumeral joint
- Origin: Lateral/axillary border and adjacent posterior aspect of the scapula
- Insertion: Inferior aspect of the greater tubercle on the humerus
- Innervation: Axillary nerve (C5, C6)
Subscapularis
- Function: Adduction and medial rotation of the arm, stabilize glenohumeral joint
- Origin: Subscapular fossa
- Insertion: Lesser tubercle of humerus
- Innervation: Subscapular nerves (C5, C6, C7)
The extrinsic muscles of the scapula attach to the processes of the scapula and affect motion at the glenohumeral joint: These include:
Biceps brachii
- Function: Resists dislocation of the shoulder, major flexor of the forearm, supination of the forearm
- Origin:
- Short head: coracoid process
- Long head: supraglenoid tubercle
- Insertion: Radial tuberosity and forearm fascia (as bicipital aponeurosis)
- Innervation: Musculocutaneous nerve (C5, C6)
Triceps brachii
- Function: Resists dislocation of the shoulder, major extensor of the forearm
- Origin:
- Lateral head: above the radial groove,
- Medial head: below the radial groove
- Long head: infraglenoid tubercle of scapula
- Insertion: Olecranon process of ulna and fascia of the forearm
- Innervation: Radial nerve (C6, C7, C8)
Deltoid
- Function:
- Anterior aspect is responsible for flexion and medial rotation of the arm
- Middle aspect is responsible for abduction of the arm (up to 90 degrees)
- The posterior aspect is responsible for extension and lateral rotation of the arm
- Origin: Lateral clavicle, acromion and scapular spine
- Insertion: Deltoid tuberosity
- Innervation: Axillary nerve (C5, C6)
Stabilizing muscles of the scapula include:
Trapezius
- Function:
- Upper fibers elevate the scapula and rotate it during abduction of the arm (90 to 180 degrees)
- Middle fibers retract the scapula
- Lower fibers pull the scapula inferiorly.
- Origin: Skull, nuchal ligament and the spinous processes of C7 to T12
- Insertion: clavicle, acromion and the scapular spine
- Innervation: Accessory nerve (Cranial nerve XI)
Levator scapulae
- Function: Elevates the scapula
- Origin: Transverse processes of the C1 to C4 vertebrae
- Insertion: Medial border of the scapula
- Innervation: C3, C4, and the Dorsal scapular nerve (C5)
Serratus anterior
- Function: fixes the scapula into the thoracic wall, and aids in rotation and abduction of the arm (90 to 180 degrees)
- Origin: Surface of the upper eight ribs at the side of the chest
- Insertion: Along the entire anterior length of the medial border of the scapula
- Innervation: Long thoracic nerve (C5, C6, C7)
Rhomboid major
- Function: Retracts and rotates the scapula
- Origin: Spinous processes of T2 to T5 vertebrae
- Insertion: Inferomedial border of the scapula
- Innervation: Dorsal scapular nerve (C5)
Rhomboid minor
- Function: Retracts and rotates the scapula
- Origin: Spinous processes of C7 to T1 vertebrae
- Insertion: Medial border of the scapula
- Innervation: Dorsal scapular nerve (C5)
Other muscles attached to the scapula include:
Latissmus dorsi
- Function: Extends, adducts and medially rotates the upper limb
- Origin: Spinous processes of T6 to T12, iliac crest, thoracolumbar fascia, the inferior three ribs, and the inferior angle of the scapula
- Insertion: Intertubercular sulcus of the humerus
- Innervation: Thoracodorsal nerve (C6, C7, C8)
Teres major
- Function: Adduction and medial rotation of the arm
- Origin: Posterior surface of the scapula at its inferior angle
- Insertion: Intertubercular groove on its medial aspect
- Innervation: Lower scapular nerve (C5, C6)
Pectoralis minor
- Function: Depression of the shoulder, protraction of the scapula
- Origin: Third, fourth, fifth ribs close to their respective costal cartilages
- Insertion: Coracoid process
- Innervation: Medial pectoral nerve (C8, T1)
Coracobrachialis
- Function: Flexion and adduction of the arm
- Origin: Coracoid process
- Insertion: Middle of the humerus, on its medial aspect
- Innervation: Musculocutaneous nerve (C5, C6, C7)
Omohyoid
- Function: Pulls hyoid bone down, active while talking and swallowing
- Origin: Superior border of scapula
- Insertion: Inferior edge of the hyoid
- Innervation: Ansa cervicalis (C1, C2, C3)
Physiologic Variants
Os acromiale - Unfused center of secondary ossification in the acromion that may cause pain and tenderness. It is thought to increase the risk of impingement and rotator cuff tears. Initial treatment can be conservative, but surgical excision of the unfused fragment is an option in refractory cases.[1]
Sprengel deformity - Congenital elevation of the scapula that leads to decreased functionality of the scapula and upper limb. Surgical reconstruction is the usual approach to correct the cosmetics and functionality of the scapula. This is a rare condition, but it is the most common variant of the scapula.[2]
Surgical Considerations
In cases of severe shoulder arthritis, malignancy, or other indications for total shoulder arthroplasty, the scapula becomes important. The glenoid fossa and labrum, which make up the scapular portion of the joint, must be replaced with an artificial component. Additionally, preoperative evaluation of glenoid version relative to the scapular axis and scapular inclination using radiologic methods, such as CT scanning, should be undertaken by the surgeon as to reduce operative complications and to ensure optimal prosthesis implantation.[3] Glenoid rim positioning has also been shown to be important in determining the amount of bone mass eligible to be used for anchor positioning in prosthetic insertion during arthroplasty.[4] During total shoulder arthroplasty, there is a significant risk to the axillary nerve during deltoid dissection. A study has shown a linear correlation between acromion-axillary nerve distance and upper arm length, thus allowing for a better prediction of the location of the axillary nerve.[5]
Clinical Significance
The scapula is a strong bone and protects the posterior upper chest. Scapular fractures are rare and indicate severe trauma. Winging of the scapula may occur after injury to the long thoracic or the spinal accessory nerves. The long thoracic nerve may be injured during axillary dissection, trauma, or a thoracotomy.[6] The spinal accessory nerve may be injured during a procedure or with trauma to the posterior neck. In the case of a winged scapula, a pertinent physical exam finding would be the scapula on the affected side protruding posteriorly when a posterior force is applied to the extended upper extremity, such as in pushing on a wall with an arm flexed to 90 degrees. The thoracodorsal nerve may also be iatrogenically injured when performing surgery on the breast or axilla as it courses close to the anterior surface of the scapula. A sign of injury to the thoracodorsal nerve is paralysis of the ipsilateral latissimus dorsi muscle, leading to an inability to actively depress the shoulder. Injury to the dorsal scapular nerve should be suspected if the scapula on one side of the body is located more lateral from the midline when compared with the contralateral side. This injury causes paralysis of the ipsilateral rhomboid muscles.[7]
In shoulder impingement syndrome, there may be an abnormal scapular function. Dysfunctional movements of the scapula can lead to dyskinesis and abnormal motion of the shoulder. In rare cases after a high thoracotomy, the scapula may become impinged between the ribs.[8] In such cases, the base of the scapula may need to be revised.
The scapula also provides an attachment point for the ligaments connecting the acromion to the clavicle and the coracoid process to the clavicle. These ligaments, the acromioclavicular and coracoclavicular ligaments, may become injured during a fall directly onto or with other traumatic impacts to the shoulder leading to a shoulder separation. This is a common injury with several grades of severity, depending on how badly the ligaments are injured.[9]
A case study was performed on a patient who presented with a triad of humeral fracture, scapular fracture, and traumatic anterior dislocation of the humerus. It is rare for these three injuries to occur together. The case report demonstrated that open reduction and internal fixation of the fracture before reducing the dislocation should be performed to reduce the risk of neurovascular compromise.[10]
Media
(Click Image to Enlarge)
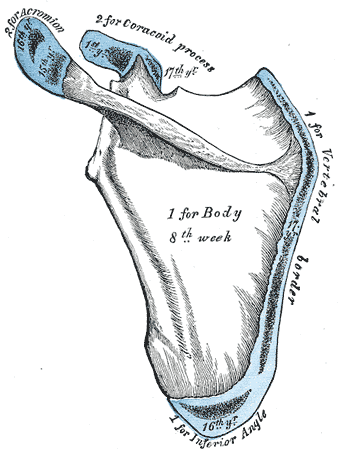
Scapula Anatomy. Anatomy includes scapula, plan of development, seven centres, vertebral border, acromion, and coracoid process.
Gray's Anatomy
References
Hurst SA, Gregory TM, Reilly P. Os acromiale: a review of its incidence, pathophysiology, and clinical management. EFORT open reviews. 2019 Aug:4(8):525-532. doi: 10.1302/2058-5241.4.180100. Epub 2019 Aug 9 [PubMed PMID: 31538003]
Pargas C, Santana A, Czoch WL, Rogers KJ, Mackenzie WG. Sprengel Deformity in Biological Sisters. Journal of the American Academy of Orthopaedic Surgeons. Global research & reviews. 2020 Apr:4(4):. doi: 10.5435/JAAOSGlobal-D-19-00120. Epub 2020 Apr 2 [PubMed PMID: 32377613]
Fulin P, Kysilko M, Pokorny D, Padr R, Kasprikova N, Landor I, Sosna A. Study of the variability of scapular inclination and the glenoid version - considerations for preoperative planning: clinical-radiological study. BMC musculoskeletal disorders. 2017 Jan 14:18(1):16. doi: 10.1186/s12891-016-1381-4. Epub 2017 Jan 14 [PubMed PMID: 28088244]
Wang S, Wang J, Gu C, Zuo J. [An anatomic study of glenoid regarding anchor insertion posion and direction]. Zhonghua wai ke za zhi [Chinese journal of surgery]. 2015 Feb:53(2):90-4 [PubMed PMID: 25908279]
Samart S, Apivatgaroon A, Lakchayapakorn K, Chemchujit B. The correlation between acromion-axillary nerve distance and upper arm length; a cadaveric study. Journal of the Medical Association of Thailand = Chotmaihet thangphaet. 2014 Aug:97 Suppl 8():S27-33 [PubMed PMID: 25518290]
Noland SS, Krauss EM, Felder JM, Mackinnon SE. Surgical and Clinical Decision Making in Isolated Long Thoracic Nerve Palsy. Hand (New York, N.Y.). 2018 Nov:13(6):689-694. doi: 10.1177/1558944717733306. Epub 2017 Oct 4 [PubMed PMID: 28975819]
Muir B. Dorsal scapular nerve neuropathy: a narrative review of the literature. The Journal of the Canadian Chiropractic Association. 2017 Aug:61(2):128-144 [PubMed PMID: 28928496]
Level 3 (low-level) evidenceZaidenberg EE, Rossi LA, Bongiovanni SL, Tanoira I, Maignon G, Ranalletta M. Snapping scapular syndrome secondary to rib intramedullary fixation device. International journal of surgery case reports. 2015:17():158-60. doi: 10.1016/j.ijscr.2015.11.010. Epub 2015 Nov 19 [PubMed PMID: 26629853]
Level 3 (low-level) evidenceBonz J, Tinloy B. Emergency department evaluation and treatment of the shoulder and humerus. Emergency medicine clinics of North America. 2015 May:33(2):297-310. doi: 10.1016/j.emc.2014.12.004. Epub 2015 Feb 26 [PubMed PMID: 25892723]
Mechanism of injury and management in traumatic anterior shoulder dislocation with concomitant humeral shaft and ipsilateral scapula fracture: a case report and review of the literature., Farooque K,Khatri K,Dev C,Sharma V,Gupta B,, Journal of medical case reports, 2014 Dec 16 [PubMed PMID: 25511744]
Level 3 (low-level) evidence