
Introduction
Syringomyelia, at its core, is a disorder characterized by abnormal cerebrospinal fluid (CSF) circulation, leading to the formation of fluid-filled cavities (syrinx) within the spinal cord parenchyma or central canal. A syrinx is a fluid-filled cavity anatomically within the spinal cord parenchyma or the central canal. This condition is often associated with Chiari malformation type 1 (CM-1) but can also result from various factors such as spinal cord tumors, trauma, or infectious adhesive arachnoiditis.[1][2]
Although syringomyelia predominantly presents with sensory symptoms such as pain and temperature insensitivity, it is an incidental finding in most cases.[3] The discovery of syringomyelia is more common because of the increased use of magnetic resonance imaging (MRI) in the routine evaluation of back and neck pain.[4]
The natural history of patients with syringomyelia is variable and unpredictable, with periods of stability and progression. Although professionals do not completely understand the natural history of syringomyelia, the clinical course typically progresses over months to years, with an early rapid deterioration that gradually slows down.[5] Sudden head jolting or prolonged bouts of coughing can trigger a sudden onset of symptoms in a previously asymptomatic patient, presumably because of an increase in tonsillar descent.[6][7] Notably, syringomyelia accounts for up to 5% of paraplegia.[8]
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
Syringomyelia develops due to a disturbance in CSF flow dynamics,[9] often resulting from spinal subarachnoid space obstruction in most cases.
Classification of Syringomyelia
Communicating: This is characterized by central canal dilatation that communicates with the fourth ventricle and is invariably associated with hydrocephalus. The cavity of the syrinx features an ependymal lining.
Non-communicating (isolated): This involves dilations of the central canal resulting from altered CSF flow dynamics within the spinal subarachnoid space resulting from CM-1, basilar impression, and arachnoiditis. These dilations tend to dissect paracentrally into the posterolateral quadrant of the spinal cord.
Extracanalicular: This is observed in the watershed area of the spinal cord following trauma or strokes and is characteristically associated with myelomalacia. These syrinx cavities are lined with glial or fibroglial tissue.[10][11]
Types of Syringomyelia or Hydromyelia
Non-communicating syringomyelia is the most common type of syringomyelia.
- Type I: This type of syringomyelia arises due to obstruction at the foramen magnum and subsequent dilation of the central spinal canal caused by conditions such as CM-1, basilar invagination, and other lesions.
- Type II: This type of syringomyelia occurs without any obstruction at the foramen magnum, and is often considered idiopathic.
- Type III: Syringomyelia results from lesions directly affecting the spinal cord, including tumors, traumatic myelopathy, spinal arachnoiditis, pachymeningitis, and myelomalacia.
- Type IV: Pure hydromyelia.[12]
Etiologies of Syringomyelia
- Cranio-cervical anomalies: These include CM-1 and basilar impression. CM-1 represents the most frequent cause,[9] with syringo-hydromyelia reported in 23% to 80% of CM-1 patients according to current literature.
- Other causes: These include tumors, trauma leading to dorsal arachnoidal webs, arachnoiditis, meningitis, postoperative scarring, and dysraphism.[13][14][15][16]
Intradural Pathologies Obstructing the CSF Flow
- Tonsils occupying the foramen magnum and overlying foramen of Magendie, medialized tonsils, tonsillar gliosis, and tonsillar hypertrophy
- Dural scarring
- Arachnoid veil, webs, adhesions, and thickening
- Vermian branch of the posterior inferior cerebellar artery
Epidemiology
The prevalence of CM-1 ranges from 3 to 8 per 100,000 individuals, with syringomyelia diagnosed in 65% of CM-1 patients.[9] The reported prevalence of syringomyelia in the literature ranges from 8.4 per 100,000 to 0.9 per 10,000.[14] A study in Italy reported a prevalence of 4.84 per 100,000 with an incidence of 0.82 per 100,000. Among Caucasians, the prevalence is reported as 5.4 per 100,000, while in Japan, it is 1.94 per 100,000.[12]
Approximately 22.7% of patients with syringomyelia are asymptomatic. In operative series from the United States and Europe, the peak ages of presentation for CM-1 were 8 in pediatric cases and 41 in adult cases. The incidence of syringomyelia in these studies was 65%.[19] With the rise in radiological imaging, incidentalomas are increasingly being detected.[20]
Pathophysiology
Authors have proposed various theories to explain the origin and progression of syringomyelia.
- Gardner and Angel introduced the "hydrodynamic theory," suggesting that hindbrain hernias obstruct normal CSF egress, causing fluid to divert into the central spinal canal and pulsate with each heartbeat, which is also known as the "water-hammer" effect.
- Williams observed pressure gradients exceeding 100 mm Hg across the foramen magnum during Valsalva maneuvers in patients with hindbrain hernias. He hypothesized that this pressure difference creates a suctional force ("suck") that draws ventricular CSF into the syrinx cavity. The fluid's entry impacts and rebounds ("sloshes") off the caudal and then rostral walls of the syrinx, akin to water behavior in an elastic balloon squeezed at one end. Although subsequent authors noted the lack of communication between the syrinx and the fourth ventricle, recent dynamic MRI studies have provided evidence supporting this theory. The slow caudal growth of a syrinx may be a result of approximately 42 million such impacts in a year.
- Ball and Dayan proposed that increased spinal CSF pressure, particularly during coughing or sneezing in patients with foramen magnum obstruction, drives CSF through para-vascular Virchow-Robin spaces along the spinal cord surface.
However, large-scale physiological studies have yet to confirm or refute these 3 proposals definitively.
- Oldfield et al proposed that a CSF pressure wave generated by the systolic "piston-like" caudal displacement contracts the cord, forcing fluid into the syrinx cavity from the spinal subarachnoid space. Critics argue that fluid cannot enter a contracted cord. Although dynamic MRI studies have shown downward tonsillar movement during systole, confirming trans-parenchymal CSF movement on Cine MRI remains elusive.
- Gretiz, Koyanagi, and Houkinkoya have proposed a theory supporting the extracellular nature of syrinx fluid rather than CSF. Abnormally rapid movement of CSF past the cord causes a low-pressure zone within the cord, promoting extracellular fluid build-up and syrinx formation.[3][21][22][23][24][25][26][27][28]
Although the pathophysiology concerning the origin of syringomyelia remains an elusive Gordian knot, the pathophysiology underpinning progressive syrinx enlargement may have a common theme.[29]
Development in the Pathogenesis of Syringomyelia
Classic communicating: Classic communicating theory posits that there is anatomical communication between the syrinx and the fourth ventricle.
Gardner and Angel postulated that atresia of the foramina of the fourth ventricle causes systolic “water hammer” from pulse wave, causing hydromyelia and herniating structures through the foramen magnum to act as a one-way pump and valve. This later ruptures the ependymal lining and diverticulum into the cord parenchyma, causing syrinx formation.[21]
In contrast, Williams argued against systolic pulse waves directly causing syringomyelia. He suggested that obstruction at the foramen magnum creates a craniospinal pressure dissociation, generating a "suck" effect. This disrupts normal CSF flow into the spinal subarachnoid space, redirecting it through the obex. The longitudinal intra-cavitary fluid motions, referred to as "slush," help in maintaining the syrinx.
Du Boulay supported the idea of 2 intracranial CSF pulse waves contributing to the systolic pulse wave in the absence of ventricular atresia. The ventricular pulse wave corresponds to the systolic pulse wave, whereas the cisternal pulse wave, the first pulse wave exiting the foramina of the fourth ventricle, also propagates into the spinal subarachnoid space.
Transmedullary infiltration: Subsequently, it was evident that anatomical communication between the syrinx and the fourth ventricle is rare.
Ball and Dayan observed that CSF pulse waves are typically insufficient to form a syrinx by entering an open central canal. They proposed that in cases of foramen magnum obstruction, a Valsalva-like maneuver leads to "craniospinal pressure dissociation," causing CSF to enter the spinal parenchyma via the perivascular space (Virchow-Robin spaces). Occasionally, the syrinx may rupture into the ependyma.[26]
However, Oldfield et al contested this theory by demonstrating compression of the upper part of the syrinx during systole. According to Oldfield, cerebellar tonsils acting as pistons generate pressure waves, forcing CSF into the parenchyma. This "Piston theory" gained support from subsequent work by Heiss.
Parenchymal formation: The pressure within the syrinx is observed to be equal to or higher than that in the spinal subarachnoid space, contradicting the transmedullary theory. Current understanding posits that the syrinx is a blood plasma "ultra-filtrate," a concept first proposed by Klekamp. The increased CSF flow resistance results in a disequilibrium between CSF and the intramedullary extracellular fluid exchange that typically occurs through the perivascular spaces.
Stoodley et al proposed that the volume and pressure of the cyst play crucial roles in regulating the balance between the inflow and outflow of CSF through the perivascular spaces.[30] Levine advocated for the concept of the spinal subarachnoid space and the neuroaxis venous system, which comprises two fluid columns in hydrostatic equilibrium. In cases of foramen magnum obstructions, the "transmural pressure displacement" leads to mechanical stress on the venous system, causing disruption to the blood-spinal cord barrier and resulting in leakage of an ultrafiltrate of blood, which contributes to syrinx formation.
Koyanagi and Houkin’s theory postulated that the reduced spinal subarachnoid compliance primarily impacts the posterior spinal veins, which lack a pial covering and are situated directly in the subarachnoid space. This disruption of Starling's equilibrium leads to intramedullary edema and eventual syrinx formation.[28]
Clinicopathological correlation: The primary pathology in syringomyelia involves a gradually enlarging cavity within the central spinal canal. This expanding CSF-filled "syrinx" compresses the spinothalamic tract neurons that cross in the anterior white commissure. However, the posterior columns remain unaffected due to their more distal location. Consequently, there is a loss of pain and temperature sensation with preserved touch and vibratory sense, leading to segmental dissociated sensory loss. This sensory loss predominantly affects the upper limbs in a "cape-like" distribution, with sensory deficits mainly observed in the shoulder area.
The natural history of CM-1 with syringomyelia is usually benign, as only a small fraction of patients treated non-surgically eventually require surgery.[20] Ependymal ciliary movement is regulated by Connexin 43 (Cx43) and actin. Studies using a rat model have demonstrated the loss of Cx43 at the site of compression, leading to the disarray of the actin network and exposing centrioles to CSF shear stress.
Basilar invagination, Chiari formation, and syringomyelia also result from atlantoaxial instability.[31] Cranio-cervical junction osseous anomalies and a skull base angle of >135° predict syrinx formation. The extent of tonsillar herniation was a determinant of cervical syrinx formation.[32]
Syringomyelia is associated with bony-posterior fossa volume, mean velocity, and the net flow of CSF at the craniovertebral junction.[33] Studies have shown that the earlier arrival and peak velocity of caudal CSF flow are associated with an increased risk of syringomyelia in CM-1 cases.[34]
History and Physical
As syringomyelia is commonly associated with CM-1, examining related clinical features is crucial.
- Tussive headaches: Coughing (Valsalva maneuvers) causes sudden increases in intracranial CSF volume, resulting in transient suboccipital headaches and neck pain a split second after a cough. The features of Chiari headaches are listed below.
- Site: Sub-occipital
- Mode of onset: Sudden
- Nature/character: Heavy, crushing, pressure-like, occasionally pounding when severe but otherwise non-throbbing
- Radiation: Radiates to the vertex, behind the eyes, and inferiorly to the neck and shoulders
- Duration: Brief, lasting only seconds
- Exacerbated by: Physical exertion, Valsalva maneuvers, head dependency, and sudden changes in posture
- Hoarseness, dysphagia, coughing with swallowing due to downward traction on lower cranial nerves and brainstem compression.
- Visual disturbances: Retro-orbital pressure and pain, along with various visual phenomena such as flashing lights, floaters, blurred vision, photophobia, and diplopia. The clinical examination may reveal possible horizontal, rotatory, or down-beat nystagmus due to the involvement of brainstem vestibulo-ocular connections.
- Oto-neurological symptoms: Dizziness, tinnitus, ear pressure, decreased hearing, oscillopsia.
- Cerebellar disturbances: Tremors, dysmetria, ataxia, gait, and balance issues.
- Syncope
Features resulting from the syrinx depend on the anatomical level and include the following conditions:
- Paresthesia/hyperesthesia is the most common sensory symptom, followed by non-radicular segmental pain.[6] Segmental dissociated sensory loss involves loss of pain and temperature sensation but preserves touch and vibratory sense, often manifesting in an upper limb "cape-like" distribution. Lack of pain perception may lead to injuries and chronic skin ulcerations on the hands.
- Muscle weakness and impaired fine motor function may progress to atrophy of intrinsic hand muscles due to damage to anterior horn cells (lower motor neurons) at the syrinx level, potentially resulting in a "claw hand" deformity.
- Spasticity in lower limbs due to syrinx expansion may compress or damage adjacent lateral corticospinal tracts (upper motor neurons).
- Progressive scoliosis resulting from injury to anterior horn cells innervating the paraspinal axial musculature.
- Horner syndrome, which may be observed in cervical or upper thoracic syringes.
The presentation of syringomyelia is highly variable, with patients reporting symptoms such as pain, muscle weakness, particularly in the hands and arms, temperature insensitivity in the upper limb, spasticity or stiffness in the lower limbs, and progressive scoliosis. The clinical course typically progresses over months to years, initially experiencing rapid deterioration that later slows down.[5] A linear relationship is observed between cyst morphology, symptom duration, and severity.[38][39] In cases where associated CM-1 is present, patients may also experience occipital headaches (precipitated by coughing, straining, and sneezing), neck pain, gait, balance problems, dizziness, hoarseness, and swallowing difficulties, as well as sleep disturbances such as snoring.
In patients with syringomyelia secondary to foramen magnum obstruction who undergo treatment with a syringosubarachnoid or thecoperitoneal shunt, an improvement in spasticity exists despite the worsening of other neurological functions. This observation suggests that the spasticity in the limbs may be attributed to the bulk of the syrinx rather than brainstem compression at the level of the foramen magnum.[40]
Classic symptoms such as suspended sensory loss, segmental weakness, and burning sensations are not universally observed in all patients with syringomyelia. The initial symptoms before intervention play a crucial role in predicting the outcome. Dissociative sensory loss typically occurs in cases of centrally located syringomyelia, resulting from the involvement of the gray commissures in lamina X. Patients may also experience autonomic bladder dysfunction. Bowel dysfunction is uncommon until the late stages of spinal cord dysfunction, which is secondary to the involvement of the Clarke nucleus in lamina VII, containing neurons of pre-ganglionic autonomic fiber origin, as well as laminae VIII and IX, associated with modulating skeletal muscle motor function.
The most common symptoms of syringomyelia include radicular pain, gait ataxia, sensory disturbances, dysesthesias, motor weakness, spasticity, autonomic dysreflexia, and neuropathic pain.[12][41]
As syringomyelia progresses, spasticity tends to increase. The progression of the condition is typically slow, with the clinical symptoms often remaining stable for years.[42]
Evaluation
Magnetic Resonance Imaging
MRI, with and without contrast, is the preferred imaging modality (see Image. Syringomyelia Visualized on MRI in a Patient With Hindbrain Herniation). The scan allows for precise delineation of relevant anatomy and accurate visualization of the syrinx in both sagittal and axial planes. MRI quickly reveals crucial information such as the syrinx cavity's location, size, and extent, along with assessing the degree of cerebellar tonsillar ectopia (see Image. Syrinx Visualized on MRI in a Patient With Basilar Invagination).
A ubiquitous feature in patients with associated CM-1 is the compression of retro-cerebellar CSF spaces, which can be clearly observed on MRI. Furthermore, MRI aids in ruling out cystic lesions or spinal tumors and can detect leptomeningeal enhancement indicative of infection, as well as arachnoid scarring. Longitudinal MRI studies can also track syrinx progression over months or years, providing valuable insights into the natural history of syringomyelia (see Image. Holocord Syrinx Visualized on MRI in a Patient With Chiari Malformation).
Dynamic MRI or Cardiac-Gated Cine MRI Flow Study
Phase-contrast MRI is used to study the disturbance of CSF dynamics in detail. This imaging technique enables noninvasive analysis of CSF hydrodynamics, diagnosing velocity or flow disturbances at the foramen magnum (especially in patients with <5 mm tonsillar ectopia), visualizing spinal cord wall motion, and detecting syrinx fluid motion during both cardiac systole and diastole at rest.[6][29] In addition, it proves valuable in documenting postoperative CSF flow changes and objective improvements.
Myelography with High-Resolution Computed Tomography Scan
This imaging modality is recommended in cases where MRI is contraindicated, such as in patients with metallic joint implants or cardiac pacemakers. Delayed computed tomography (CT) scans can effectively visualize dye leached into the syrinx cavity. However, some authors have criticized CT myelography for its low sensitivity in detecting CSF blockage.[43]
Although electromyography lacks diagnostic value in syringomyelia, it helps rule out peripheral neuropathy as a cause of paresthesias.
The configuration of syrinx can be categorized into 4 types—distended, moniliform type (continuous septations ≥3), slender type, and circumscribed.[44]
Treatment / Management
Treatment strategies for syringomyelia include avoiding activities that increase venous pressure, such as straining, flexing the neck, and breath-holding spells, which can help alleviate symptoms by reducing pressure.
Spontaneous resolution of syringomyelia is common among children as their skulls grow and CSF flow is restored. In adults, spontaneous resolution can occur due to various factors, such as the spontaneous rupture of arachnoid adhesions, drainage of the syrinx into the spinal subarachnoid space, or brain atrophy in older patients.[30] Surgical interventions aim to correct the underlying pathophysiology causing syringomyelia, with the primary goal of improving CSF flow dynamics.(B3)
In patients with CM-1, craniocervical decompression is often the recommended approach.[1] This consists of suboccipital craniectomy and removal of the posterior arch of C1, opening the dura and arachnoid, and resection of arachnoid adherences when present.[45] Essentially, this surgical intervention creates an artificially enlarged cisterna magna. Intraoperative ultrasonography can be used to confirm the decompression of the tonsils and ensure pulsatile CSF flow around the craniovertebral junction. The duration of sensory deficits before surgery significantly predicts symptomatic improvement following surgery. Studies have shown that a shorter duration of preoperative symptoms has better outcomes. Therefore, early surgical intervention is crucial to minimize deficits and improve overall outcomes.(B3)
In patients with postinflammatory arachnoid scarring and posttraumatic syringomyelia, the operative procedure is directed toward reconstituting spinal subarachnoid CSF flow by arachnoid scar membrane resection, microsurgical lysis of arachnoid adherences, and dural reconstruction.[46][47](B2)
Shunts are typically considered for idiopathic syringomyelia or in cases where patients have not responded to other treatments. The syringosubarachnoid shunt is the most commonly used shunt procedure, with the syringoperitoneal shunt being an alternative if the former fails. Although some studies suggest better outcomes with the syringosubarachnoid shunt compared to foramen magnum decompression, this recommendation is not universally recognized.[39][48][49] Shunts are generally not preferred and are considered a last resort due to their high complication and failure rates, as well as their inability to address the underlying cause of syringomyelia. (B2)
Surgical Indications
- Symptomatic CM-1-A (CM-1 with syrinx)
- Asymptomatic CM-1-A with a holocord syrinx, clinical-radiological worsening, central syringe with Vaquero index >0.5 or eccentric syringe, and concurrent syringobulbia
- Symptomatic isolated syringomyelia with no consensus for surgery
- Posttraumatic syringomyelia with motor deficits
The key surgical interventions involve osseo-dural decompression of the posterior fossa and complete release of obstruction at the foramen magnum and foramen of Magendie.[12][17] Atlantoaxial stabilization has shown clinical improvements and restoration of spinal alterations and abnormal curvatures.[50](B3)
PPreoperative assessment of intracranial compliance is essential. Patients with low intracranial compliance who undergo treatment with a ventriculoperitoneal shunt before foramen magnum decompression demonstrate regression of syringomyelia in nearly 80% of cases.[51] The use of a fourth ventricle to spinal subarachnoid space stent has been recommended for refractory cases and in tetra-ventricular hydrocephalus.[52][53](A1)
Treatment Modalities
Various treatment modalities are listed below.
- Foramen magnum decompression is typically combined with duraplasty, arachnoid opening, widening of the foramen of Magendie, or tonsillar resection. Obex plugging is less commonly used to prevent the "water hammer" effect.
- If hydrocephalus is also present, shunting or endoscopic third ventriculostomy is used as the initial treatment to relieve pressure on the cerebellar tonsils.
- Endoscopic fenestration of a cystic fourth ventricle or a cyst in the posterior fossa can be considered part of the treatment plan.
- Any relevant spinal pathologies, such as untethering the tethered cord, are addressed. If these interventions are insufficient, additional syrinx shunting procedures may be necessary.
Differential Diagnosis
The differential diagnosis should include the conditions mentioned below.
- Spinal intramedullary tumors, such as hemangioblastoma, ependymoma, and gliomas, may secrete exudative fluid with a high protein content, leading to microcysts that can eventually coalesce. While most intramedullary tumors enhance on contrast MRI (a syrinx does not enhance on contrast MRI), a true syrinx can occur within a tumor.
- Spinal intramedullary cysts, myelomalacia, arachnoid cysts, and glioependymal cysts.
- Residual central spinal canal: The central canal of the spinal cord may involute with age, and a persistent central canal is not considered an anomaly.
Prognosis
Professionals continue to grapple with the elusive natural history of syringomyelia, characterized by its unpredictable and highly variable course, making accurate prognostication challenging. The prognosis hinges on factors such as the underlying cause, the extent of neurological impairment, the location and size of the syrinx cavity, and a syrinx diameter exceeding 5 mm, along with associated edema, which often predicts rapid deterioration. The rarity of the condition, its variable progression, and limited follow-up periods further complicate treatment assessment.[54] However, early surgical intervention is associated with reduced deficits and improved outcomes.
Most studies (99%) have reported using posterior fossa/foramen magnum decompression as the primary surgical intervention. Postoperatively, syringomyelia improved or resolved in nearly 80% of patients.[19] Small-bone-window posterior fossa decompression with duraplasty has emerged as an effective and safe treatment option with a low complication rate.[55] Foramen magnum decompression and duraplasty have shown significant and sustained improvements in both clinical and radiological outcomes. Paradoxically, no association with clinical outcomes exists concerning regression of the syrinx or alterations in the position of the cerebellar tonsillar.[56] The restoration of CSF flow at the craniocervical junction has demonstrated a stronger correlation with improved outcomes following posterior fossa decompression with duraplasty compared to factors like the fourth ventricle area and Vaquero index (syrinx to cord ratio).[57]
The Chicago Chiari Outcome Scale score was also better in the posterior fossa decompression and resection of the tonsils group.[58][59] A recent systematic review and meta-analysis demonstrated a clinical improvement rate of 86.8% in the posterior fossa decompression with duraplasty group compared to 69.8% in the posterior fossa decompression cohort. Medullary decompression and occipital-cervical sagittal realignment have shown resolution of syringomyelia.[60] Foramen magnum decompression with dural patch grafting has exhibited better functional outcomes than dural dissection. Recent meta-analyses highlight the superiority of autologous grafts over non-autologous options in terms of complications.[30] Dura splitting decompression is comparable to posterior fossa decompression with duraplasty in terms of clinical improvement while significantly reducing operative time, hospital stay duration, and CSF-related complications such as CSF leak, meningitis, and pseudomeningocele.[61]
Size, length, and number of syringomyelia are not critical to prognosis. However, size reduction of the syrinx confers high chances of motor improvement compared to sensory disturbance and pain.[62] Motor dysfunction, brainstem herniation, and basilar invagination are predictors of poor clinical prognosis.[55] Autonomic dysfunction and non-cervical site of the syrinx and motor impairments have an unfavorable functional outcome. Cervical syringomyelia, in particular, has the potential for strong functional recovery after adequate intervention, probably owing to minimal CSF pressure caused by gravity compared to thoracic and lumbar areas.[10]
A moniliform variant of posttraumatic syringomyelia shows a better prognosis.[44] Posttraumatic syringomyelia typically affects individuals aged 30 and older with complete spinal cord injury and commonly involves the cervical spine within 5 years post-injury.[63] A systematic review of posttraumatic syringomyelia involving 1803 patients found that the time from spinal cord injury to syringomyelia diagnosis ranged from 42 to 264 months. Surgical management, primarily arachnoid lysis and syrinx drainage, was performed in nearly 90% of cases, with a complication rate of 26%. Postoperative symptom improvement was observed in 43% of patients.[64] The 10-year survival rate among cohorts with syringomyelia following traumatic spinal cord injury is approximately 70%.[65]
Prophylactic neurosurgery may offer benefits in reducing the necessity for spinal curvature correction surgery in patients with a large syrinx (syrinx/cord or S/C ratio >0.7).[66]
Despite undergoing posterior fossa decompression, persistent, recurrent, or worsening syringomyelia may occur in 10% to 50% of cases. They can be categorized into:
- Group I: Cases with insufficient decompression may require repeat posterior fossa decompression or dredging of the foramen magnum and foramen of Magendie.
- Group II: Cases involving craniocervical instability may necessitate atlantoaxial fusion surgery.
- Group III: Cases related to local spinal pathologies such as fractures, tumors, and cysts may be managed with modalities such as ventriculoperitoneal shunt, syringo-subarachnoid shunt, and pulsed radiofrequency treatment.[13]
Complications
Myelopathy is a significant complication resulting from the disease process. It can lead to spasticity, which may progress to paraplegia/quadriplegia, decubitus ulcers, recurrent pneumonia, and bowel and bladder dysfunction. Additional complications include neuropathic pain and neuro-arthropathy.
Kyphoscoliosis is the result of a reduction in spinal length.[67][68]
Postoperative complications have been reported in 41% of cases in one series, with the most common complications being CSF leak, pseudomeningocele, aseptic meningitis, wound infection, meningitis, and neurological deficits, resulting in a mean complication rate of 4.5%. Mortality rates were found to be 11% in the same study, with no observed difference between pediatric and adult series.[19]
Deterrence and Patient Education
Patient education should include the following considerations:
- Patients with untreated syringomyelia should avoid activities that can increase intracranial or intra-abdominal pressure, such as straining during bowel movements, coughing, sneezing, and lifting heavy weights to prevent worsening symptoms and further enlarging the syrinx. This caution is particularly important in the initial weeks after surgery, especially when patients may be taking narcotic pain medication that can cause constipation. Patients should promptly consult their doctor if they experience symptoms such as a persistent cough or constipation.
- Patients with Chiari malformation should avoid activities that strain the neck, such as roller coasters and trampolines, and refrain from contact sports like football. Alternative forms of exercise like swimming, stationary bicycling, and yoga are recommended.
- Patients should immediately report to the treating clinician any postoperative drainage of purulent fluid from the surgical site or signs of infection, such as a painful, edematous, or reddened wound.
Pearls and Other Issues
The key points are as follows:
- Syringomyelia should be prominently considered in the differential diagnosis of any young person with progressive scoliosis. Early identification and treatment can reverse the deformity.
- In most cases, hand involvement in syringomyelia patients is frequently asymmetric due to the eccentricity of the syrinx cavity.
- Clinicians need to distinguish Chiari headaches, and a patient's history is crucial in this regard.
- A history of long-duration headaches and pain relief with neck support can help identify headaches originating in neck muscles that may extend into the suboccipital area.
- Posterior fossa brain tumors may produce similar headaches and also cause tonsillar descent. However, these headaches are of prolonged duration and are often accompanied by projectile vomiting. Fundoscopy in these patients may also reveal papilledema.
- Headaches in fibromyalgia patients may also mimic Chiari headaches.
- Being a chronic disorder, a patient with syringomyelia does not typically present symptoms such as anxiety, memory impairment, and depression. Clinicians must assess all symptoms appropriately, especially considering the potential for specific symptoms to improve following surgery.[69][70][71]
Identifying and distinguishing the root cause of deficits in posttraumatic syringomyelia, whether it is due to the syrinx cavity or cord injury, remains challenging.
Enhancing Healthcare Team Outcomes
Postoperative pain following surgery is a significant concern for patients and is often managed with opioids and muscle relaxants. Patients and their family members should understand that clinicians cannot overmedicate. Pain medications have both benefits and risks, so the risk-benefit ratio must be carefully considered. Excessive sedation with opioids can increase the risk of complications such as pneumonia. Therefore, clinicians must titrate the dose of pain medications carefully to achieve maximum comfort with minimal risk of complications. In addition, the patient and their family and friends must understand and respect this delicate balance. A well-informed patient can contribute significantly to the decision-making process by understanding the proposed treatment strategy, diagnostic workup, and subsequent monitoring.
Media
(Click Image to Enlarge)

Syringomyelia Visualized on MRI in a Patient With Hindbrain Herniation.
Contributed by V Shenoy, MD, MBBS
(Click Image to Enlarge)
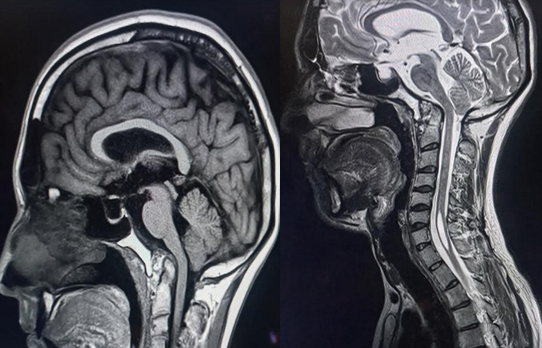
Syrinx Visualized on MRI in a Patient With Basilar Invagination.
Contributed by S Munakomi, MD
(Click Image to Enlarge)
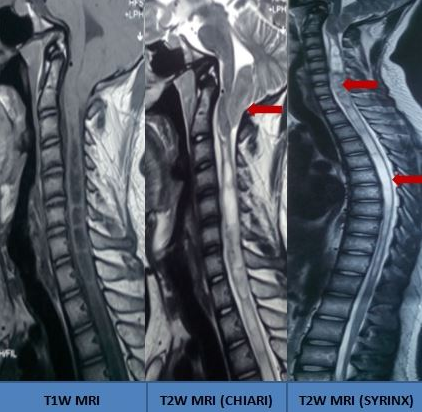
Holocord Syrinx Visualized on MRI in a Patient With Chiari Malformation.
Contributed by S Munakomi, MD
References
Roy AK, Slimack NP, Ganju A. Idiopathic syringomyelia: retrospective case series, comprehensive review, and update on management. Neurosurgical focus. 2011 Dec:31(6):E15. doi: 10.3171/2011.9.FOCUS11198. Epub [PubMed PMID: 22133183]
Level 3 (low-level) evidenceKlekamp J, Batzdorf U, Samii M, Bothe HW. Treatment of syringomyelia associated with arachnoid scarring caused by arachnoiditis or trauma. Journal of neurosurgery. 1997 Feb:86(2):233-40 [PubMed PMID: 9010425]
Level 2 (mid-level) evidenceGreitz D. Unraveling the riddle of syringomyelia. Neurosurgical review. 2006 Oct:29(4):251-63; discussion 264 [PubMed PMID: 16752160]
Level 3 (low-level) evidenceRoser F, Ebner FH, Sixt C, Hagen JM, Tatagiba MS. Defining the line between hydromyelia and syringomyelia. A differentiation is possible based on electrophysiological and magnetic resonance imaging studies. Acta neurochirurgica. 2010 Feb:152(2):213-9; discussion 219. doi: 10.1007/s00701-009-0427-x. Epub 2009 Jun 16 [PubMed PMID: 19533016]
Bogdanov EI, Mendelevich EG. Syrinx size and duration of symptoms predict the pace of progressive myelopathy: retrospective analysis of 103 unoperated cases with craniocervical junction malformations and syringomyelia. Clinical neurology and neurosurgery. 2002 May:104(2):90-7 [PubMed PMID: 11932037]
Level 2 (mid-level) evidenceMilhorat TH, Chou MW, Trinidad EM, Kula RW, Mandell M, Wolpert C, Speer MC. Chiari I malformation redefined: clinical and radiographic findings for 364 symptomatic patients. Neurosurgery. 1999 May:44(5):1005-17 [PubMed PMID: 10232534]
Level 2 (mid-level) evidenceMampalam TJ, Andrews BT, Gelb D, Ferriero D, Pitts LH. Presentation of type I Chiari malformation after head trauma. Neurosurgery. 1988 Dec:23(6):760-2 [PubMed PMID: 3216976]
Level 3 (low-level) evidenceWilliams B. Post-traumatic syringomyelia, an update. Paraplegia. 1990 Jun:28(5):296-313 [PubMed PMID: 2235038]
Level 3 (low-level) evidenceZuev AA, Kostenko GV. [Treatment of syringomyelia associated with Chiari 1 malformation]. Zhurnal nevrologii i psikhiatrii imeni S.S. Korsakova. 2017:117(3):102-106. doi: 10.17116/jnevro201711731102-106. Epub [PubMed PMID: 28399105]
Zheng YC, Liu YT, Wei KC, Huang YC, Chen PY, Hsu YH, Lin CL. Outcome predictors and clinical presentation of syringomyelia. Asian journal of surgery. 2023 Feb:46(2):705-711. doi: 10.1016/j.asjsur.2022.06.150. Epub 2022 Jul 20 [PubMed PMID: 35868963]
Milhorat TH, Capocelli AL Jr, Anzil AP, Kotzen RM, Milhorat RH. Pathological basis of spinal cord cavitation in syringomyelia: analysis of 105 autopsy cases. Journal of neurosurgery. 1995 May:82(5):802-12 [PubMed PMID: 7714606]
Level 3 (low-level) evidenceCiaramitaro P, Garbossa D, Peretta P, Piatelli G, Massimi L, Valentini L, Migliaretti G, Baldovino S, Roccatello D, Kodra Y, Taruscio D, Interregional Chiari and Syringomyelia Consortium, on behalf of the Interregional Chiari and Syringomyelia Consortium. Syringomyelia and Chiari Syndrome Registry: advances in epidemiology, clinical phenotypes and natural history based on a North Western Italy cohort. Annali dell'Istituto superiore di sanita. 2020 Jan-Mar:56(1):48-58. doi: 10.4415/ANN_20_01_08. Epub [PubMed PMID: 32242535]
Level 3 (low-level) evidenceYuan C, Guan J, Du Y, Fang Z, Wang X, Yao Q, Zhang C, Liu Z, Wang K, Duan W, Wang X, Wang Z, Wu H, Jian F. Neurological deterioration after posterior fossa decompression for adult syringomyelia: Proposal for a summarized treatment algorithm. Frontiers in surgery. 2022:9():968906. doi: 10.3389/fsurg.2022.968906. Epub 2022 Sep 15 [PubMed PMID: 36189393]
Gade SP, Harjpal P, Kovela RK. Novelty in Impact of Neurorehabilitation in a Classic Case of Syringomyelia. Cureus. 2022 Sep:14(9):e29126. doi: 10.7759/cureus.29126. Epub 2022 Sep 13 [PubMed PMID: 36258946]
Level 3 (low-level) evidenceThi Phuong Dinh H, Tomohiko H, Madelar RT, Dinh Anh Hoang H, Yukihiro M. Giant-Cell Ependymoma of the Cervical Spinal Cord With Syringomyelia and Pathological Presentation: A Case Report and Review of the Literature. Cureus. 2022 Dec:14(12):e33174. doi: 10.7759/cureus.33174. Epub 2022 Dec 31 [PubMed PMID: 36726917]
Level 3 (low-level) evidenceHow Hong EA, Shalid A, Deepak S, Kounin G. Posterior Cranial Fossa Meningioma Causing Tonsillar Herniation and Giant Cervicothoracic Syringomyelia: Case Report and Review of Literature. Asian journal of neurosurgery. 2022 Sep:17(3):515-520. doi: 10.1055/s-0042-1756634. Epub 2022 Oct 8 [PubMed PMID: 36398186]
Level 3 (low-level) evidenceGuan J, Yuan C, Zhang C, Ma L, Yao Q, Cheng L, Liu Z, Wang K, Duan W, Wang X, Wu H, Chen Z, Jian F. Intradural Pathology Causing Cerebrospinal Fluid Obstruction in Syringomyelia and Effectiveness of Foramen Magnum and Foramen of Magendie Dredging Treatment. World neurosurgery. 2020 Dec:144():e178-e188. doi: 10.1016/j.wneu.2020.08.068. Epub 2020 Aug 15 [PubMed PMID: 32805463]
Shao B, Wojcik D, Ma KL, Amaral-Nieves N, Poggi JA, Leary OP, Klinge PM. Reappraisal of intradural findings in Chiari malformation type I. Neurosurgical focus. 2023 Mar:54(3):E2. doi: 10.3171/2022.12.FOCUS22628. Epub [PubMed PMID: 36857788]
Arnautovic A, Splavski B, Boop FA, Arnautovic KI. Pediatric and adult Chiari malformation Type I surgical series 1965-2013: a review of demographics, operative treatment, and outcomes. Journal of neurosurgery. Pediatrics. 2015 Feb:15(2):161-77. doi: 10.3171/2014.10.PEDS14295. Epub 2014 Dec 5 [PubMed PMID: 25479580]
Holste KG, Muraszko KM, Maher CO. Epidemiology of Chiari I Malformation and Syringomyelia. Neurosurgery clinics of North America. 2023 Jan:34(1):9-15. doi: 10.1016/j.nec.2022.08.001. Epub 2022 Nov 3 [PubMed PMID: 36424068]
GARDNER WJ, ANGEL J. The mechanism of syringomyelia and its surgical correction. Clinical neurosurgery. 1958:6():131-40 [PubMed PMID: 13826542]
Williams B. Pathogenesis of syringomyelia. Lancet (London, England). 1972 Nov 4:2(7784):969-70 [PubMed PMID: 4116840]
Williams B. On the pathogenesis of syringomyelia: a review. Journal of the Royal Society of Medicine. 1980 Nov:73(11):798-806 [PubMed PMID: 7017117]
Level 3 (low-level) evidenceOldfield EH, Muraszko K, Shawker TH, Patronas NJ. Pathophysiology of syringomyelia associated with Chiari I malformation of the cerebellar tonsils. Implications for diagnosis and treatment. Journal of neurosurgery. 1994 Jan:80(1):3-15 [PubMed PMID: 8271018]
Milhorat TH, Miller JI, Johnson WD, Adler DE, Heger IM. Anatomical basis of syringomyelia occurring with hindbrain lesions. Neurosurgery. 1993 May:32(5):748-54; discussion 754 [PubMed PMID: 8492850]
Ball MJ, Dayan AD. Pathogenesis of syringomyelia. Lancet (London, England). 1972 Oct 14:2(7781):799-801 [PubMed PMID: 4116236]
Oldfield EH. Pathogenesis of Chiari I - Pathophysiology of Syringomyelia: Implications for Therapy: A Summary of 3 Decades of Clinical Research. Neurosurgery. 2017 Sep 1:64(CN_suppl_1):66-77. doi: 10.1093/neuros/nyx377. Epub [PubMed PMID: 28899066]
Koyanagi I, Houkin K. Pathogenesis of syringomyelia associated with Chiari type 1 malformation: review of evidences and proposal of a new hypothesis. Neurosurgical review. 2010 Jul:33(3):271-84; discussion 284-5. doi: 10.1007/s10143-010-0266-5. Epub 2010 Jun 8 [PubMed PMID: 20532585]
Honey CM, Martin KW, Heran MKS. Syringomyelia Fluid Dynamics and Cord Motion Revealed by Serendipitous Null Point Artifacts during Cine MRI. AJNR. American journal of neuroradiology. 2017 Sep:38(9):1845-1847. doi: 10.3174/ajnr.A5328. Epub 2017 Jul 27 [PubMed PMID: 28751514]
Van Der Veken J, Harding M, Hatami S, Agzarian M, Vrodos N. Syringomyelia intermittens: highlighting the complex pathophysiology of syringomyelia. Illustrative case. Journal of neurosurgery. Case lessons. 2021 Sep 13:2(11):CASE21341. doi: 10.3171/CASE21341. Epub 2021 Sep 13 [PubMed PMID: 35855301]
Level 3 (low-level) evidenceWang X, Jiang C, Lu C, Ma L, Feng Y, Cui S, Li Q, Li K, Wang X, Jian F. Impairment of Connexin 43 may initiate cilia decline in syringomyelia. Experimental neurology. 2023 Jul:365():114430. doi: 10.1016/j.expneurol.2023.114430. Epub 2023 Apr 28 [PubMed PMID: 37121428]
Halvorson KG, Kellogg RT, Keachie KN, Grant GA, Muh CR, Waldau B. Morphometric Analysis of Predictors of Cervical Syrinx Formation in the Setting of Chiari I Malformation. Pediatric neurosurgery. 2016:51(3):137-41. doi: 10.1159/000442991. Epub 2016 Feb 13 [PubMed PMID: 26871424]
Wang S, Zhang D, Wu K, Fan W, Fan T. Potential association among posterior fossa bony volume and crowdedness, tonsillar hernia, syringomyelia, and CSF dynamics at the craniocervical junction in Chiari malformation type I. Frontiers in neurology. 2023:14():1069861. doi: 10.3389/fneur.2023.1069861. Epub 2023 Feb 20 [PubMed PMID: 36891476]
Clarke EC, Stoodley MA, Bilston LE. Changes in temporal flow characteristics of CSF in Chiari malformation Type I with and without syringomyelia: implications for theory of syrinx development. Journal of neurosurgery. 2013 May:118(5):1135-40. doi: 10.3171/2013.2.JNS12759. Epub 2013 Mar 15 [PubMed PMID: 23495878]
Level 2 (mid-level) evidenceWeig SG, Buckthal PE, Choi SK, Zellem RT. Recurrent syncope as the presenting symptom of Arnold-Chiari malformation. Neurology. 1991 Oct:41(10):1673-4 [PubMed PMID: 1922816]
Batzdorf U, Khoo LT, McArthur DL. Observations on spine deformity and syringomyelia. Neurosurgery. 2007 Aug:61(2):370-7; discussion 377-8 [PubMed PMID: 17762750]
Level 3 (low-level) evidenceMilhorat TH, Mu HT, LaMotte CC, Milhorat AT. Distribution of substance P in the spinal cord of patients with syringomyelia. Journal of neurosurgery. 1996 Jun:84(6):992-8 [PubMed PMID: 8847594]
Grant R, Hadley DM, Macpherson P, Condon B, Patterson J, Bone I, Teasdale GN. Syringomyelia: cyst measurement by magnetic resonance imaging and comparison with symptoms, signs and disability. Journal of neurology, neurosurgery, and psychiatry. 1987 Aug:50(8):1008-14 [PubMed PMID: 3655805]
Fujii K, Natori Y, Nakagaki H, Fukui M. Management of syringomyelia associated with Chiari malformation: comparative study of syrinx size and symptoms by magnetic resonance imaging. Surgical neurology. 1991 Oct:36(4):281-5 [PubMed PMID: 1948628]
Level 2 (mid-level) evidenceGoel A, Desai K. Surgery for syringomyelia: an analysis based on 163 surgical cases. Acta neurochirurgica. 2000:142(3):293-301; discussion 301-2 [PubMed PMID: 10819260]
Level 3 (low-level) evidenceBrodbelt AR, Stoodley MA. Post-traumatic syringomyelia: a review. Journal of clinical neuroscience : official journal of the Neurosurgical Society of Australasia. 2003 Jul:10(4):401-8 [PubMed PMID: 12852875]
Mariani C, Cislaghi MG, Barbieri S, Filizzolo F, Di Palma F, Farina E, D'Aliberti G, Scarlato G. The natural history and results of surgery in 50 cases of syringomyelia. Journal of neurology. 1991 Dec:238(8):433-8 [PubMed PMID: 1779249]
Level 2 (mid-level) evidenceMauer UM, Freude G, Danz B, Kunz U. Cardiac-gated phase-contrast magnetic resonance imaging of cerebrospinal fluid flow in the diagnosis of idiopathic syringomyelia. Neurosurgery. 2008 Dec:63(6):1139-44; discussion 1144. doi: 10.1227/01.NEU.0000334411.93870.45. Epub [PubMed PMID: 19057326]
Lu C, Ma L, Yuan C, Cheng L, Wang X, Duan W, Wang K, Chen Z, Wu H, Zeng G, Jian F. Phenotypes and Prognostic Factors of Syringomyelia in Single-Center Patients With Chiari I Malformation: Moniliform Type as a Special Configuration. Neurospine. 2022 Sep:19(3):816-827. doi: 10.14245/ns.2244332.166. Epub 2022 Sep 30 [PubMed PMID: 36203304]
Dyste GN, Menezes AH, VanGilder JC. Symptomatic Chiari malformations. An analysis of presentation, management, and long-term outcome. Journal of neurosurgery. 1989 Aug:71(2):159-68 [PubMed PMID: 2746341]
Attal N, Parker F, Tadié M, Aghakani N, Bouhassira D. Effects of surgery on the sensory deficits of syringomyelia and predictors of outcome: a long term prospective study. Journal of neurology, neurosurgery, and psychiatry. 2004 Jul:75(7):1025-30 [PubMed PMID: 15201364]
Lee TT, Alameda GJ, Camilo E, Green BA. Surgical treatment of post-traumatic myelopathy associated with syringomyelia. Spine. 2001 Dec 15:26(24 Suppl):S119-27 [PubMed PMID: 11805618]
Level 2 (mid-level) evidenceHida K, Iwasaki Y, Koyanagi I, Sawamura Y, Abe H. Surgical indication and results of foramen magnum decompression versus syringosubarachnoid shunting for syringomyelia associated with Chiari I malformation. Neurosurgery. 1995 Oct:37(4):673-8; discussion 678-9 [PubMed PMID: 8559295]
Level 2 (mid-level) evidenceGrant R, Hadley DM, Lang D, Condon B, Johnston R, Bone I, Teasdale GM. MRI measurement of syrinx size before and after operation. Journal of neurology, neurosurgery, and psychiatry. 1987 Dec:50(12):1685-7 [PubMed PMID: 3437304]
Goel A. Scoliosis and Syringomyelia. Neurology India. 2022 Sep-Oct:70(5):2192-2193. doi: 10.4103/0028-3886.359263. Epub [PubMed PMID: 36352639]
Frič R, Ringstad G, Eide PK. Low versus High Intracranial Compliance in Adult Patients with Chiari Malformation Type 1-Comparison of Long-Term Outcome After Tailored Treatment. World neurosurgery. 2023 May:173():e699-e707. doi: 10.1016/j.wneu.2023.02.134. Epub 2023 Mar 6 [PubMed PMID: 36889634]
Spennato P, Vitulli F, Tafuto R, Imperato A, Mirone G, Cinalli G. Fourth ventricle to spinal subarachnoid space stenting in pediatric patients with refractory syringomyelia: case series and systematic review. Neurosurgical review. 2023 Mar 11:46(1):67. doi: 10.1007/s10143-023-01972-y. Epub 2023 Mar 11 [PubMed PMID: 36905420]
Level 1 (high-level) evidenceHan RK, Medina MP, Giantini-Larsen AM, Chae JK, Cruz A, Garton ALA, Greenfield JP. Fourth ventricular subarachnoid stent for Chiari malformation type I-associated persistent syringomyelia. Neurosurgical focus. 2023 Mar:54(3):E10. doi: 10.3171/2022.12.FOCUS22633. Epub [PubMed PMID: 36857783]
Logue V, Edwards MR. Syringomyelia and its surgical treatment--an analysis of 75 patients. Journal of neurology, neurosurgery, and psychiatry. 1981 Apr:44(4):273-84 [PubMed PMID: 7241155]
Deng X, Yang C, Gan J, Wu L, Yang T, Yang J, Xu Y. Long-Term Outcomes After Small-Bone-Window Posterior Fossa Decompression and Duraplasty in Adults with Chiari Malformation Type I. World neurosurgery. 2015 Oct:84(4):998-1004. doi: 10.1016/j.wneu.2015.02.006. Epub 2015 Feb 18 [PubMed PMID: 25701768]
Level 2 (mid-level) evidenceWang B, Wang C, Zhang YW, Liang YC, Liu WH, Yang J, Xu YL, Wang YZ, Jia WQ. Long-term outcomes of foramen magnum decompression with duraplasty for Chiari malformation type I in adults: a series of 297 patients. Neurosurgical focus. 2023 Mar:54(3):E5. doi: 10.3171/2022.12.FOCUS22627. Epub [PubMed PMID: 36857791]
Cai Y, Wang C, Chai S, Li G, Zhang T, Liu Z, Yi D, Chen J, Hu J, Liu K, Xiong N. Prognostic analysis of posterior fossa decompression with or without cerebellar tonsillectomy for Chiari malformation type I: a multicenter retrospective study. Neurosurgical focus. 2023 Mar:54(3):E4. doi: 10.3171/2022.12.FOCUS22626. Epub [PubMed PMID: 36857790]
Level 2 (mid-level) evidenceZhang M, Hu Y, Song D, Duan C, Wei M, Zhang L, Lei S, Guo F. Exploring the prognostic differences in patients of Chiari malformation type I with syringomyelia undergoing different surgical methods. Frontiers in neurology. 2022:13():1062239. doi: 10.3389/fneur.2022.1062239. Epub 2023 Jan 4 [PubMed PMID: 36686516]
Yang M, Niu HT, Jiang HS, Wang YZ. Posterior fossa decompression and duraplasty with and without tonsillar resection for the treatment of adult Chiari malformation type I and syringomyelia. Medicine. 2022 Dec 16:101(50):e31394. doi: 10.1097/MD.0000000000031394. Epub [PubMed PMID: 36550873]
Lu C, Duan W, Zhang C, Du Y, Wang X, Ma L, Wang K, Wu H, Chen Z, Jian F. Correlation Among Syrinx Resolution, Cervical Sagittal Realignment, and Surgical Outcome After Posterior Reduction for Basilar Invagination, Atlantoaxial Dislocation, and Syringomyelia. Operative neurosurgery (Hagerstown, Md.). 2023 Aug 1:25(2):125-135. doi: 10.1227/ons.0000000000000719. Epub 2023 Apr 21 [PubMed PMID: 37083634]
Chang TW, Zhang X, Maoliti W, Yuan Q, Yang XP, Wang JC. Outcomes of Dura Splitting Decompression Versus Posterior Fossa Decompression With Duraplasty in the Treatment of Chiari I Malformation: A Systematic Review and Meta-analysis. World neurosurgery. 2021 Mar:147():105-114. doi: 10.1016/j.wneu.2020.11.163. Epub 2020 Dec 5 [PubMed PMID: 33290896]
Level 1 (high-level) evidenceSakushima K, Hida K, Yabe I, Tsuboi S, Uehara R, Sasaki H. Different surgical treatment techniques used by neurosurgeons and orthopedists for syringomyelia caused by Chiari I malformation in Japan. Journal of neurosurgery. Spine. 2013 Jun:18(6):588-92. doi: 10.3171/2013.3.SPINE12837. Epub 2013 Apr 19 [PubMed PMID: 23600586]
Krebs J, Koch HG, Hartmann K, Frotzler A. The characteristics of posttraumatic syringomyelia. Spinal cord. 2016 Jun:54(6):463-6. doi: 10.1038/sc.2015.218. Epub 2015 Dec 1 [PubMed PMID: 26620880]
Kleindienst A, Laut FM, Roeckelein V, Buchfelder M, Dodoo-Schittko F. Treatment of posttraumatic syringomyelia: evidence from a systematic review. Acta neurochirurgica. 2020 Oct:162(10):2541-2556. doi: 10.1007/s00701-020-04529-w. Epub 2020 Aug 20 [PubMed PMID: 32820376]
Level 1 (high-level) evidenceChen CM, Huang WC, Yang YH, Huang SS, Lu KY. Factors affecting long-term mortality rate after diagnosis of syringomyelia in disabled spinal cord injury patients: a population-based study. Spinal cord. 2020 Apr:58(4):402-410. doi: 10.1038/s41393-019-0363-4. Epub 2019 Oct 10 [PubMed PMID: 31602006]
Zhu C, Huang S, Song Y, Liu H, Liu L, Yang X, Zhou C, Hu B, Chen H. Surgical Treatment of Scoliosis-Associated with Syringomyelia: The Role of Syrinx Size. Neurology India. 2020 Mar-Apr:68(2):299-304. doi: 10.4103/0028-3886.280648. Epub [PubMed PMID: 32189709]
Bleck TP, Shannon KM. Disordered swallowing due to a syrinx: correction by shunting. Neurology. 1984 Nov:34(11):1497-8 [PubMed PMID: 6493500]
Level 3 (low-level) evidenceMasmoudi K, Feki A, Akrout R, Baklouti S. Neuropathic arthropathy of the wrist revealing a syringomyelia. BMJ case reports. 2022 Nov 25:15(11):. doi: 10.1136/bcr-2022-249804. Epub 2022 Nov 25 [PubMed PMID: 36428034]
Level 3 (low-level) evidenceMuhonen MG, Menezes AH, Sawin PD, Weinstein SL. Scoliosis in pediatric Chiari malformations without myelodysplasia. Journal of neurosurgery. 1992 Jul:77(1):69-77 [PubMed PMID: 1607974]
Level 3 (low-level) evidenceWatson NF, Buchwald D, Goldberg J, Maravilla KR, Noonan C, Guan Q, Ellenbogen RG. Is Chiari I malformation associated with fibromyalgia? Neurosurgery. 2011 Feb:68(2):443-8; discussion 448-9. doi: 10.1227/NEU.0b013e3182039a31. Epub [PubMed PMID: 21135714]
Mueller DM, Oro' JJ. Prospective analysis of presenting symptoms among 265 patients with radiographic evidence of Chiari malformation type I with or without syringomyelia. Journal of the American Academy of Nurse Practitioners. 2004 Mar:16(3):134-8 [PubMed PMID: 15130068]