
Introduction
Pityriasis rubra pilaris (PRP) is a rare inflammatory papulosquamous disorder of unknown etiology. There are 6 clinical subtypes, which occur in both children and adults. Common elements noted across all subtypes include palmoplantar keratoderma and follicular papules coalescing into well-demarcated plaques of various sizes with characteristic reddish-orange hue and non-adherent, flaking scale. More generalized subtypes often demonstrate intervening areas of unaffected skin, known as "islands of sparing," a signature characteristic of PRP. However, this feature may occasionally be found in PRP-mimickers (eg, psoriasis or mycosis fungoides), especially when these patients are erythrodermic.
Patients with PRP have a broad spectrum of presentations, from mild disease isolated to extensor extremities to diffuse erythroderma involving 90% to 100% of body surface area, as well as intense itching, skin tightness, burning, stinging, and pain. In some cases, PRP is self-limited and asymptomatic; however, in symptomatic chronic cases, continued treatment is indicated, primarily consisting of topical treatments for symptomatic management and systemic therapy to reduce inflammation.[1][2][3][4][5]
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
The etiology of PRP remains elusive. PRP-like eruptions have been associated with some medications, especially ponatinib or other kinase inhibitors.[6] Although PRP has been temporally associated with viral infections, vaccinations, injuries, and other illnesses, these are not consistent, and distinguishing temporal associations from causality is difficult. There are multiple case reports associating PRP with malignancy, although the cutaneous manifestations of PRP in these cases tend to be atypical, and the range of associated tumors is varied.[7]
Epidemiology
PRP occurs worldwide. Estimates of prevalence range from 1 in 500 new patient dermatology visits in Kenya to 1 in 5000 new dermatology visits in Great Britain to 1 in 50,000 new dermatology visits in India.[8][9][10] The prevalence of PRP between males and females is approximately equal, although some publications suggest a slight male predominance.[7] The onset of PRP can occur at all ages, with slight bimodal peaks during the first to second and fifth to sixth decades of life.[11] Most cases appear to be sporadic, though familial cases also occur. The familial inheritance pattern is usually autosomal dominant with gain-of-function gene variations found in CARD14.[12]
Pathophysiology
Inherited PRP, which usually presents before age 2, is associated with gain-of-function gene variations in CARD14, found in the psoriasis susceptibility locus 2 (PSORS2), a gene that activates Nuclear Factor-kappa B (NFkB).[12] Occasionally, these gene variations have also been noted in patients with sporadic adult-onset PRP.[13] CARD14 gene variations are also found in familial psoriasis, highlighting the overlap between PRP and psoriasis.[14]
Like psoriasis, classical PRP is associated with activation of the Th17/IL23 inflammatory pathways.[15][16] Transgenic mouse models that recapitulate the epidermal CARD14 gene variations found in PRP and psoriasis caused induction of NFkB and activation of the IL23-IL17A cytokine axis,[17][18] suggesting that genetic and sporadic PRP have similar underlying inflammatory pathways. Transcriptomics comparison between skin from patients with psoriasis and PRP showed a complete overlap of dysregulated genes, such that all significantly dysregulated genes in PRP were also found in psoriasis skin, further highlighting the shared pathophysiology between PRP and psoriasis.[19]
Histopathology
PRP classically presents with irregular, psoriasiform acanthosis of the epidermis and a characteristic overlying "checkerboard" pattern of parakeratosis, alternating vertical and horizontal ortho- and parakeratosis. Follicular plugging with shoulder parakeratosis is often noted also. Findings of thick, rather than thin, suprapapillary plates and lack of neutrophils in the stratum corneum may help distinguish PRP from psoriasis. Typically, with PRP, the granular layer is normal or thickened under areas of parakeratosis on histologic evaluation. Furthermore, variable mild superficial perivascular lymphohistiocytic infiltrate, occasional mild epidermal spongiosis, eosinophils, and focal acantholytic dyskeratosis, which histopathologically resembles Grover's disease, have been reported but are not consistently found.[20] While acantholysis may be seen in <25% of cases, this finding can further help distinguish PRP from psoriasis.[21]
History and Physical
The clinical spectrum of PRP was initially divided into 5 subtypes using a widely accepted classification scheme proposed by Griffiths in 1980, based on the onset (ie, childhood versus adult), lesion characteristics, and distribution.[10] Griffiths also suggested that these clinical subtypes were predictive of clinical prognosis, but these predictions were not validated and have not been held in clinical trials.[22][23] A sixth subtype was added due to reports of association with HIV.[24][25] Finally, patients with early-onset PRP associated with CARD14 gene variations have been proposed as a separate entity, entitled CARD14-associated papulosquamous eruption (CAPE).[26] The following are the subtypes of PRP:
- Type I: classical adult-onset
- Type II: atypical adult-onset
- Type III: classical juvenile-onset
- Type IV: circumscribed juvenile-onset
- Type V: atypical juvenile-onset
- Type VI: HIV-associated
- CARD14-associated papulosquamous eruption (CAPE)
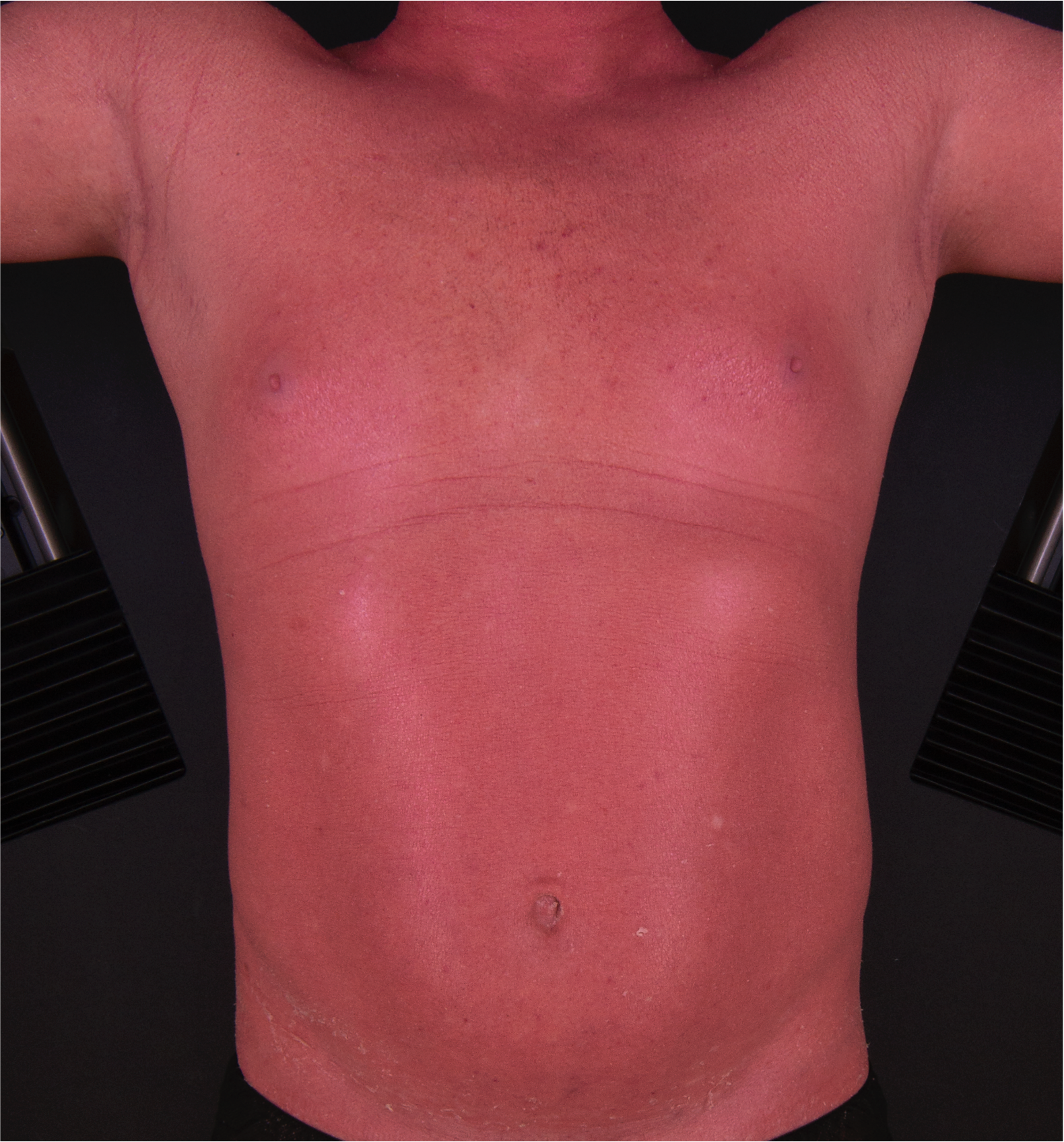
The cardinal features across subtypes include palmoplantar hyperkeratosis and hyperkeratotic follicular papules coalescing into well-demarcated red-orange plaques. (see Image. Pityriasis Rubra Pilaris). Limited or circumscribed variants may be only mildly pruritic. In contrast, widespread PRP is associated with severe pruritus and pain interfering with activities of daily living and quality of life and an increased risk of suicidal ideation.[27][28][3] (see Image. Severe Pityriasis Rubra Pilaris).
Type I Classical Adult Pityriasis Rubra Pilaris
Type I PRP affects 55% of patients and is the most common in adults.[10] The classic sequence of signs in type I PRP begins with a fine scale and erythema on the scalp, which may be initially mistaken for seborrheic dermatitis. Small groups of follicular hyperkeratotic papules may be noted on the dorsal fingers or the head and neck. Various terms, including “nutmeg grater” or “exaggerated gooseflesh,” have been used to describe these grid-line arrays of follicular-based papules.(see Image. Pityriasis Rubra Pilaris Lesions). Within weeks to a few months, more papules erupt and coalesce into plaques that progress in a cephalocaudal manner. Involved skin is often sharply demarcated from adjacent uninvolved skin, producing a characteristic phenomenon termed “islands of sparing.” (see Image. Islands of Sparing in Pityriasis Rubra Pilaris).
The disease often progresses into diffuse erythrodermic plaques, in which the follicular papules are no longer visible.[29] (see Image. Pityriasis Rubra Pilaris With Erythroderma.) The epidermal scale is fine and nonadherent, termed pityriasiform or furfuraceous scaling, although it may be thicker and more adherent on the face and scalp. In deeply pigmented skin, the characteristics lesions of PRP appear hyperpigmented with subtle dark red to violaceous erythema. (see Image. Pityriasis Rubra Pilaris of the Dorsal Foot). In lightly pigmented skin, the lesions are pink-red to salmon-orange. Dermoscopy may reveal a keratotic whitish plug with central hair and surrounding yellow-pink to dark brown halo with dotted vessels.[30] Palmoplantar keratoderma (PPK) is another characteristic finding in PRP and classically has a unique waxy red-orange or bright yellow color. Nail involvement is common, with subungual hyperkeratosis, splinter hemorrhages, and longitudinal ridging. (see Image. Pityriasis Rubra Pilaris with Keratoderma). Eruptive seborrheic keratoses are occasionally found in erythrodermic PRP; these have not been associated with malignancy, as would be considered in the sign of Leser-Trelat.[31][32] During the resolution phase of PRP, cutaneous plaques may form an erythema gyratum repens-like morphology, with parallel arcuate rings resembling wood grain. This likewise has not been associated with malignancy when it occurs in association with PRP, as compared with true erythema gyratum repens, which often is a sign of underlying malignancy.[33] (see Image. Gyratum-Repens Like Pityriasis Rubra Pilaris).
Noncutaneous complications of widespread or erythrodermic PRP include ectropion of the lower eyelids that occasionally results in keratitis, the buildup of wax and scale in the external auditory canals that may muffle hearing, rhinorrhea, hair loss, edema of the limbs, anhidrosis (ie, lack of sweating), and difficulty with body temperature regulation. Common physical symptoms of widespread PRP include severe pruritus, a burning sensation in the involved skin, painful palmoplantar fissures, arthralgias, poor sleep, and fatigue. These symptoms may lead to loss of fine motor ability, difficulty walking, difficulty wearing regular clothing due to dysesthesia, and difficulty leaving the home. Common mental health impacts reported by people with severe PRP include depression, anxiety, embarrassment, loneliness, loss of self-esteem, memory loss or brain fog, and passive or active suicidal ideation.[27]
Type II Atypical Adult Pityriasis Rubra Pilaris
Type II PRP reportedly affects 5% of patients with PRP.[10] Clinical findings of type II PRP may be similar to those in classical PRP but with more eczematous plaques, ichthyosiform scale, especially on the lower extremities, coarse laminated palmoplantar keratoderma, and more pronounced alopecia. (see Image. Pityriasis Rubra Pilaris With Atypical Ichthyosiform Scale). Care must be taken when making this diagnosis since, clinically, it has a substantial overlap with erythrodermic mycosis fungoides, Sezary syndrome, and paraneoplastic phenomena.[34]
Type III Classic Juvenile Pityriasis Rubra Pilaris
Type III PRP comprises 10% of cases and is similar to type I classical adult PRP but has a juvenile onset and less commonly results in erythroderma. Palmoplantar keratoderma with scalp, face, and upper trunk involvement is most common.[35][36][37]
Type IV Circumscribed Juvenile Pityriasis Rubra Pilaris
Type IV PRP is the only focal variant.[35][36][37] This is the most common subtype of juvenile PRP and most commonly occurs in prepubertal children. Sharply demarcated grouped follicular papules on an erythematous base are commonly found on the extensor elbows, knees, Achilles tendon, and other bony prominences. Follicular papules may be variably scattered across other body areas. Palmoplantar keratoderma is also present.
Type V Atypical Juvenile Pityriasis Rubra Pilaris
Type V PRP is a chronic, generalized juvenile variant affecting 5% of patients. Griffiths described it in children in the first few years of life, with follicular hyperkeratosis, less prominent erythema, and occasional scleroderma-like changes of the hands. Type V PRP is sometimes used to describe all cases of inherited PRP, although others have proposed that many of these cases be recategorized as CAPE. Griffiths and others have suggested that some Type V PRP cases may represent atypical follicular ichthyosis.[38]
Type VI HIV-associated Pityriasis Rubra Pilaris
Type VI PRP occurs concurrently with HIV. Relatively few case reports have been published, so a causal association is not clear, although the relative immune dysregulation in HIV may link the two entities. PRP has been reported in individuals with both well-controlled HIV and poorly controlled HIV/AIDS. With PRP, hidradenitis suppurativa, acne conglobata, and lichen spinulosus, a follicular occlusion syndrome has also been described.[39]
CARD14-Associated Papulosquamous Eruption
CARD14-associated papulosquamous eruption (CAPE) presents in children in the first 2 years of life with a gene variation in CARD14.[26] Inheritance is autosomal dominant. CAPE may present clinically as classical psoriasis, classical PRP, or a hybrid. Erythema of the cheeks, chin, and ears is common. (see Image. Facial Pityriasis Rubra Pilaris). Sclerodermoid changes of the hands are occasionally found, as described in Griffiths type V PRP, but are not present in most individuals.
Evaluation
A complete cutaneous exam should be performed, with palpation for lymphadenopathy that might indicate malignancy and thus an alternate diagnosis, especially in adults. If present, at least 2 cutaneous biopsies are recommended to capture follicular papules or scaly erythematous plaques. PRP is diagnosed based on clinical and histopathological features. Studies have not identified serologic or immunohistochemical markers to assist in the diagnosis. Due to the rare association with HIV, screening should be considered.
Treatment / Management
The treatment of PRP can be challenging, and there are currently no US Food and Drug Administration-approved treatments. All patients may benefit symptomatically from frequently applying bland cream or ointment-based emollients daily or frequently throughout the day, as needed, for comfort and skin barrier repair. Topical corticosteroids may not always show benefit over bland emollients. However, a 2-week trial of a mid-potency topical steroid for the body and a high-potency topical steroid for the hands and feet can be tried. Keratolytic agents, such as urea, salicylic acid, or alpha-hydroxy acid-containing preparations, can be helpful for thick palmoplantar keratoderma, especially under occlusion with gloves for the hands and booties (eg, neoprene scuba socks) for the feet.
In patients with widespread PRP, a waterproof PVC or coated nylon “sauna suit” can be helpful for body temperature dysregulation, occlusion of the skin barrier, and skin dysesthesia from clothing intolerance. Bathing should be as often as tolerated; some individuals with PRP find comfort from long, tepid baths, and others cannot tolerate the feeling of water on the skin.
For patients with moderate-to-severe PRP, systemic therapy is recommended. No randomized controlled trials have been performed in PRP. Only 3 systematic open-label trials have been published; these trials studied high-dose isotretinoin, ixekizumab, and secukinumab.[22][23][40][41][40][23] In a 1982 study, isotretinoin was given to 45 adults and children with PRP at an average dose of 2.13 mg/kg/day, and 26 subjects (58%) clearly improved after 4 weeks.[41] A recent meta-analysis reported that isotretinoin is associated with a 61.1% excellent response rate.[42] However, high-dose isotretinoin is difficult to tolerate due to severe xerosis and cheilitis, myalgias, elevations in liver function tests, elevated triglycerides, and a high risk of congenital disabilities. Targeted biologics may be preferred, given the emerging role of the IL17/IL23 axis in PRP. Ixekizumab, a biologic IL17A inhibitor, was given to adults with moderate-to-severe PRP and resulted in a mean 61.3% improvement in clinical severity after 24 weeks, with no serious adverse events.[22] (A1)
In the clinician-measured Psoriasis Area and Severity Index (PASI75), 5 of 11 participants (45%) had ≥75% improvement. Similarly, secukinumab, another biologic IL17A inhibitor, was given to adults with moderate-to-severe PRP and resulted in a mean 55.6% improvement in clinical severity after 28 weeks and no serious adverse events in 6 of 11 participants with PASI75 (55%).[23] Ustekinumab has shown benefit in case series of children with CAPE.[26] Of important note, oral corticosteroids (eg, prednisone) are not effective for PRP, and this has been suggested to have diagnostic relevance since most other forms of erythroderma have at least partial improvement with oral corticosteroids.[42][43](A1)
Historically, methotrexate and acitretin have been suggested as first-line systemic therapy for PRP. While no systematic trials have been performed for these medications, systematic reviews suggest lower efficacy rates compared to the trials above. A very good response was reported to acitretin in 36% and methotrexate in 35% of patients in one review, and an excellent response was reported to oral retinoids in 42% and methotrexate in 33% of patients in another review.[43][42] The actual rates may be lower still since the data were collected from case series and case reports, increasing the risk of publication bias. Other systemic immunomodulators have been reported to benefit PRP in case reports and small case series. These include additional IL17 inhibitors brodalumab and bimekizumab; the IL23 inhibitors guselkumab, risankizumab, and tildrakizumab; the TNF-alpha inhibitors adalimumab, etanercept, and infliximab; the phosphodiesterase 4 inhibitor apremilast; and the JAK inhibitors tofacitinib and upadacitinib.[44][45][46][47][48][49][50][51][52][53](A1)
Narrow-band UVB phototherapy is rarely helpful for PRP since most patients report photo-exacerbation of their disease, but approximately 10% of patients may respond to phototherapy.[42][43] Once a patient responds to therapy and resolves the disease, treatment can be discontinued, and many patients will remain clear.(A1)
Differential Diagnosis
The differential diagnosis for PRP varies depending on the subtype and progression of the disease. PRP is generally a papulosquamous disorder with the most clinical overlap with psoriasis. Psoriasis has a rare follicular subtype that may be difficult to distinguish from PRP, although lack of palmoplantar keratoderma would be a pertinent negative finding in follicular psoriasis.[54] Additional pertinent differentials based on common PRP findings include:
- Scalp: Early scalp disease of PRP can vary from fine to larger plate-like scale, typically on an erythematous base, and may look similar to seborrheic dermatitis or allergic contact dermatitis.
- Palmoplantar keratoderma: The characteristic red-orange color and the waxy surface of classic PRP may help to distinguish it from psoriasis, acrokeratosis paraneoplastica (ie, Bazex syndrome), and mycosis fungoides.
- Erythroderma: Many inflammatory diseases become difficult to discriminate when generalized into erythroderma, including PRP, psoriasis, mycosis fungoides, Sezary syndrome, atopic dermatitis, allergic contact dermatitis, drug reactions, paraneoplastic erythroderma, and idiopathic erythroderma. The diagnosis of atypical PRP, in particular, must be used with caution since erythrodermic mycosis fungoides and Sezary syndrome may closely mimic PRP, occasionally even exhibiting characteristic islands of sparing. A pastory of an inflammatory disease may aid the diagnosis, although some individuals with PRP have a personal or family history of psoriasis. A biopsy may be helpful.
- Joint or muscle pain: Arthralgias are common in adult PRP, and true inflammatory arthritis is rare but occasionally present.[55][56] However, Wong-type dermatomyositis should be considered if patients report weakness. Wong-type dermatomyositis is a condition with cutaneous features of both PRP and dermatomyositis and systemic dermatomyositis.[57]
Prognosis
PRP is not associated with an increased risk of mortality, although the morbidity and quality of life impact are high, especially in more severe diseases.[27] In spontaneous adult-onset PRP, there is approximately a 50% rate of gradual disease resolution over months to years, with a mean time to resolution of around 3 years.[11][58] Once resolved, recurrence is rare. The remaining 50% of patients may have life-long disease. Early reports suggested that type I (classical adult onset) PRP has an 81% chance of spontaneous clearing in 3 years, whereas type II (atypical adult onset) PRP has a 20% chance.[10] However, more recent and systematic studies would suggest that this distinction is less clear, and the diagnosis of type II PRP includes the retrospective criterion of persistent disease, making it difficult to predict which patients will improve prospectively.
Early childhood onset PRP younger than 2 years is often associated with gene variations, in which case the disease is life-long. Pediatric case series of spontaneous PRP report a complete resolution rate between 43% and 80%.[35][37][59]
Complications
PRP's quality-of-life impact correlates with the severity of patient-reported symptoms and clinician-reported disease severity.[27] Palmar keratoderma leads to difficulty with fine motor skills, including difficulty using smart screens due to loss of tactile grip. Plantar keratoderma with pain and fissuring leads to difficulty walking. Cutaneous itch, pain, dysesthesia, and the need for frequent emollient application lead to difficulty wearing clothing. These factors can lead to difficulty leaving the home and challenges completing daily home and work duties.[27]
Most individuals with moderate-to-severe PRP report a strong mental health impact, including depression, anxiety, embarrassment, loneliness, loss of self-esteem, and memory loss or brain fog. In one study, the risk of passive suicidal ideation was 38% and active suicidal ideation 4% during the course of the disease. Another study reported a 7.3% suicidal ideation rate in the preceding 2 weeks in participants with PRP.[28] For those patients with complete disease resolution, complications are uncommon, although some patients report incomplete hair regrowth and a persistent feeling of memory loss or "brain fog." Cutaneous scarring is not expected.[27]
Consultations
Dermatology should be consulted expediently when PRP is suspected. Additional consultants should include ophthalmology when ectropion is present and podiatry to manage plantar keratoderma and nail dystrophy. All patients should be queried about their mental health impacts, including suicidal ideation, and offered a referral to a mental health clinician.
Deterrence and Patient Education
PRP has no clear association with lifestyle factors or other underlying health conditions. All patients should be given information about the PRP Alliance (PRPAlliance.org), a nonprofit patient-support group founded in 2013. The PRP Alliance maintains a “PRP Survival Guide” written by and for patients with PRP.
Pearls and Other Issues
Key facts that clinicians should bear in mind include:
- PRP is a cutaneous disorder diagnosed by clinical exam and cutaneous biopsy. There are no blood tests for PRP.
- PRP is rare, and all patients should be directed to the PRP Alliance (PRPAlliance.org) for patient support.
- Disease severity is associated with an increasingly negative effect on the quality of life from multiple factors, including cutaneous itch, pain, and dysesthesia; pain and decreased function of the hands and feet from palmoplantar keratoderma; and mental health impacts. All patients should be asked about suicidal ideation and offered a referral to a mental health clinician.
- There are no FDA-approved treatments for PRP. Frequent use of topical emollients is essential for comfort, and topical steroids may be tried, although they are not always helpful. Oral corticosteroids are not effective. The highest efficacy rates were reported in open-label studies of immunomodulation of the IL17 pathway using ixekizumab and secukinumab. Oral retinoids and methotrexate are also commonly used for treatment, although response rates may be lower.
- Approximately half of cases of PRP resolve within 3 years, although the range is variable, and many cases are life-long.
- There are variants of PRP with atypical presentations, but caution should be taken not to miss mimickers, especially mycosis fungoides, Sezary Syndrome, or paraneoplastic phenomena.
Enhancing Healthcare Team Outcomes
PRP is a rare, chronic skin disorder characterized by reddish-orange scaling patches, keratotic follicular papules, and palmoplantar keratoderma. The disorder may be encountered by the primary care clinician at its onset. Clinicians should recognize its distinctive clinical features, consider histopathology for confirmation, and differentiate it from other dermatoses. Because there is no laboratory test to make a diagnosis, the patient should be referred to the dermatologist for further workup. Once diagnosed, the treatment can be challenging and is usually managed by a medical dermatologist.
Based on the severity of symptoms, other care team members may include an ophthalmologist and a podiatrist. Management involves topical agents, systemic therapies, and supportive care. PRP's variable course and potential for significant impact on patients' quality of life necessitate a tailored, interprofessional approach. Regular monitoring, patient education, and adaptive therapeutic strategies are essential for optimizing outcomes in this challenging dermatological condition. All team members should be aware of the mental health impact of PRP, and patients should be regularly assessed for depression and suicidal ideation and referred to a mental health clinician as appropriate.
Media
(Click Image to Enlarge)

Pityriasis Rubra Pilaris Lesions. Characteristic lesions of PRP on a patient's hands and abdomen.
Contributed by H Ali Syed, MD
(Click Image to Enlarge)

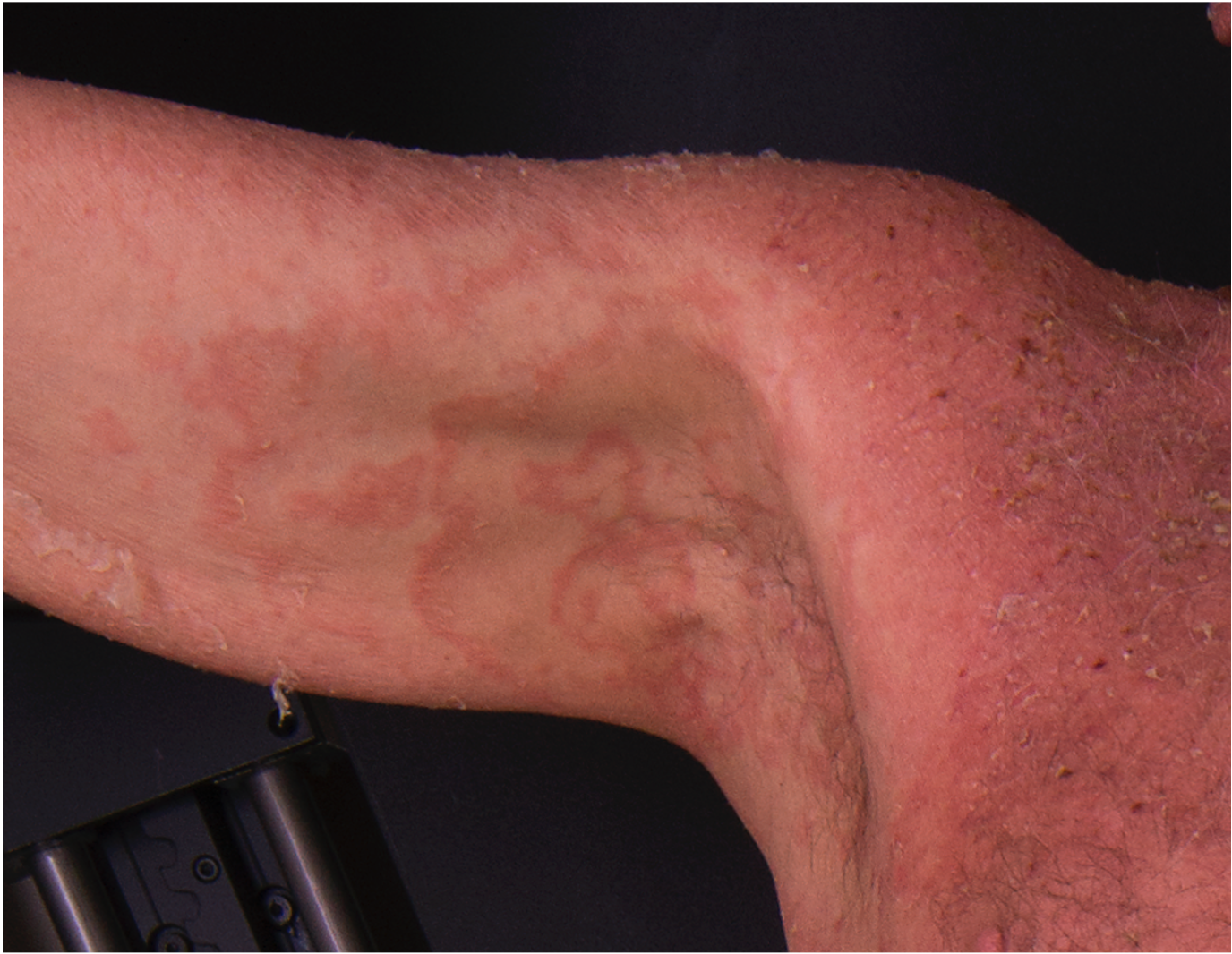
Acral Pityriasis Rubra Pilaris. Upper extremity involvement in a patient with pityriasis rubra pilaris.
Contributed by H Ali Syed, MD
(Click Image to Enlarge)

Pityriasis Rubra Pilaris With Keratoderma. PRP with waxy orange-red palmar and bright yellow plantar keratoderma.
Contributed by TM Greiling, MD
(Click Image to Enlarge)

Islands of Sparing in Pityriasis Rubra Pilaris. Characteristic bright red-orange plaques and follicular papules within islands of sparing that are frequently seen with PRP.
Contributed by TM Greiling, MD
(Click Image to Enlarge)
Pityriasis Rubra Pilaris With Erythroderma. Characteristic bright red plaques with a few islands of sparing on the lower abdomen of a patient with PRP.
Contributed by TM Greiling, MD
(Click Image to Enlarge)

Facial Pityriasis Rubra Pilaris. PRP with lateral facial involvement and thicker plate-like scale.
Contributed by TM Greiling, MD
(Click Image to Enlarge)

Pityriasis Rubra Pilaris of the Dorsal Foot. PRP with darker red-brown erythema with medium background pigment of the dorsal foot.
Contributed by TM Greiling, MD
(Click Image to Enlarge)

Severe Pityriasis Rubra Pilaris. PRP with ectropion of the lower eyelids in a patient who was asked to close their eyes as much as possible.
Contributed by TM Greiling, MD
(Click Image to Enlarge)
Gyratum-Repens-Like Pityriasis Rubra Pilaris. PRP with axillary erythema gyratum-repens-like morphology.
Contributed by TM Greiling, MD
(Click Image to Enlarge)
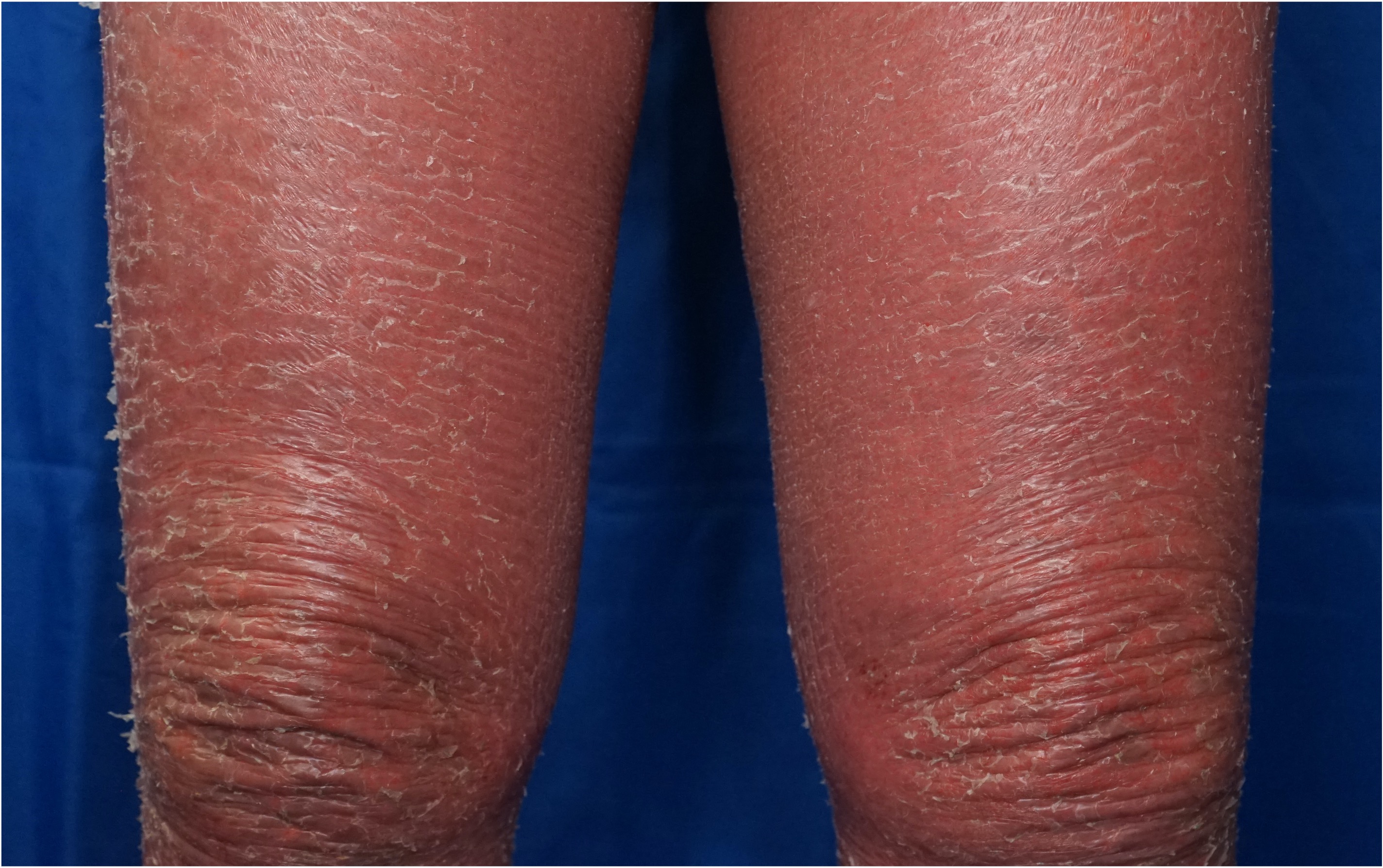
Pityriasis Rubra Pilaris With Atypical Ichthyosiform Scale. Type II PRP with eczematous plaques and ichthyosiform scale on the lower extremities.
Contributed by TM Greiling, MD
References
Aboobacker S, Harris BW, Limaiem F. Lichenification. StatPearls. 2024 Jan:(): [PubMed PMID: 30726017]
Eastham AB. Pityriasis Rubra Pilaris. JAMA dermatology. 2019 Mar 1:155(3):404. doi: 10.1001/jamadermatol.2018.5030. Epub [PubMed PMID: 30725099]
Eastham AB, Tkachenko EY, Femia AN, Pappas-Taffer LK, Rosenbach M, Joyce CJ, Liu S, Vleugels RA. Pityriasis rubra pilaris: A study evaluating patient quality of life in 2 populations. Journal of the American Academy of Dermatology. 2019 Aug:81(2):638-640. doi: 10.1016/j.jaad.2019.01.061. Epub 2019 Jan 30 [PubMed PMID: 30710600]
Level 2 (mid-level) evidenceGál B, Göblös A, Danis J, Farkas K, Sulák A, Varga E, Nagy N, Széll M, Kemény L, Bata-Csörgő Z. The management and genetic background of pityriasis rubra pilaris: a single-centre experience. Journal of the European Academy of Dermatology and Venereology : JEADV. 2019 May:33(5):944-949. doi: 10.1111/jdv.15455. Epub 2019 Mar 3 [PubMed PMID: 30697821]
Cribier B. [The very first images in the Annales de dermatologie et de syphiligraphie, 1868-1889]. Annales de dermatologie et de venereologie. 2018 Dec:145 Suppl 6():VIS63-VIS100. doi: 10.1016/S0151-9638(18)31295-X. Epub [PubMed PMID: 30598136]
Mufti A, Lytvyn Y, Maliyar K, Sachdeva M, Yeung J. Drugs associated with development of pityriasis rubra pilaris: A systematic review. Journal of the American Academy of Dermatology. 2021 Apr:84(4):1071-1081. doi: 10.1016/j.jaad.2020.07.052. Epub 2020 Jul 17 [PubMed PMID: 32687965]
Level 1 (high-level) evidenceJoshi TP, Duvic M. Pityriasis Rubra Pilaris: An Updated Review of Clinical Presentation, Etiopathogenesis, and Treatment Options. American journal of clinical dermatology. 2024 Mar:25(2):243-259. doi: 10.1007/s40257-023-00836-x. Epub 2023 Dec 30 [PubMed PMID: 38159213]
Sehgal VN, Jain MK, Mathur RP. Pityriasis rubra pilaris in Indians. The British journal of dermatology. 1989 Dec:121(6):821-2 [PubMed PMID: 2611132]
Verhagen AR, Koten JW, Chaddah VK, Patel RI. Skin diseases in Kenya. A clinical and histopathological study of 3,168 patients. Archives of dermatology. 1968 Dec:98(6):577-86 [PubMed PMID: 4235165]
Griffiths WA. Pityriasis rubra pilaris. Clinical and experimental dermatology. 1980 Mar:5(1):105-12 [PubMed PMID: 7398119]
Davidson CL Jr, Winkelmann RK, Kierland RR. Pityriasis rubra pilaris. A follow-up study of 57 patients. Archives of dermatology. 1969 Aug:100(2):175-8 [PubMed PMID: 5797957]
Fuchs-Telem D, Sarig O, van Steensel MA, Isakov O, Israeli S, Nousbeck J, Richard K, Winnepenninckx V, Vernooij M, Shomron N, Uitto J, Fleckman P, Richard G, Sprecher E. Familial pityriasis rubra pilaris is caused by mutations in CARD14. American journal of human genetics. 2012 Jul 13:91(1):163-70. doi: 10.1016/j.ajhg.2012.05.010. Epub 2012 Jun 14 [PubMed PMID: 22703878]
Li Q, Jin Chung H, Ross N, Keller M, Andrews J, Kingman J, Sarig O, Fuchs-Telem D, Sprecher E, Uitto J. Analysis of CARD14 Polymorphisms in Pityriasis Rubra Pilaris: Activation of NF-κB. The Journal of investigative dermatology. 2015 Jul:135(7):1905-1908. doi: 10.1038/jid.2015.65. Epub 2015 Mar 3 [PubMed PMID: 25734815]
Jordan CT, Cao L, Roberson ED, Pierson KC, Yang CF, Joyce CE, Ryan C, Duan S, Helms CA, Liu Y, Chen Y, McBride AA, Hwu WL, Wu JY, Chen YT, Menter A, Goldbach-Mansky R, Lowes MA, Bowcock AM. PSORS2 is due to mutations in CARD14. American journal of human genetics. 2012 May 4:90(5):784-95. doi: 10.1016/j.ajhg.2012.03.012. Epub 2012 Apr 19 [PubMed PMID: 22521418]
Haynes D, Reiter T, Velasco R, Chang M, Kulkarni R, Kent G, Strunck J, Cassidy P, Greiling TM. Pityriasis Rubra Pilaris Transcriptomics Implicate T Helper 17 Signaling and Correlate with Response to Ixekizumab, with Distinct Gene Expression Profiles in Nonresponders. The Journal of investigative dermatology. 2023 Mar:143(3):501-504.e1. doi: 10.1016/j.jid.2022.09.005. Epub 2022 Sep 24 [PubMed PMID: 36167251]
Strunck JL, Cutler B, Rajpal B, Kent G, Haynes D, Topham CA, Ortega-Loayza AG, Yang D, Wang Z, Liu Y, Cassidy P, Greiling TM. Pityriasis Rubra Pilaris Response to IL-17A Inhibition Is Associated with IL-17C and CCL20 Protein Levels. The Journal of investigative dermatology. 2022 Jan:142(1):235-239.e1. doi: 10.1016/j.jid.2021.06.009. Epub 2021 Jul 9 [PubMed PMID: 34246621]
Mellett M, Meier B, Mohanan D, Schairer R, Cheng P, Satoh TK, Kiefer B, Ospelt C, Nobbe S, Thome M, Contassot E, French LE. CARD14 Gain-of-Function Mutation Alone Is Sufficient to Drive IL-23/IL-17-Mediated Psoriasiform Skin Inflammation In Vivo. The Journal of investigative dermatology. 2018 Sep:138(9):2010-2023. doi: 10.1016/j.jid.2018.03.1525. Epub 2018 Apr 22 [PubMed PMID: 29689250]
Wang M, Zhang S, Zheng G, Huang J, Songyang Z, Zhao X, Lin X. Gain-of-Function Mutation of Card14 Leads to Spontaneous Psoriasis-like Skin Inflammation through Enhanced Keratinocyte Response to IL-17A. Immunity. 2018 Jul 17:49(1):66-79.e5. doi: 10.1016/j.immuni.2018.05.012. Epub 2018 Jul 3 [PubMed PMID: 29980436]
Shao S, Chen J, Swindell WR, Tsoi LC, Xing X, Ma F, Uppala R, Sarkar MK, Plazyo O, Billi AC, Wasikowski R, Smith KM, Honore P, Scott VE, Maverakis E, Kahlenberg JM, Wang G, Ward NL, Harms PW, Gudjonsson JE. Phospholipase A2 enzymes represent a shared pathogenic pathway in psoriasis and pityriasis rubra pilaris. JCI insight. 2021 Oct 22:6(20):. pii: e151911. doi: 10.1172/jci.insight.151911. Epub 2021 Oct 22 [PubMed PMID: 34491907]
Ghatnekar S, Shah N, Min MS, Mazori DR, LaChance AH, Vleugels RA, Nambudiri VE. Clinical features and eosinophilia in pityriasis rubra pilaris: A multicenter cohort. Journal of the American Academy of Dermatology. 2022 Apr:86(4):907-909. doi: 10.1016/j.jaad.2021.03.043. Epub 2021 Mar 24 [PubMed PMID: 33771592]
Avitan-Hersh E, Bergman R. The Incidence of Acantholysis in Pityriasis Rubra Pilaris-Histopathological Study Using Multiple-Step Sections and Clinicopathologic Correlations. The American Journal of dermatopathology. 2015 Oct:37(10):755-8. doi: 10.1097/DAD.0000000000000346. Epub [PubMed PMID: 26381023]
Haynes D, Strunck JL, Topham CA, Ortega-Loayza AG, Kent G, Cassidy PB, Hu R, Choate K, Wang Z, Liu Y, Greiling TM. Evaluation of Ixekizumab Treatment for Patients With Pityriasis Rubra Pilaris: A Single-Arm Trial. JAMA dermatology. 2020 Jun 1:156(6):668-675. doi: 10.1001/jamadermatol.2020.0932. Epub [PubMed PMID: 32293641]
Boudreaux BW, Pincelli TP, Bhullar PK, Patel MH, Brumfiel CM, Li X, Heckman MG, Pittelkow MR, Mangold AR, Sluzevich JC. Secukinumab for the treatment of adult-onset pityriasis rubra pilaris: a single-arm clinical trial with transcriptomic analysis. The British journal of dermatology. 2022 Nov:187(5):650-658. doi: 10.1111/bjd.21708. Epub 2022 Jul 15 [PubMed PMID: 35701384]
Blauvelt A, Nahass GT, Pardo RJ, Kerdel FA. Pityriasis rubra pilaris and HIV infection. Journal of the American Academy of Dermatology. 1991 May:24(5 Pt 1):703-5 [PubMed PMID: 1869640]
Misery I, Faure M, Claidy A. Pityriasis rubra pilaris and human immunodeficiency virus infection--type 6 pityriasis rubra pilaris? The British journal of dermatology. 1996 Dec:135(6):1008-9 [PubMed PMID: 8983330]
Craiglow BG, Boyden LM, Hu R, Virtanen M, Su J, Rodriguez G, McCarthy C, Luna P, Larralde M, Humphrey S, Holland KE, Hogeling M, Hidalgo-Matlock B, Ferrari B, Fernandez-Faith E, Drolet B, Cordoro KM, Bowcock AM, Antaya RJ, Ashack K, Ashack RJ, Lifton RP, Milstone LM, Paller AS, Choate KA. CARD14-associated papulosquamous eruption: A spectrum including features of psoriasis and pityriasis rubra pilaris. Journal of the American Academy of Dermatology. 2018 Sep:79(3):487-494. doi: 10.1016/j.jaad.2018.02.034. Epub 2018 Mar 1 [PubMed PMID: 29477734]
Velasco RC, Shao C, Greiling TM. Patient-reported cutaneous signs and symptoms of adult pityriasis rubra pilaris and correlation with quality of life and clinician-reported severity: A cross-sectional study. Journal of the American Academy of Dermatology. 2024 Jan:90(1):200-202. doi: 10.1016/j.jaad.2023.08.100. Epub 2023 Sep 23 [PubMed PMID: 37748557]
Level 2 (mid-level) evidenceJi-Xu A, Lei DK, Worswick S, Maloney NJ, Kim MM, Cutler L. Patient and disease characteristics associated with psychiatric symptoms and impaired quality of life in pityriasis rubra pilaris. The British journal of dermatology. 2022 Dec:187(6):1024-1026. doi: 10.1111/bjd.21792. Epub 2022 Aug 18 [PubMed PMID: 35895853]
Level 2 (mid-level) evidenceGriffiths WA. Pityriasis rubra pilaris--an historical approach. 2. Clinical features. Clinical and experimental dermatology. 1976 Mar:1(1):37-50 [PubMed PMID: 1269179]
Batra J, Gulati S, Sarangal R, Chopra D, Puri S, Kaur R. Utility of Dermoscopy in the Diagnosis of Erythroderma: A Cross-Sectional Study. Indian dermatology online journal. 2023 Nov-Dec:14(6):821-828. doi: 10.4103/idoj.idoj_678_22. Epub 2023 Oct 17 [PubMed PMID: 38099018]
Level 2 (mid-level) evidenceGleeson CM, Chan I, Griffiths WA, Bunker CB. Eruptive seborrhoeic keratoses associated with erythrodermic pityriasis rubra pilaris. Journal of the European Academy of Dermatology and Venereology : JEADV. 2009 Feb:23(2):217-8. doi: 10.1111/j.1468-3083.2008.02799.x. Epub 2008 May 13 [PubMed PMID: 18482315]
Level 3 (low-level) evidenceSahin MT, Oztürkcan S, Ermertcan AT, Saçar T, Türkdogan P. Transient eruptive seborrhoeic keratoses associated with erythrodermic pityriasis rubra pilaris. Clinical and experimental dermatology. 2004 Sep:29(5):554-5 [PubMed PMID: 15347352]
Richey PM, Fairley JA, Stone MS. Transformation from pityriasis rubra pilaris to erythema gyratum repens-like eruption without associated malignancy: A report of 2 cases. JAAD case reports. 2018 Oct:4(9):944-946. doi: 10.1016/j.jdcr.2018.07.009. Epub 2018 Oct 10 [PubMed PMID: 30345340]
Level 3 (low-level) evidenceDavis AE, Raine BE, Swartzman I, Bogner PN, Nazareth M. Rethinking pityriasis rubra pilaris as a paraneoplastic syndrome: Two cases of pityriasis rubra pilaris with concomitant underlying malignancy. JAAD case reports. 2023 Feb:32():90-95. doi: 10.1016/j.jdcr.2022.12.007. Epub 2022 Dec 27 [PubMed PMID: 36691586]
Level 3 (low-level) evidenceGelmetti C, Schiuma AA, Cerri D, Gianotti F. Pityriasis rubra pilaris in childhood: a long-term study of 29 cases. Pediatric dermatology. 1986 Dec:3(6):446-51 [PubMed PMID: 3562357]
Level 3 (low-level) evidencePiamphongsant T, Akaraphant R. Pityriasis rubra pilaris: a new proposed classification. Clinical and experimental dermatology. 1994 Mar:19(2):134-8 [PubMed PMID: 8050142]
Allison DS, El-Azhary RA, Calobrisi SD, Dicken CH. Pityriasis rubra pilaris in children. Journal of the American Academy of Dermatology. 2002 Sep:47(3):386-9 [PubMed PMID: 12196748]
Gelmetti C, Cerri D. Pityriasis rubra pilaris: the problem of its classification. Journal of the American Academy of Dermatology. 1990 Dec:23(6 Pt 1):1186-8 [PubMed PMID: 2091649]
Sánchez-Regaña M, Fuentes CG, Creus L, Salleras M, Umbert P. Pityriasis rubra pilaris and HIV infection: a part of the spectrum of HIV-associated follicular syndrome. The British journal of dermatology. 1995 Nov:133(5):818-9 [PubMed PMID: 8555047]
Shao C, Velasco R, Greiling TM. The individual Pityriasis Rubra Pilaris area and severity index (iPRPASI): validity, reliability, and responsiveness of a novel patient-reported severity tool. Archives of dermatological research. 2023 Dec:315(10):2933-2935. doi: 10.1007/s00403-023-02682-7. Epub 2023 Aug 2 [PubMed PMID: 37532946]
Goldsmith LA, Weinrich AE, Shupack J. Pityriasis rubra pilaris response to 13-cis-retinoic acid (isotretinoin). Journal of the American Academy of Dermatology. 1982 Apr:6(4 Pt 2 Suppl):710-5 [PubMed PMID: 7040513]
Kromer C, Sabat R, Celis D, Mössner R. Systemic therapies of pityriasis rubra pilaris: a systematic review. Journal der Deutschen Dermatologischen Gesellschaft = Journal of the German Society of Dermatology : JDDG. 2019 Mar:17(3):243-259. doi: 10.1111/ddg.13718. Epub 2018 Dec 6 [PubMed PMID: 30520557]
Level 1 (high-level) evidenceEngelmann C, Elsner P, Miguel D. Treatment of pityriasis rubra pilaris type I: a systematic review. European journal of dermatology : EJD. 2019 Oct 1:29(5):524-537. doi: 10.1684/ejd.2019.3641. Epub [PubMed PMID: 31789274]
Level 1 (high-level) evidenceDe Rosa A, Gambardella A, Licata G, Alfano R, Argenziano G. Successful treatment of Pityriasis rubra pilaris with brodalumab. The Australasian journal of dermatology. 2020 May:61(2):e249-e251. doi: 10.1111/ajd.13215. Epub 2019 Dec 18 [PubMed PMID: 31851372]
Saad M, Spurr A, Lipson J. Pityriasis rubra pilaris partially responsive to treatment with upadacitinib: A case report. SAGE open medical case reports. 2023:11():2050313X231160927. doi: 10.1177/2050313X231160927. Epub 2023 Mar 29 [PubMed PMID: 37009550]
Level 3 (low-level) evidenceKromer C, Schön MP, Mössner R. Bimekizumab in refractory pityriasis rubra pilaris. Journal der Deutschen Dermatologischen Gesellschaft = Journal of the German Society of Dermatology : JDDG. 2024 Jan:22(1):102-104. doi: 10.1111/ddg.15252. Epub 2023 Dec 8 [PubMed PMID: 38066410]
Pilz AC, Seiringer P, Biedermann T, Eyerich K. Treatment of Pityriasis Rubra Pilaris With Guselkumab. JAMA dermatology. 2019 Dec 1:155(12):1424-1426. doi: 10.1001/jamadermatol.2019.2774. Epub [PubMed PMID: 31577328]
Ricar J, Cetkovska P. Successful treatment of refractory extensive pityriasis rubra pilaris with risankizumab. The British journal of dermatology. 2021 May:184(5):e148. doi: 10.1111/bjd.19681. Epub 2020 Dec 4 [PubMed PMID: 33274752]
Licata G, Gambardella A, Calabrese G, Pagliuca F, Alfano R, Argenziano G. Refractory Type I pityriasis rubra pilaris treated with tildrakizumab. Clinical and experimental dermatology. 2021 Dec:46(8):1594-1595. doi: 10.1111/ced.14790. Epub 2021 Jul 14 [PubMed PMID: 34101231]
Zhang YH, Zhou Y, Ball N, Su MW, Xu JH, Zheng ZZ. Type I pityriasis rubra pilaris: upregulation of tumor necrosis factor alpha and response to adalimumab therapy. Journal of cutaneous medicine and surgery. 2010 Jul-Aug:14(4):185-8 [PubMed PMID: 20642989]
Garcovich S, Di Giampetruzzi AR, Antonelli G, Garcovich A, Didona B. Treatment of refractory adult-onset pityriasis rubra pilaris with TNF-alpha antagonists: a case series. Journal of the European Academy of Dermatology and Venereology : JEADV. 2010 Aug:24(8):881-4. doi: 10.1111/j.1468-3083.2009.03511.x. Epub 2009 Nov 30 [PubMed PMID: 20002243]
Level 2 (mid-level) evidenceKrase IZ, Cavanaugh K, Curiel-Lewandrowski C. Treatment of Refractory Pityriasis Rubra Pilaris With Novel Phosphodiesterase 4 (PDE4) Inhibitor Apremilast. JAMA dermatology. 2016 Mar:152(3):348-50. doi: 10.1001/jamadermatol.2015.3405. Epub [PubMed PMID: 26536384]
Ying Y, Yu-Hua L, Xiao-Yan W, Su-Chun H. A case of pityriasis rubra pilaris treated with tofacitinib after failure with acitretin and ixekizumab. The Australasian journal of dermatology. 2023 Aug:64(3):445-447. doi: 10.1111/ajd.14076. Epub 2023 May 18 [PubMed PMID: 37200390]
Level 3 (low-level) evidenceMagro C, Cheng E, Kline MA, Belsito DV, Goldman B, Varghese M, Crowson AN, Momtahen S. Follicular psoriasis: a report of 5 cases and review of the literature, likely an under-recognized yet distinctive variant of psoriasis. Dermatology online journal. 2020 Jul 15:26(7):. pii: 13030/qt5103211m. Epub 2020 Jul 15 [PubMed PMID: 32898397]
Level 3 (low-level) evidenceHalper K, Wright B, Maloney NJ, Kim MM, Ravi V, Worswick S, Lei DK. Characterizing Disease Features and Other Medical Diagnoses in Patients With Pityriasis Rubra Pilaris. JAMA dermatology. 2020 Dec 1:156(12):1373-1374. doi: 10.1001/jamadermatol.2020.3426. Epub [PubMed PMID: 32965475]
Conaghan PG, Sommer S, McGonagle D, Veale D, Waldmann H, Hale G, Goodfield M, Emery P, Isaacs J. The relationship between pityriasis rubra pilaris and inflammatory arthritis: case report and response of the arthritis to anti-tumor necrosis factor immunotherapy. Arthritis and rheumatism. 1999 Sep:42(9):1998-2001 [PubMed PMID: 10513817]
Level 3 (low-level) evidenceHaro R, Revelles JM, Fariña Mdel C, Martín L, Requena L. Wong's dermatomyositis: a new case and review of the literature. International journal of dermatology. 2013 Apr:52(4):466-70. doi: 10.1111/j.1365-4632.2011.05244.x. Epub 2012 Dec 11 [PubMed PMID: 23230970]
Level 3 (low-level) evidenceRoss NA, Chung HJ, Li Q, Andrews JP, Keller MS, Uitto J. Epidemiologic, Clinicopathologic, Diagnostic, and Management Challenges of Pityriasis Rubra Pilaris: A Case Series of 100 Patients. JAMA dermatology. 2016 Jun 1:152(6):670-5. doi: 10.1001/jamadermatol.2016.0091. Epub [PubMed PMID: 26963004]
Level 2 (mid-level) evidenceYang CC, Shih IH, Lin WL, Yu YS, Chiu HC, Huang PH, Cheng YW, Lee JY, Chen W. Juvenile pityriasis rubra pilaris: report of 28 cases in Taiwan. Journal of the American Academy of Dermatology. 2008 Dec:59(6):943-8. doi: 10.1016/j.jaad.2008.07.054. Epub 2008 Sep 25 [PubMed PMID: 18819727]
Level 3 (low-level) evidence